
Abstract
Objective
Sleep pattern at high altitude has been studied, mainly with the use of polysomnography. This study aimed to analyze subjective sleep quality at high altitude using the following standardized scales: the Pittsburgh Sleep Quality Index (PSQI) and the Athens Insomnia Scale (AIS-8).
Methods
Thirty-two members of 2 expeditions—28 males and 4 females (mean age 31 years)—participated in this study conducted in Nepal, Himalayas (Lobuche East, 6119 m above sea level [masl]), Kyrgyzstan, Pamirs (Lenin Peak, 7134 masl), and Poland (sea level). The scales were administered twice, at high altitude (mean altitude 4524 masl) and at sea level.
Results
Both measures showed a decrease in sleep quality at high altitude (statistical significance, P < .001). Sleep problems affected general sleep quality and sleep induction. Sleep disturbances due to awakenings during the night, temperature-related discomfort, and breathing difficulties were reported. High altitude had no statistically significant effect on sleep duration or daytime dysfunction as measured by PSQI.
Conclusions
The overall results of PSQI and AIS-8 confirm the data based on the climbers’ subjective accounts and polysomnographic results reported in previous studies. The introduction of standardized methods of subjective sleep quality assessment might resolve the problem of being able to perform precise evaluations and research in the field of sleep disturbances at high altitude.
Introduction
Sleep, which constitutes one third of a lifetime, is significantly affected by high-altitude environment. 1 Poor-quality sleep may provoke emotional instability, disturbed cognitive functioning, 2 and high-altitude daytime dysfunction. 3 The main cause of reduced quality sleep at high altitude seems to be hypobaric hypoxia due to decrease in the partial pressure of oxygen with rising altitude. Sleep quality improvement with a decrease in altitude 4 and application of supplementary oxygen 5 might confirm the dominant role of hypobaric hypoxia. Other factors affecting sleep quality may be a fall in the air temperature 6 and the season of the year. 7 Poor nocturnal sleep may induce sleepiness during the day. 8
From the first descriptions of a decrease in the quality of sleep in hypobaric hypoxia conditions provided by West et al 1 and Barcroft 9 there has been significant development of objective sleep quality measures, such as polysomnography, that have been used in high-altitude field research and that have enabled further insight into sleep patterns at high altitude. 10 –12 At high altitude there is a shift in sleep stage distribution, with a prevalence of the lighter non–rapid eye movement (NREM) sleep stages I and II and almost complete elimination of the deeper NREM stages III and IV. 13 Rapid eye movement sleep period is of variable duration, and an increased frequency of brief arousals at high altitude is connected with the appearance of periodic breathing during NREM. 13
Such objective data about the changes in sleep at high altitude are supported by a subjective decrease in the quality of sleep. Trekkers and alpinists complain about the superficiality of sleep, problems with sleep induction, incidents of awakening with a sense of suffocation and about feeling unrefreshed in the morning. 1 The current literature, however, is lacking in standardized subjective sleep quality measures at high altitude, apart from the work of Pedlar et al, 14 who used the Leeds Sleep Evaluation Questionnaire (LSEQ) in the conditions of normobaric hypoxia. Conclusions are often based on climbers’ personal accounts 1 and nonstandardized ratings of separate aspects of sleep quality.5,15 This does not allow for duplication of methods or extrapolation of results, and it provides insufficient information about different aspects of sleep quality.
The aim of our study was to evaluate the subjective quality of sleep at high altitude using reliable, standardized scales: the Pittsburgh Sleep Quality Index (PSQI) 16 and the Athens Insomnia Scale (AIS-8), 17 which have been validated at sea level. The introduction of such standardized methods of assessment of subjective sleep quality might facilitate future research in the field of sleep disturbances at high altitude.
Methods
Volunteers included 38 healthy Caucasian adults, 34 men and 4 women, with a mean age of 31 ± 9 years (range 19–55 years), who were the participants in 2 mountaineering expeditions (Lobuche East, 6119 m above sea level [masl], Himalayas, Nepal; and Lenin Peak, 7134 masl, Pamirs, Kyrgyzstan). All volunteers gave informed consent to participate in the study, which was approved by the Medical University of Gdansk Regional Ethics Committee. The participants were asked to refrain from taking any medications that could enhance acclimatization or alter quality of sleep. Question No. 6 in PSQI asks about using any sleeping medications. Participants were asked to write the name and dose of any medication used during the research period.
Modified versions of PSQI and AIS-8 were used in the study. The assessment of subjective sleep quality was performed twice in each volunteer—first at high altitude during the expedition and later at sea level after the expedition. Sleep time was habitual. The assessment at high altitude was conducted on average 9 ± 3 days after beginning the high-altitude sojourn (at an altitude over 2500 masl), at an average altitude of 4329 ± 218 masl. The assessment at sea level was performed on average 57 ± 31 days after the end of the expedition.
The PSQI consists of 19 self-rated questions designed to assess 7 components of sleep quality: subjective sleep quality (C1), sleep latency (C2), sleep duration (C3), habitual sleep efficiency (C4), sleep disturbances (C5), use of sleeping medication (C6), and daytime dysfunction (C7). Each component is scored on a scale ranging from 0 to 3, and the global score has a possible range of 0 to 21 points, where higher scores indicate a greater decrease in the quality of sleep. Results measuring over 5 indicate poor sleep quality (poor sleepers). As a result of the study conditions, the PSQI was modified in such a manner that participants rated their sleep quality during the past week, not the past month, as in the original version. The reliability of PSQI was found to be satisfactory at sea level (Cronbach's α = 0.83). 16
The AIS-8 consists of 8 items assessing the following: 1, sleep induction; 2, awakening during the night; 3, final awakening; 4, total sleep duration; 5, sleep quality; 6, well-being during the day; 7, functioning capacity during the day; and 8, sleepiness during the day. Each item is scored from 0 to 3, and the total score ranges from 0 to 24, where higher scores indicate greater sleep impairment. Participants considered their past week in the sleep quality assessment. A result of ≥6 indicates insomnia (insomniacs). The reliability of AIS-8 was found to be satisfactory at sea level (Cronbach's α = 0.89). 17
The PSQI is based mainly on the quantitative questions that have to be answered using concrete units (minutes, hours) or on the frequency of occurrence of specific problems affecting sleep quality (eg, the number of awakenings because of respiratory problems). Questions used in the AIS-8 refer to the subjective perception of sleep problems. For instance, sleep duration is not computed in hours, as in the PSQI, but rather the participant is asked whether it was sufficient or not. The AIS-8 seems to rely more on the individual perception of the sleep quality than does the PSQI. As early reports 1 underline the discrepancy between qualitative and quantitative accounts of sleep problems, both of these types of account were included in our research design.
Statistical analysis of the results was based on Cronbach's internal consistency reliability coefficient for all the scales. The difference between results of the PSQI and AIS-8 at sea level and at high altitude was analyzed using the nonparametric Bonferroni-adjusted Wilcoxon rank test (z) to account for multiple comparisons. SPSS 12.0 for Windows was used as a statistical program.
Results
Six participants were excluded from the study because they used medications such as Diuramid (acetazolamide, ZF Polpharma SA, Starogard Gdanski, Poland) and Stilnox (zolpidem, Synthelabo, Paris, France), which could alter their acclimatization and sleep quality. Eventually 32 participants, 28 men and 4 women (mean age 31 ± 9 years; range, 19–55 years), qualified for subsequent analysis. The results of the PSQI and AIS-8 were analyzed to assess the subjective sleep quality during a week at the mean altitude of 4524 ± 451 masl.
Based on their PSQI score, 17 participants (53%) were identified as poor sleepers at high attitude, while according to the AIS-8 cutoff score, there were 15 (47%) insomniacs. Two participants were diagnosed as poor sleepers according to their PSQI scores at sea level, and there were no insomniacs according to AIS-8 results at sea level. The PSQI and AIS-8 internal consistencies at high altitude were found to be high (Cronbach's α = 0.73 [computed without C6] and α = 0.69, respectively).
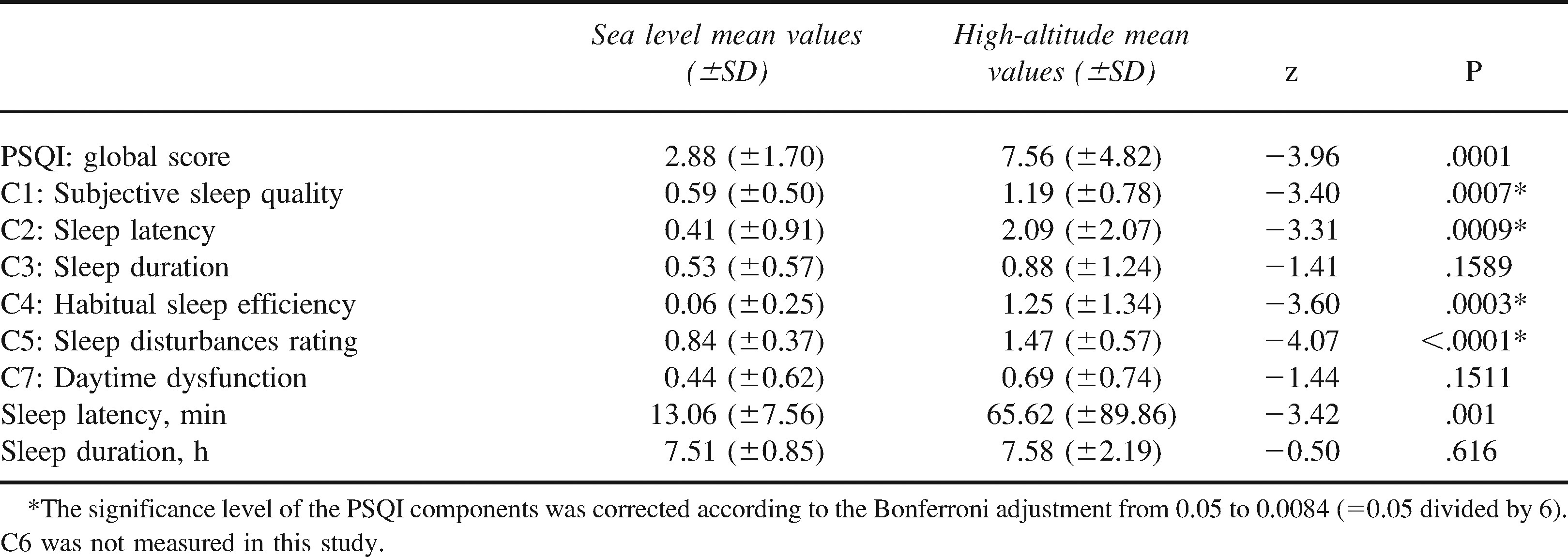
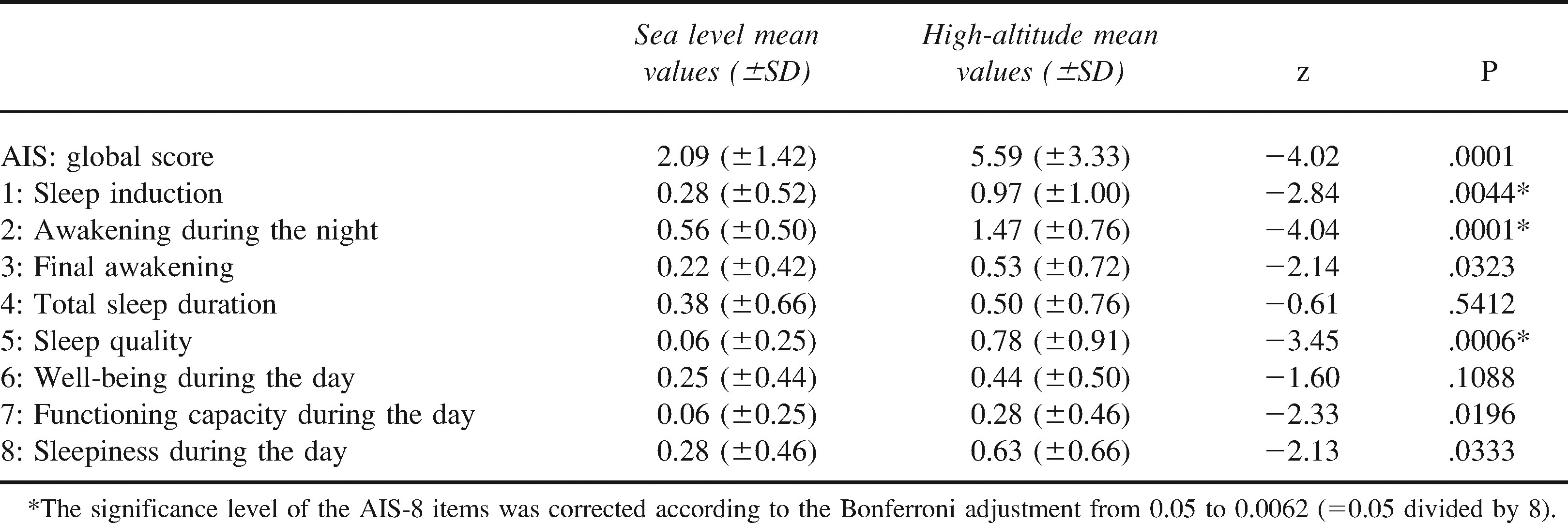
According to the PSQI and AIS-8 results there was a statistically significant decrease in the subjective quality of sleep at high altitude (see Tables 1 and 2). According to the PSQI, sleep quality averaged 2.9 ± 1.7 at sea level and 7.6 ± 4.8 at high altitude. The difference was statistically significant (z = −4.0, P < .001). Similarly, sleep quality measured by AIS-8 was poorer at high altitude (5.6 ± 3.3) than at sea level (2.1 ± 1.4) (z = −4.0, P < .001).
Pittsburgh Sleep Quality Index (PSQI) results at sea level and at high altitude
Athens Insomnia Scale (AIS-8) results at sea level and at high altitude
Significant differences were noted in the following PSQI subscales: C1, subjective sleep quality; C2, sleep latency; C4, habitual sleep efficiency; and C5, sleep disturbances. Reported sleep latency increased by almost 1 hour at high altitude. There were no significant changes observed for C3 (sleep duration) or C7 (daytime dysfunction or sleep duration in hours). As individuals using sleeping medications were excluded from the trial we could not estimate the role of this factor in the subjective quality of sleep.
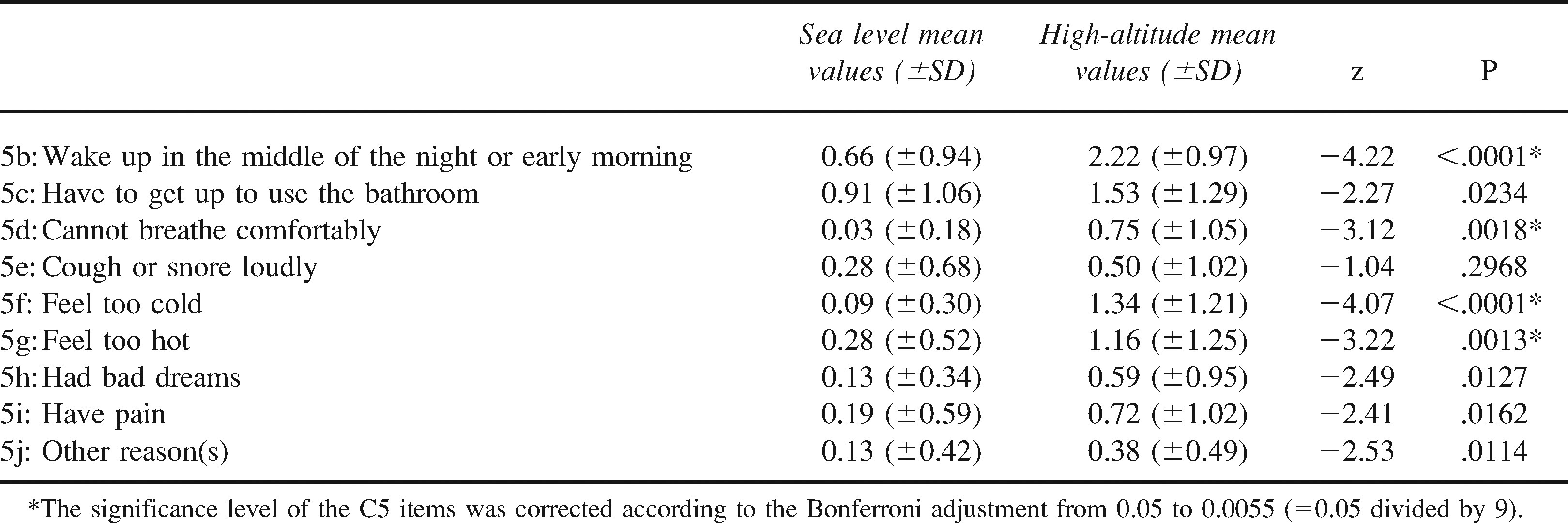
Among the items from the component C5 (sleep disturbances): 5b, wake up in the middle of the night or early morning; 5d, cannot breathe comfortably; 5f, feel too cold; and 5g, feel too hot, were significantly altered at high altitude (see Table 3).
Items from C5—sleep disturbances of the Pittsburgh Sleep Quality Index (PSQI) at sea level and at high altitude
Significant differences were noted in the following AIS-8 items: 1, sleep induction; 2, awakening during the night; and 5, sleep quality. There were no significant differences observed for 3, final awakening; 4, total sleep duration; 6, well-being during the day; 7, functioning capacity during the day; and 8, sleepiness during the day.
Average time spent in bed at sea level was 8.0 ± 1.0 hours (range 6–10 hours), while at high altitude, this measure was 10 hours 16 minutes ± 1 hour 36 minutes (range 6–13 hours). Time spent in bed was significantly increased at high altitude (z = −4.45, P < .001). Average time of going to bed at sea level was 11:40
Discussion
In accordance with previous studies reviewed by Weil, 13 sleep quality significantly decreased at high altitude. In our study the sleep problems confirmed by PSQI and AIS-8 were due to poor sleep quality in general, longer periods of sleep induction, and incidents of sleep disturbances that provoked awakening during the night. West et al 1 and Anholm et al 12 found similar results based on personal sleep quality accounts of the participants of the study. Feeling of sleeplessness was also observed by Barcroft 9 and by Reite et al 11 in a group study. Luks et al 5 used a nonstandardized questionnaire assessing sleep quality and reached the same conclusions.
Fragmentation of sleep as a result of increased number of arousals and periodic breathing observed via polysomnography by other researchers4,11–13,18 might explain the subjective feeling of sleep disturbances and awakening during the night. Fragmentation of sleep might be the main reason for the poor quality of sleep.4,13 The shift of sleep stages in NREM toward the lighter sleep stages I and II 13 might, to some extent, explain the superficiality of sleep and overall decrease in sleep quality. Pedlar et al 14 did not observe decrease of subjective sleep quality measured by LSEQ after 1 night spent in a normobaric hypoxic tent, which might be explained by the fact that there were no differences in sleep stages III and IV between normoxic and normobaric hypoxic conditions observed in the same study. In our work, sleep disturbances were mostly due to awakening in the middle of the night or early morning, breathing problems, and feeling too hot or too cold (PSQI). Weil 13 also observed that nighttime awakenings are connected with a sense of suffocation. In our study, sleep disturbances were not connected with having continuous or intermittent bad dreaming, as mentioned by Barcroft 9 and West et al. 1
The considerably longer period required for sleep induction observed in our work may be partially explained by the fact that at high altitude volunteers went to bed almost 3.5 hours earlier than they did at sea level. Contrary to our results, 1 night spent in the normobaric hypoxic tent simulating an altitude of 2500 masl resulted in no changes in the getting-to-sleep parameter measured by LSEQ. 14 We have found no polysomnographic data concerning sleep induction period at high altitude, apart from the work of Beaumont et al, 19 who, in contrast to us, observed a significant decrease in sleep onset latency—the time from “lights out” to the first episode of sleep stage II, at a simulated altitude of 4000 m.
Weil 13 and Netzer and Strohl 4 noted the absence of total sleep time changes at high altitude in polysomnography studies. No reduction was also observed in our study; thus, subjective sleep quality seems not to depend on total sleep time changes. However, a decrease of total sleep time was observed in a hypobaric chamber study. 12 We observed a reduction in habitual sleep efficiency (ie, total sleep time to time spent in bed), possibly caused by the increased time spent in bed—over 2 hours longer than at sea level. The AIS-8 showed that final awakening period problems do not influence sleep quality. The time of getting up in the morning, which was over 1 hour earlier at high altitude, does not provoke sleep impairment. According to our results, alpinists seem to go to bed and get up earlier during the high-altitude sojourn, which might be explained by the change of the daytime profile of activities and the accommodation conditions of the expedition or trekking.
Daytime functioning was not altered by the poor quality of sleep in our study, in contrast to the findings of West et al 1 and Bonnet and Arand 20 but in accordance with the neuropsychological studies done by Luks et al. 5
It seems that subjective and objective changes in sleep quality in hypoxic conditions might depend on the duration and level of hypoxia. One night spent in the normobaric hypoxic tent simulating an altitude of 2500 masl resulted in a significant increase in respiratory disturbances without changes in sleep stages and had no impact on subjective quality-of-sleep and getting-to-sleep parameters. 14 The only subjective disturbance observed in the study of Pedlar et al 14 was feeling of residual tiredness measured by LSEQ.
Our study has certain limitations. We did not study the sleep quality prior to the expedition. The main reason for performing postascent and not pre-ascent sea level measurements was our lack of opportunity to meet all the participants and to explain to them the examination procedure before the expedition. The polysomnography measurements done by Netzer and Strohl 4 indicate that high-altitude poor quality of sleep does not affect the quality of sleep at sea level after the high-altitude sojourn. The objective quality of sleep at sea level before and after the high-altitude sojourn remains the same. In light of those facts, sleep quality after the expedition as a measure in our study should have been comparable to the sleep quality of the participants before the expedition. The period between the end of the high-altitude sojourn and the assessment done at sea level, which is not the same for all participants, should also not have had an effect on the obtained data. The average time of sea level measurement was 1 month after the expedition. The differences in timing were due to the time at which the postascent questionnaires were received from participants.
There are some differences of timing in the high-altitude measurements as a result of individual changes in the ascent profile. Trekkers or alpinists rarely follow exactly the same ascent profile, even on the same mountain trail. The aim of the study was to perform the high-altitude measurement in the early phase of acclimatization after a first week spent at an average of 4500 masl.
The results of our study show that the psychometric values of PSQI and AIS-8 are satisfactory, regardless of the fact that reliability coefficients were lower than in the original validation studies16,17,21,22 conducted at sea level. The reason for this discrepancy could be differences in health status, size of the examined group, and specificity of the sleep problems at high altitude.
Modifying the assessment period of PSQI from 1 month to 1 week might have affected the tool's sensitivity. This modification seems indispensable in the reality of high-altitude expeditions, durations of which are less than 1 month, and where early sleep evaluation is essential. The estimate period was also reduced to 1 week in the PSQI reliability and validity analysis for cancer patients 23 and to 2 weeks for insomnia patients. 24
Psychometric evaluation of subjective quality of sleep at high altitude should consist not only of a reliability analysis but also of a validity analysis. Unfortunately, we did not have resources to perform polysomnography or actigraphy studies in the examined group. The lack of any subjective sleep quality scale that had been validated and standardized in the high-altitude conditions precluded the validation of the PSQI and AIS-8.
The scales used in our study did not contain any questions concerning how refreshed the volunteer felt in the morning, so feelings of being less refreshed in the morning mentioned in other studies1,5,12,14 cannot be confirmed by our results.
Apart from the fact that the PSQI is compatible with polysomnography results, 16 it should be noted that polysomnography and subjective sleep quality measures may also detect different aspects of sleep experience. The former concentrates on the sleep stages, not on the subjective sleep components. 25 Those 2 assessment strategies complement each other. However, considering the fact that polysomnography studies are expensive and labor intensive, which results in small sample sizes, standardized methods such as the PSQI and AIS-8 might offer a good, practical alternative.
In future studies, it is worth considering actigraphy as an “objective” adjunct to subjective sleep quality measures. Actigraphy is not as accurate as polysomnography but is more reliable than sleep logs and can be used in conditions that prove too cumbersome for polysomnography.26,27
Our study confirms the utility of subjective sleep quality scales at high altitude as research and diagnostic tools, tools that could also be used to estimate the effectiveness of sleep therapy, as is done at sea level.25,28
As a result of its compact form, ease of administration, scoring system, and optional period of assessment, the AIS-8 seems to be more user friendly, and therefore we would recommend its use to expedition doctors. As a more detailed and mainly quantitative questionnaire, the PSQI might be recommended for clinical trials and scientific research. The fact that some of its components consist of specific items may offer further insight into the underlying cause of sleep disturbances.
We conclude that subjective sleep quality decreases at high altitude. The introduction of standardized methods of subjective sleep quality assessment might enhance precise evaluation and research in the field of sleep disturbances at high altitude.
Footnotes
Acknowledgments
Arfan M. Sheikh, BSc, is acknowledged for language editing of the English version of the article.
*
The work was presented as a poster during Mountain & Wilderness Medicine World Congress, Aviemore, Scotland, October 3–7, 2007.
**
The work is attributed to Clinical Department of Emergency Medicine, Medical University of Gdańsk, Poland. The research was not supported financially.