
Abstract
This Lessons from History article uses science, aviation, medicine, and mountaineering sources to describe some of the effects of hypoxia, illumination, and other environmental conditions on the eye, the central nervous system, and light and color perception. The historical perspective is augmented by an analysis of an informal observation of the altered perception of red color on a deck of playing cards while climbing Mera Peak in the Himalaya. The appearance of a grayer red color on the cards was initially attributed to the effects of hypoxia alone. Instead, analysis of cards in combination with the low incidence of protan color vision defects at altitude indicated that glare and contrast effects in the extremely bright lighting environment combined with hypoxia likely caused the perception of a grayer red. The incident provides an educational opportunity for review, analysis, and commentary about some of the complex elements that impact color vision.
Introduction
Vision is critical for safe mountaineering; however, the environment at high altitudes can damage various ocular structures through exposure to intense levels of sunlight or hypobaria and hypoxia. 1 -3 Visual function is also impaired by hypoxia without obvious damage to the ocular tissues. Mild or moderate hypoxia can compromise dark adaptation, peripheral visual fields (ie, tunnel vision), contrast sensitivity at lower light levels, and color vision. 4 -6 An altered perception of playing cards by 4 members of a Himalayan expedition provides an opportunity to review some of the history and physiology of vision at high altitudes emphasizing color vision. Although this informal observation was not a preplanned scientific venture, the review and subsequent analysis of the cards’ contrast and color provide insight into how hypoxia and other environmental factors, such as glare, could have contributed to the altered color perception.
Color Vision in the Mountains: Mera La
On the way to Mera Peak (Himalaya, Nepal), the expedition party, including one of the authors (HVL), camped on the Mera La (pass) at 5400 m, where the partial pressure of oxygen is half the sea level value. The camp was reached over 9 d and within staged-ascent guidelines to allow for partial acclimatization to reduce the risk of high altitude illnesses. 7 No one had acute mountain sickness (AMS), high altitude cerebral edema, or high altitude pulmonary edema. The card game of Crazy Eights had been played at lower altitudes, including the previous evening at 4900 m illuminated by a kerosene lamp. However, the observation occurred the next day after reaching Mera La and playing cards for approximately 1 h. The site was outside on lightly colored crushed rock and snow adjacent to the white ice-sloped edge of the Mera glacier in the early afternoon sun. In this extremely high glare setting, one of the foursome suddenly exclaimed that the red cards were “missing.” Incredulous, the other 3 members promptly agreed that red suits appeared almost gray. Figure 1 shows a sample of the original cards with a simulation of the altered perception. Until this surprising observation, the players had not noticed that the red color on the cards seemed lackluster and not as distinct as usual from the black cards, nor had they noticed any decrement in card playing performance. The hasty consensus of the group was that the altered color perception was solely hypoxia related. Unfazed, the group continued the game without apparent difficulties, possibly relying on the suit’s shape difference. The team climbed higher later in the expedition, but Mera La was the highest altitude for card playing because of adverse environmental conditions.
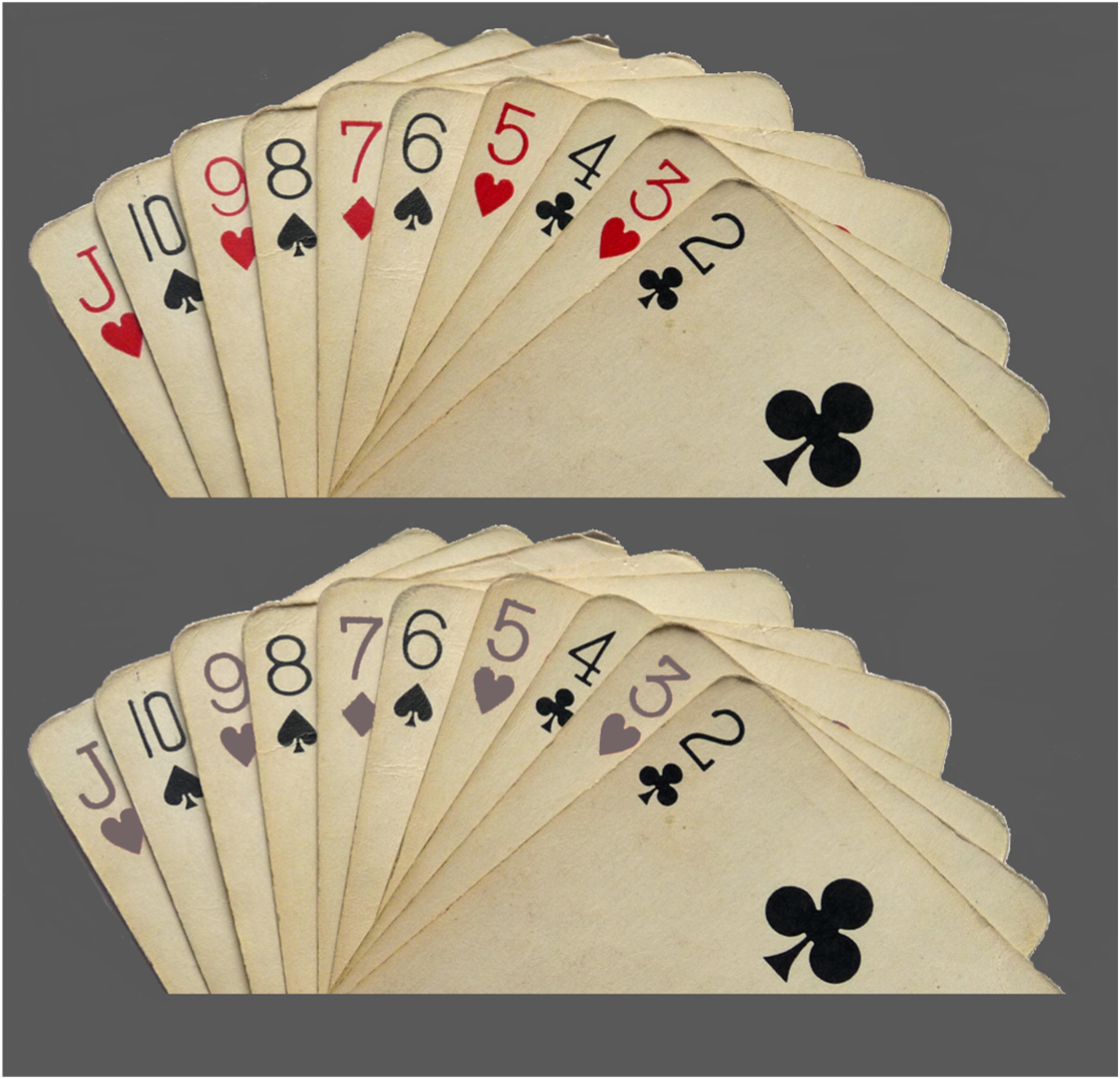
Photograph of sample cards from the expedition (upper image) taken with a Lumix DMC-TZ5 camera (Panasonic, Kadoma, Japan). The lower portion was altered based on the first author’s recollection using Photoshop (ver 12.0.4; Adobe Systems Incorporated, San Jose, CA) to simulate the observation at 5400 m in the Himalaya.
The remainder of the essay is organized into overlapping discussions on color vision, physiology, the effects of hypoxia, historical vignettes of people and observations, and color vision studies on other mountains. It concludes with our analysis of the cards using filters to simulate color vision deficiencies that suggest the expedition’s rash conclusion that hypoxia was the sole cause of the altered perception was incorrect. Another environmental factor, disability glare, could have reduced the color contrast and been a contributing factor.
Vision
Light is electromagnetic energy that creates a visual sensation without damaging the eye. By itself, radiant energy has no color. That is, color is not a physical property. Color perception can only occur through the complex translation of the radiant energy into neural impulses, starting with the absorption of light by the photoreceptors. The human eye contains at least 3 types of photoreceptors: rods, cones, and a comparatively few intrinsically photosensitive retinal ganglion cells. The intrinsically photosensitive retinal ganglion cells are involved in nonvisual functions, such as circadian rhythm, and will not be discussed in this article. Rods mediate peripheral vision in low-light environments, which are equivalent to illumination by a quarter moon. This is synonymous with night vision or scotopic vision. Rods cannot resolve fine detail or mediate color vision, so objects appear as low-resolution gray-scale images. Cones mainly mediate during daytime or at illumination levels comparable to hallway illumination or brighter. This is known as photopic vision. Cones are found throughout the retina, with the highest concentration in the central area known as the fovea, the area of sharpest vision. Outside of the fovea, cone density rapidly decreases as the proportion of rods increases. 8 -10 As with the rest of the retina and central nervous system, rods and cones are highly metabolically active and sensitive to hypoxia. Oxygen consumption increases as light levels fall for both photoreceptors, although the increase appears larger for rods. 10 -12 The idea that a scotopic system is mediated by rods and a photopic one is based on cones is called the duplex theory of vision and is consistent with the 1866 Duplicity Theory of German anatomist Max Schultze.8,13 However, rods and cones mediate vision together without abrupt transition in dim light. This range is known as mesopic vision and is equivalent to street lighting at night.
The realization that the wavelengths of light have no color by themselves is attributed to Sir Isaac Newton. His treatise Opticks in 1704 overturned many ancient ideas about visual perception. 14 The roots of modern color vision theories lie in the Young-Helmholtz trichromatic theory and the Hering opponent colors theory.15,16 The visual signal starts with the absorption of photons by the cone photoreceptors, beginning a process called visual phototransduction, which turns energy into neural impulses. There are 3 types of cones labeled by the wavelength range to which they are maximally sensitive: short (S), medium (M), or long (L). There is substantial overlap in the wavelengths to which the cones respond and some individual variation in the location of the peak absorption of the cone photopigments. The cone signals are processed at multiple levels within the retina and the visual cortex.8,10,11,17 In the basic model of color perception, there are 2 chromatic channels. The blue-yellow channel compares the S-cone response with the sum of the L- and M-cone responses to signal either blueness or yellowness. The red-green channel compares the sum of the S- and L-cone responses with the M-cone response to signal either redness or greenness. The third channel is an achromatic channel, which sums the L- and M-cone responses and provides black/white information. Blackness is perceived when the surrounding area is brighter than the object of regard. 18 More complex theories try to model how the observer’s interpretation of context and memory influences the final perception through interactions with other cortical areas.19,20
The loss in color discrimination due to hypoxia often resembles the loss associated with congenital color vision deficiencies. Congenital color vision deficiencies are classified based on which cone photopigment is altered. Individuals with a deutan deficiency have an altered M-cone photopigment, and protan individuals have an altered L-cone photopigment. Many colors confused by protan individuals are similar to those confused by deutan individuals (eg, orange, yellow, and green; dark green, brown, and red); hence, these are referred to as red-green color vision deficiencies. 21 Two major differences between these 2 subtypes are that deutans have normal brightness sensitivity to red light, but protans have decreased brightness sensitivity to red light, and protans confuse red with gray, whereas deutans do not confuse these 2 colors. A tritan defect occurs when the S-cone function is impaired. 22 Individuals with a tritan defect typically confuse violet, gray, and yellow-green with each other; blue with blue-green; blue-green with a bluish-white; and navy blue with black. This defect is also referred to as a blue-yellow color vision deficiency. Although the hypoxia-related color vision defects resemble receptor-based congenital color vision defects, it is unlikely that the defects result from changes at the photopigment level of the cones. Previous studies have shown that the cone signals are largely unaffected by hypoxia. Instead, it has been hypothesized that the site of the hypoxia-related defect is located early in the retinal processes, perhaps where the cone signals are first combined into the postreceptor channels.6,23-25
Altitude Effects
Reports on mountain climbing to extreme altitude appeared in ancient writings by the Chinese, in the 16th century by the Spanish in South America, and beginning in the mid to late 19th century by other Europeans. 26 -30 The symptoms described are identified today as part of AMS and high altitude deterioration, but it is unclear if visual changes were recognized. One of the earliest reports on vision changes from hypoxia at an extreme altitude that probably exceeded 8840 m was in 1862 by English balloonist James Glaisher. He creatively described the effect on his vision before becoming unconscious: “In an instant intense darkness overcame me, so that the optic nerve lost power suddenly.” He later concluded, “I thought I had been seized with asphyxia.” 31
Paul Bert (1833–86), the father of high altitude physiology, performed barometric chamber studies to reveal that low partial pressure of oxygen caused physiological impairment. 32 Bert’s book included anecdotes of other travelers’ vision at high or extreme altitude. Several accounts were metaphorical, but others portrayed some of the real effects of hypoxia: “lost power of vision,” “disturbances of vision,” and “dimness of vision.” 32 During hypobaric chamber studies, Bert observed not only dull vision from hypoxia but brightening of vision with supplemental oxygen. One subject “resorted to oxygen because he could hardly see his paper, which at the first inhalation appeared to him very white, as if he were dazzled.” 32
In 1919, British respiratory physiologist John Scott Haldane (1860–1936) performed hypobaric chamber studies on himself and others, including Scottish Himalayan explorer Alexander Kellas. Haldane noted, “On taking two or three breaths of oxygen, the light suddenly became brighter to all of us” and, just as important, “On raising the pressure rapidly, the same brightening of light was observed.” 33 Notably, either supplemental oxygen or raised air pressure benefited vision.
C. Raymond Greene (1901–82) was a British medical officer on the 1931 expedition that summited Kamet (7756 m) and the 1933 Everest expedition. 34 -36 Before the Everest expedition, he had consulted Haldane and spent hours in the Oxford hypobaric chamber.33,35,37,38 Greene described Haldane’s eureka moment: “The electric light glowed suddenly more brightly. At first, he [Haldane] thought the current had been increased, but later realized that the change was in himself and not in the current.”35,38 Greene also contributed 2 related observations about hypoxia in the medical chapter of Kamet Conquered in this single sentence: “The special senses at great altitudes are frequently blunted, although this change was not noticed by the majority of the expedition.” 35 On Everest, Greene found cylinders from George Finch’s 1922 campsite at 7650 m and “took a swig of oxygen. The first effect was a sudden increase in the light intensity. I saw more sharply, and colours became brighter.” 33 -35 Greene also reported improved vision with higher atmospheric pressure. Descending to 5030 m on Kamet, he noticed, “For me, shut in no steel chamber… I began once more to appreciate the pleasures of the senses…The snow was whiter and more scintillating.”34,38
It is not necessary to go to extreme altitudes to affect vision. At 2438 m, the threshold for high altitude illnesses, arterial oxyhemoglobin concentration drops to approximately 93%, resulting in mild hypoxia and a measurable decline in visual function. Aviation medicine has long known that hypoxia affects night vision at an altitude as low as 1524 m. The US Federal Aviation Administration suggests using supplemental oxygen in unpressurized aircraft for flying at night above 1828 m and during daytime above 3048 to 4267 m depending on the aircraft type and flight duration. The degree of color vision loss produced by mild hypoxia at these daytime altitudes is similar to a slight reduction in retinal illuminance. With increasing altitude, an aviator’s perceptual and cognitive skills are further impaired, and this impairment dramatically accelerates at extreme altitudes, usually defined as above 5486 m. Hypoxic cerebral and visual symptoms at any threshold level are often rapid for aviators and prolonged for mountaineers, with important differences in presentation.30,39-43
Color Vision Studies in the Mountains
In the mountains, vision is needed to get up or down safely. Color discrimination is valuable to the mountaineer for using handheld navigational devices and reading maps, color-coded supply labels, and computer displays. Color vision is important in identifying colored marker flags or recognizing people’s clothing. Even a tent may have its color misidentified. 44 It could be catastrophic to seek the wrong tent for life-saving shelter, supplemental oxygen, fuel, or food. Aviators assisting the expedition must avoid catastrophe by relying on colored digital cockpit displays, navigational aids, and external visual clues. Interpreting visual information correctly is especially critical at night and during hazardous helicopter operations.
Despite the importance, color vision studies in high mountains have been infrequent compared with those of other medical studies. Testing color vision is challenging because of the limitations of the test selected for the study, varying lighting conditions, acclimatization, and more. Acknowledging these constraints, the following section reviews the few available color vision studies on mountains at altitudes comparable to or higher than Mera La.
Studies were performed on Mount Agri (Ararat) at 4200 m in Turkey; on Ama Dablam (Himalaya) at 1300, 4000, and 5400 m; on Cho Oyo (Himalaya) and Gasherbrum (Karakoram) at 5400 and 7000 m; on Everest (Himalaya) at 5300 and 8000 m (the Willmann et al 45 study); and on a simulated climb to 8848 m using a hypobaric chamber. 46 -50 The general findings are that a tritan color vision deficiency could occur at an altitude as low as 1300 m in a minority of individuals, and the likelihood of the defect occurring in more individuals increases with altitude. In addition, minor deutan and protan color vision deficiencies could occur in a small number of individuals at altitudes 4000 m and above. The severity of the tritan defect decreases with acclimatization and, perhaps, supplemental oxygen. Nevertheless, there are some individuals whose color vision is likely to be unaffected up to altitudes of 7000 m. The mountain studies’ variable but general finding that tritan color vision defects occur in susceptible individuals is consistent with other studies that used hypobaric chambers or normobaric hypoxic conditions. If light levels are in the mesopic or photopic range, the overall effect of mild hypoxia equivalent to 3048 to 3778 m on color vision is similar to a reduction in retinal illumination. A tritan defect superimposed on generalized loss is more likely to occur in mesopic light levels and above 4000 m, especially at extreme altitude.6,47,51,52 However, this deficit is typically not noticed by mountaineers. The similarity of hypoxia-induced color vision defects to reduced retinal illumination is consistent with the reports of earlier mountaineers that hypoxia results in a dimming of vision. If this “dimming” is equivalent to viewing through a neutral gray filter, one would expect a loss along the tritan discrimination axis superimposed on a more generalized loss of discrimination.53,54 The impact of the “dimming” would be larger if the ambient light levels were already reduced.
Analysis of the Mera La Observation
This section reviews potential factors that could have altered the appearance of the cards at Mera La. Medications such as digoxin, and acetazolamide for AMS, can affect color vision. 55 However, no one took any medications, nor did anyone have diabetes or other conditions known to affect color vision. Age affects chromatic discrimination, with a mild, benign decline beginning after the age of 40 y, with loss of discrimination primarily along the tritan axis. 56 -58 The Mera La players’ ages ranged from 32 to 49 y, so age was not a likely factor. The confusion of red with gray would be consistent with a protan defect, which is more common in males of northern European descent. 59 While the Mera La players were in this demographic, the chance that all 4 card players had a protan defect is infinitesimally small given that the prevalence of protan defects in Caucasian males is approximately 2%. 59 After the expedition, author HVL’s color vision was tested and confirmed to be normal. Sunglasses may have been a factor. Specialty sunglasses with only 3 to 8% transmittances are often used in the mountains to bring luminance into the comfort zone. All 4 players at Mera La wore green-gray glacier-style sunglasses. No one thought to remove their eyewear to re-examine the cards. Nevertheless, long-term adaptation and other color-constancy mechanisms while wearing the tinted lenses could have reduced any color distortion. In addition, if the sunglasses were tinted enough to alter the cards’ color, then other color distortions would have likely been noticed in the days preceding the card game. It is unlikely that sunglasses were sufficiently dense to lower the light to mesopic or scotopic light levels. In bright sunlight with snow cover, the luminance levels at altitude can exceed 30,000 cdm−2, so the light level while wearing glacier glasses would still be well within the photopic visual range. 60 Nevertheless, the combined dimming effects of hypoxia and sunglasses could have lowered light levels into the low photopic region, so the sunglass contribution cannot be ruled out.
The next possibility is that the faded appearance of the red was due to hypoxia-related color vision defects. Figure 2 shows the simulated appearance of the card deck for each of the 3 types of color vision deficiencies. ImageJ (version 1.53t) with Vischeck dichromatic filters were used to create the images. The transformations are based on the Brettel et al 61 algorithm and represent the severe form of each color vision deficiency. They are a reasonable representation of each color defective person’s perception of colored images. 61 -63 Based on the simulations, the protan defect is the most similar to the altered perception experienced on the mountain at Mera La rather than the tritan defect, which would be the more common deficiency at altitude. The validity of this conclusion was confirmed by color measurements of the original card deck under a daylight source (data available by request).
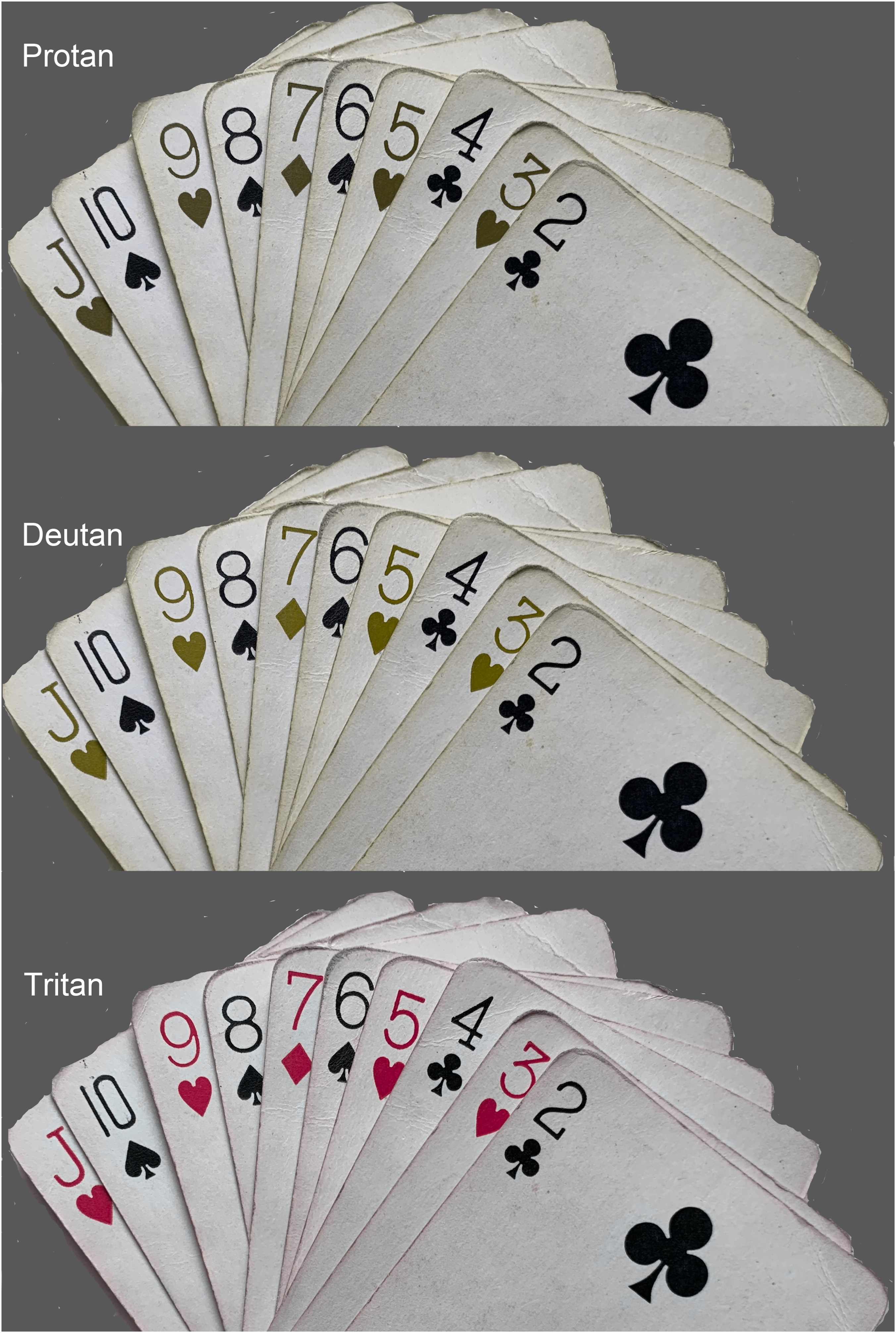
Simulated perception of the card deck for the 3 types of congenital color vision defects. The simulations were created using Image J (ver 1.53t) with Vischeck dichromatic filters.
Although the protan perception of the cards is consistent with the protan defect reported by others, there are other considerations. First, the hypoxia-related protan defect has only been reported in a small number of individuals. Second, the protan defect in the Willmann et al 45 study was subtle relative to the tritan defect. Third, the other observer in the Willmann et al 45 study showed a slight improvement in color discrimination along the protan color axis relative to a near–sea level altitude. These factors suggest that any change in the red suit’s appearance would be subtle and not noticed by everyone at the Mera La card game. The fact that all of the foursome saw the unequivocal change and no color alteration was noticed the day before suggests that other factors contributed to the change in appearance. Although the card game was played at the lower altitude of 4900 m the previous day, the light level was likely in the low photopic/mesopic range, which would have increased the probability of altered color perception compared with the afternoon game at 5300 m. We propose that the extreme glare during the afternoon game from the glossy white card background and the surrounding environment at the Mera La site was the other responsible factor and likely the major one.
This type of glare is referred to as disability glare. Disability glare reduces the luminance contrast of an object by scattering the light onto the object and by neural inhibitory effects. 60 The scattered light would also reduce the saturation of the red color, resulting in a more pink appearance; however, the bright background surrounding the figure would inhibit the brightness and hue, resulting in red having a gray or black appearance. 64 Red stimuli appear black when the luminance of the background is approximately 20 times brighter than the red stimulus. Glare from the glossy white background of the cards combined with the glare from the surrounding environment could have produced this brightness contrast with the red suit even while wearing sunglasses. Glare would not have had as large of an effect on the black suits because the inhibitory effect of the brighter surround canceled the reduced contrast from scattered light. In the laboratory, it was not possible to duplicate the glare effects from the surrounding bright environment on the mountain because of the uniformity in the artificial lighting, and the specular component of the background was appreciably reduced because the original deck had lost much of its glossiness since the expedition. Nevertheless, it is possible to experience the effect of glare by playing a card game on a tablet computer in bright sunlight.
Another critical issue revealed in this account is the problem of relatively inert brains at that altitude. Reports from comparable altitudes describe cognitive difficulties in sorting cards, scoring card games, playing chess, playing video games, reading books, and performing functions such as arithmetic or using a map or other navigational aids. 65 -68 This results from inattention; impaired short-term memory and mental coordination; slower reaction time; and psychomotor, visual, and neurological changes. These occur even with mild hypoxia and are only partially relieved by acclimatization.39,40 Indicative of these cognitive challenges, the Mera La group did not notice the visual change, whether from hypoxia or the other causes, until the first individual recognized it after approximately 1 h into the game. To quote Greene again, “The special senses at great altitudes are frequently blunted, although this change was not noticed by the majority of the expedition.” 35 That was certainly true in this case. We suggest that the inability to notice the change in color perception was because shape was a more dominant cue than color in playing cards. The fact that the altered color perception was not readily noticed and the members continued to play without apparent problems shows the value of using salient redundant coding, especially when critical information is conveyed at high altitudes and in other hypoxic settings.
Conclusions
This essay about color vision included an informal observation of an altered perception of the red color on playing cards in the Himalaya initially attributed to hypoxia alone. Analyses of the cards in the context of results of previous studies indicated that disability glare effects in the extremely bright lighting glacial environment, perhaps in combination with hypoxia, were more likely the cause of the perception of a grayer red. The climbers noticed the change in the appearance of the cards only after the game had been played for a while at the new altitude. Hypoxia likely impacted their ability to recognize either visual or mental changes. However, card game performance apparently remained the same because of the redundant shape clue.
Footnotes
Acknowledgment
The first author thanks Remi Sojka for teamwork at extreme altitude.