
Abstract
Objective
To determine the efficacy of 2 different sources of Ginkgo biloba extract (GBE) in reducing the incidence and severity of acute mountain sickness (AMS) following rapid ascent to high altitude.
Methods
Two randomized, double-blind, placebo-controlled cohort studies were conducted in which participants were treated with GBE (240 mg·d−1) or placebo prior to and including the day of ascent from 1600 m to 4300 m (ascent in 2 hours by car). Acute mountain sickness was diagnosed if the Environmental Symptom Questionnaire III acute mountain sickness–cerebral (AMS-C) score was ≥0.7 and the Lake Louise Symptom (LLS) score was ≥3 and the participant reported a headache. Symptom severity was also determined by these scores.
Results
Results were conflicting: Ginkgo biloba reduced the incidence and severity of AMS compared to placebo in the first but not the second study. In the first study, GBE reduced AMS incidence (7/21) vs placebo (13/19) (P = .027, number needed to treat = 3), and it also reduced severity (AMS-C = 0.77 ± 0.26 vs 1.59 ± 0.27, P = .029). In the second study, GBE did not reduce incidence or severity of AMS (GBE 4/15 vs placebo 10/22, P = .247; AMS-C = 0.48 ± 0.13 vs 0.58 ± 0.11, P = .272). The primary difference between the 2 studies was the source of GBE.
Conclusions
The source and composition of GBE products may determine the effectiveness of GBE for prophylaxis of AMS.
Introduction
Pike's Peak in Colorado has over 300 000 visitors per year who rapidly ascend from 2000 to 4300 m in 2 hours via cog train or car. As expected, many of these visitors experience acute mountain sickness (AMS). Visitors often do not see a physician to obtain acetazolamide, the standard prophylactic treatment for AMS for this type of rapid ascent.1,2 Furthermore, acetazolamide is not tolerated by some individuals and is associated with side effects such as paresthesia and nausea. 2 An alternative over-the-counter prophylactic treatment with no side effects would be optimal for prevention of AMS in people acutely ascending to high altitude.
Ginkgo biloba extract (GBE) is an easily obtainable over-the-counter alternative with few side effects that has been investigated as a preventative therapy for AMS.1,3–6 Results from these studies are variable; 3 studies report Ginkgo biloba reduced the incidence and severity of AMS3,4,6 and 2 studies report that it did not.1,5 In order to further investigate this, we tested the hypothesis that Ginkgo biloba would reduce the incidence and severity of AMS following rapid ascent to the summit of Pike's Peak.
We conducted 2 randomized, double-blind, placebo-controlled cohort studies over the course of 3 years to test the results of differing sources of Ginkgo biloba.
Methods
The methodology of the 2 studies was similar. For study 1 we recruited 44 participants and for study 2 we recruited 40 participants; both studies were conducted with the approval of the Mesa State College and the University of Missouri, Columbia Institutional Review Boards. Participants were primarily undergraduate and medical students from Mesa State College and the University of Colorado Health Sciences Center and resided between 1400 and 1600 m. Each participant completed a health questionnaire and signed an informed consent. Exclusion criteria included the following: pregnancy, smoking, a history of cardiac/pulmonary disease (except asthma), use of anticoagulants (including aspirin), history of a bleeding disorder, alcohol consumption within 24 hours prior to ascent, and a current viral illness. Participants were also excluded if they had been above 2100 m for more than 1 day in the preceding 2 weeks. Four participants were excluded from study 1 and 2 participants from study 2 for ascending to altitude within a week of the study, and 1 participant was excluded from study 2 for exercising during the study at altitude.
Drug and Randomization
The Ginkgo biloba dose for both studies (120 mg twice a day) was based on a previous study in which 80 mg of Ginkgo biloba administered twice daily was reported to reduce the incidence of AMS 4 as well as on the availability of 60-mg capsules in the United States and on the fact that Ginkgo biloba in doses of up to 300 mg per day is safe. 7
Drug treatment
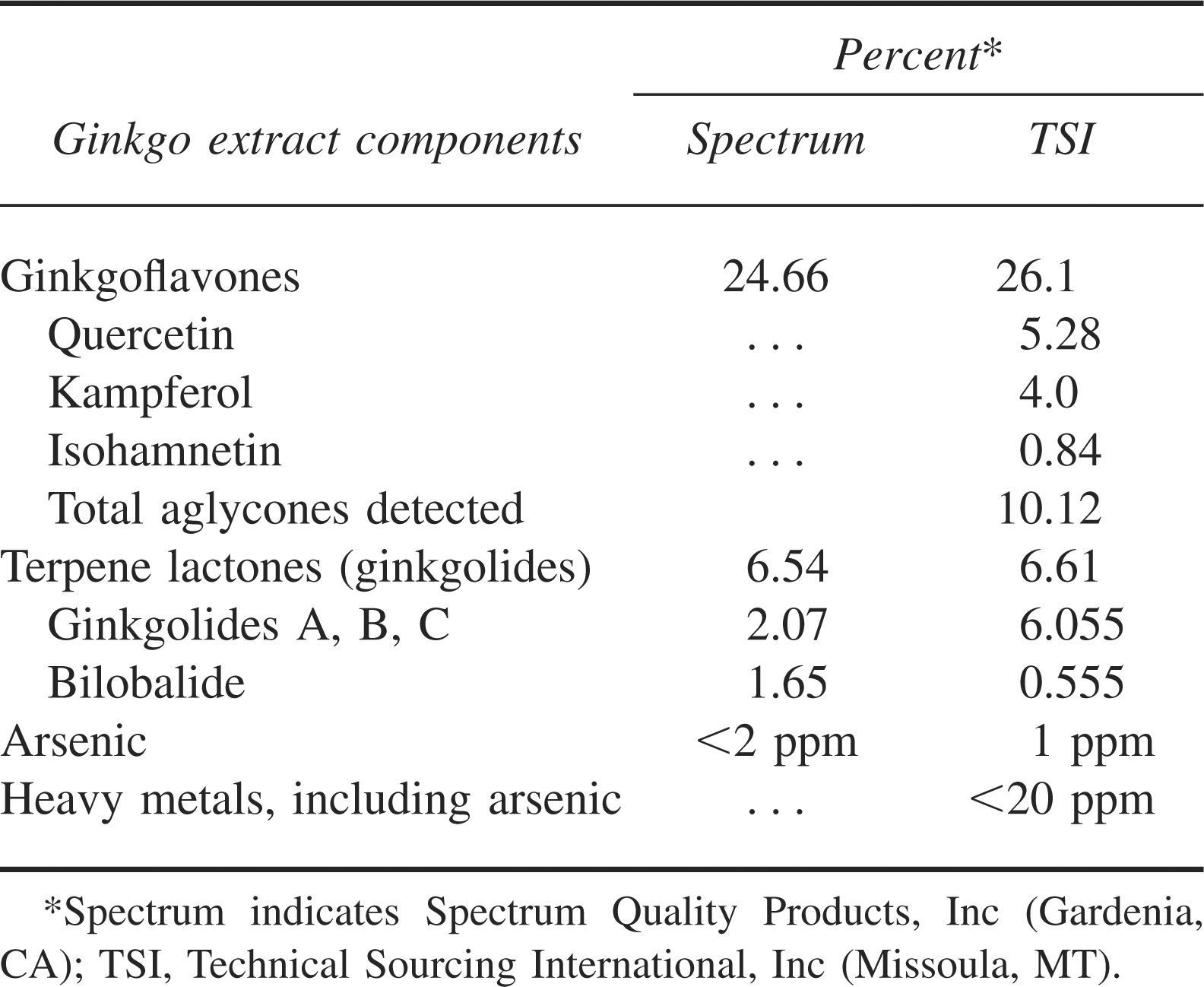
Ginkgo biloba (catalogue No. G1101, Lot No. OC0854) was obtained from standardized extract produced by Spectrum Chemical and Laboratory Products, Inc (Gardena, CA) for study 1 and Ginkgo biloba 24/6/5 was obtained from Technical Sourcing International, Inc (TSI, Missoula, MT) for study 2. A comparison of the composition of these 2 Gingko products based on high-performance liquid chromatography data supplied by the manufacturer is presented in Table 1. An oral dose of 120 mg of GBE or placebo was self-administered by participants twice per day, morning and evening, for 4 days (study 1) or 3 days (study 2) prior to ascent and during 24 hours at altitude, for a total treatment time of 5 days in study 1 and 4 days in study 2. The 5-day pretreatment was chosen initially based on the study by Roncin et al, 4 in which GBE was started at low altitude during a 5-day trek to reach high altitude. Pretreatment time was 1 day less in study 2 because this study was conducted simultaneously with a second study in which acetazolamide was compared with the placebo group and pretreatment with acetazolamide for longer than 4 days could not be justified. The participants in the acetazolamide arm of the second study were not included in the current study. The placebo capsules contained lactulose and did not differ in appearance. Participants were not allowed to take other drugs outside of the study preparations for treatment or prevention of AMS (eg, dexamethasone, acetazolamide, nonsteroidal anti-inflammatory drugs) prior to or during ascent.
Ginkgo biloba extract analyses
Randomization
Participants in each study were matched by age, gender, height, weight, and body mass index, and each pair was randomized to either GBE or placebo treatments, using a random number-assignment program.
Study Design
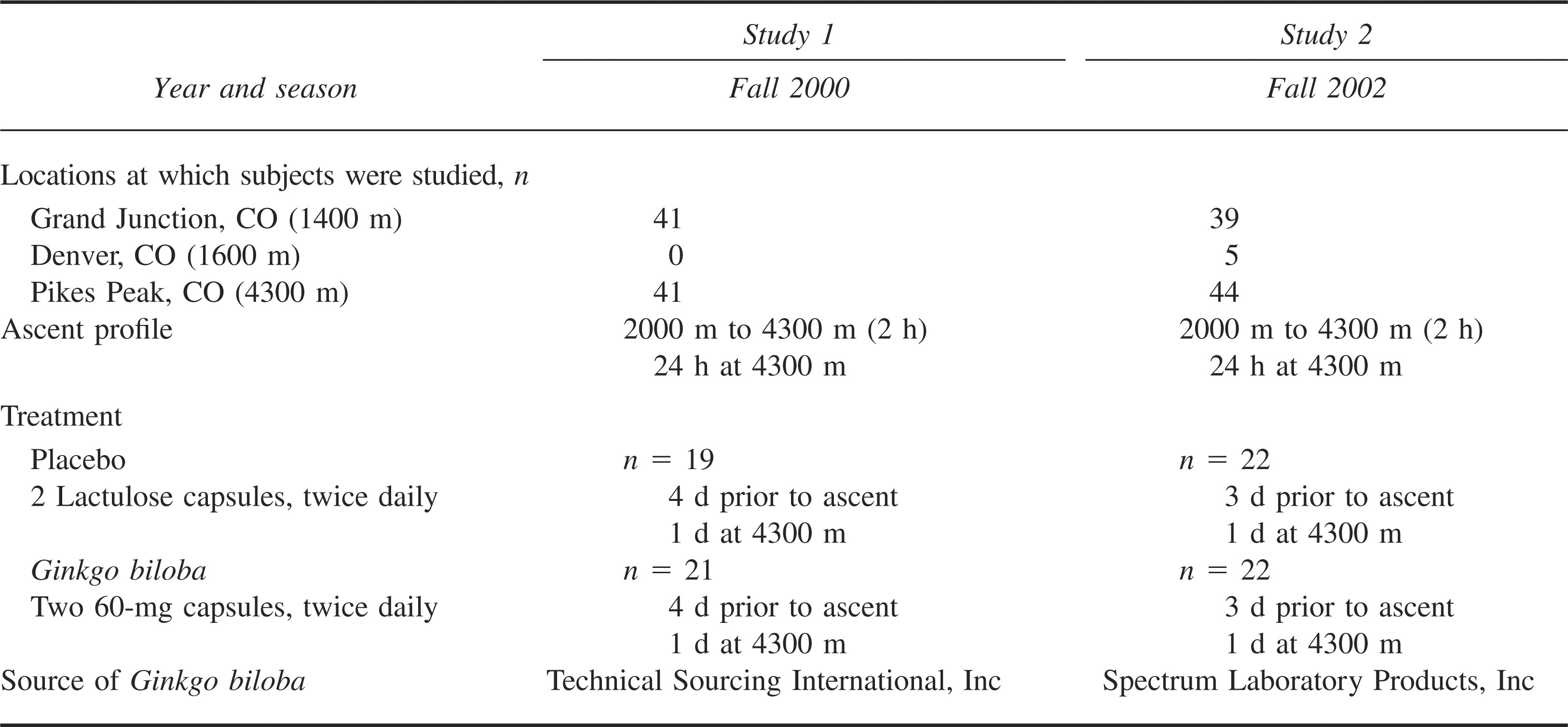
Both studies were randomized, double-blind, placebo-controlled, cohort studies. Environmental Symptom Questionnaire III acute mountain sickness–cerebral (AMS-C) section 8 and Lake Louise Symptom (LLS) questionnaires 9 were administered at 1600 m and again in a staging area at 2000 m just prior to ascent to 4300 m. Participants ascended from 2000 m to 4300 m in 2 hours by car (Table 2). Participants did not exercise at altitude. Final AMS questionnaires were administered after 24 hours at 4300 m or when participants terminated the study because of symptoms. If the participant was severely ill with AMS, AMS questionnaires were completed and the participant was treated with dexamethasone (4 mg by mouth or intramuscularly) and oxygen (1–2 L·min−1). 10
Comparison of study designs
Acute Mountain Sickness
The primary outcome measures were incidence and severity of AMS based on the AMS-C score, derived from the Environmental Symptoms Questionnaire-III and the LLS. Diagnosis of AMS was determined by an AMS-C score ≥0.7 and an LLS score ≥3 with headache. Higher AMS-C and LLS scores indicated greater symptom severity.
Statistics
Based on previous reports of GBE reducing AMS,3,4 a power test to determine samples size was conducted using an expected difference of 35% between the outcomes in the GBE and placebo groups (α = .05, SD = .5). This indicated that a total of 66 participants (n = 33 per treatment group) would provide 80% power for each study. Logistical and funding constraints prohibited including this many participants in each study; however, we decided to continue with the study as a means to examine trends and to generate preliminary data to support a fully powered future study.
The incidence of AMS between treatments was analyzed by Pearson's χ2 analyses. Analysis of variance was used to determine if participant characteristics differed between treatment groups within a study or between studies and to determine differences in LLS or AMS-C scores. Significance was set at P ≤ .05 for all statistical analyses.
Results
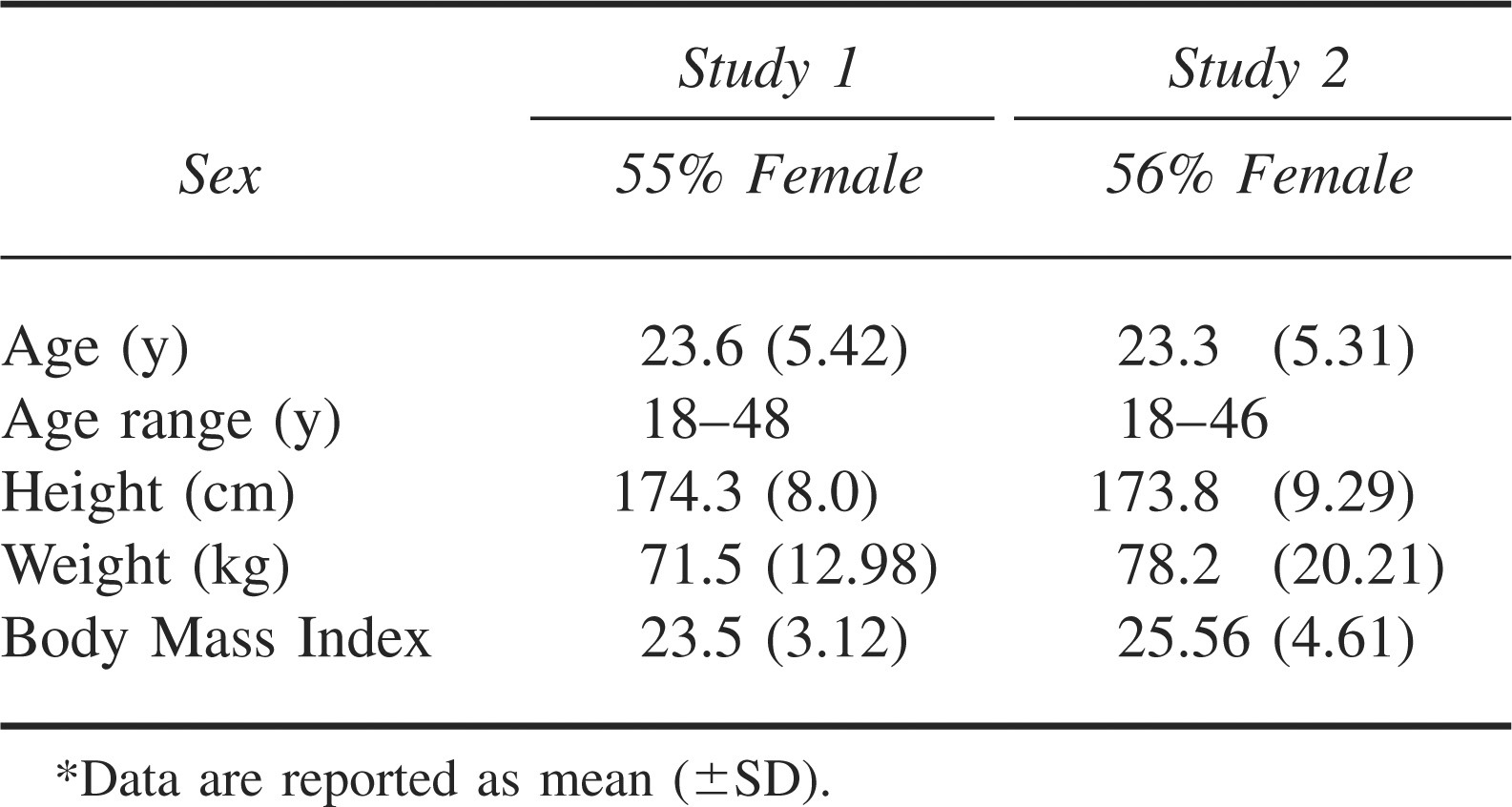
There were no differences between the 2 pools of participants nor between the placebo and active treatment groups with regard to gender, age, height, weight, and body mass index in either study (Table 3).
Subject characteristics*
Results of Study 1
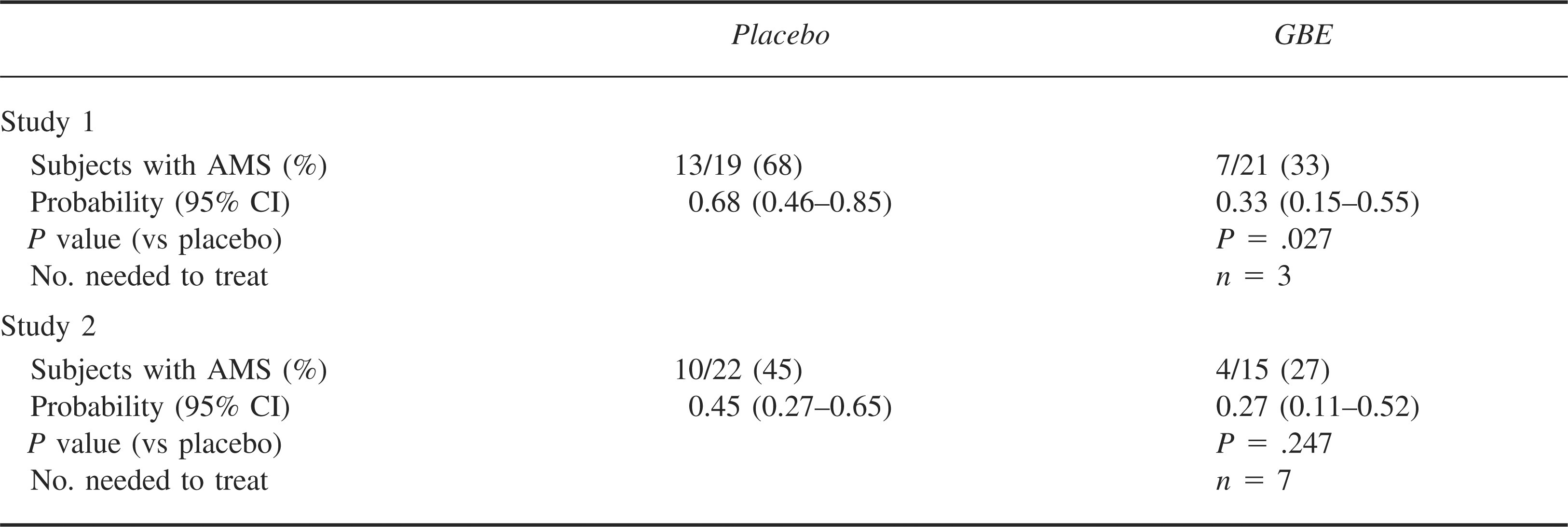
Treatment with 120-mg GBE twice daily significantly reduced both the incidence (Table 4) and severity (the Figure) of AMS in participants rapidly exposed to 4300 m. Sixty-eight percent of participants had AMS in the placebo group, compared to 33% in the GBE group. The number needed to treat was 3. Mean AMS-C and LLS scores were significantly greater for placebo than for GBE-treated participants (AMS-C: GBE, 0.76 ± 0.2, Placebo, 1.6 ± 0.32; LLS: GBE, 3.9 ± 0.62, Placebo, 6.2 ± 0.88; P = .03) (Figure). Three participants in the placebo group and no participants in the GBE group requested dexamethasone and oxygen treatment.
Incidence of acute mountain sickness (AMS) in subjects treated with Ginkgo biloba extract (GBE) vs placebo
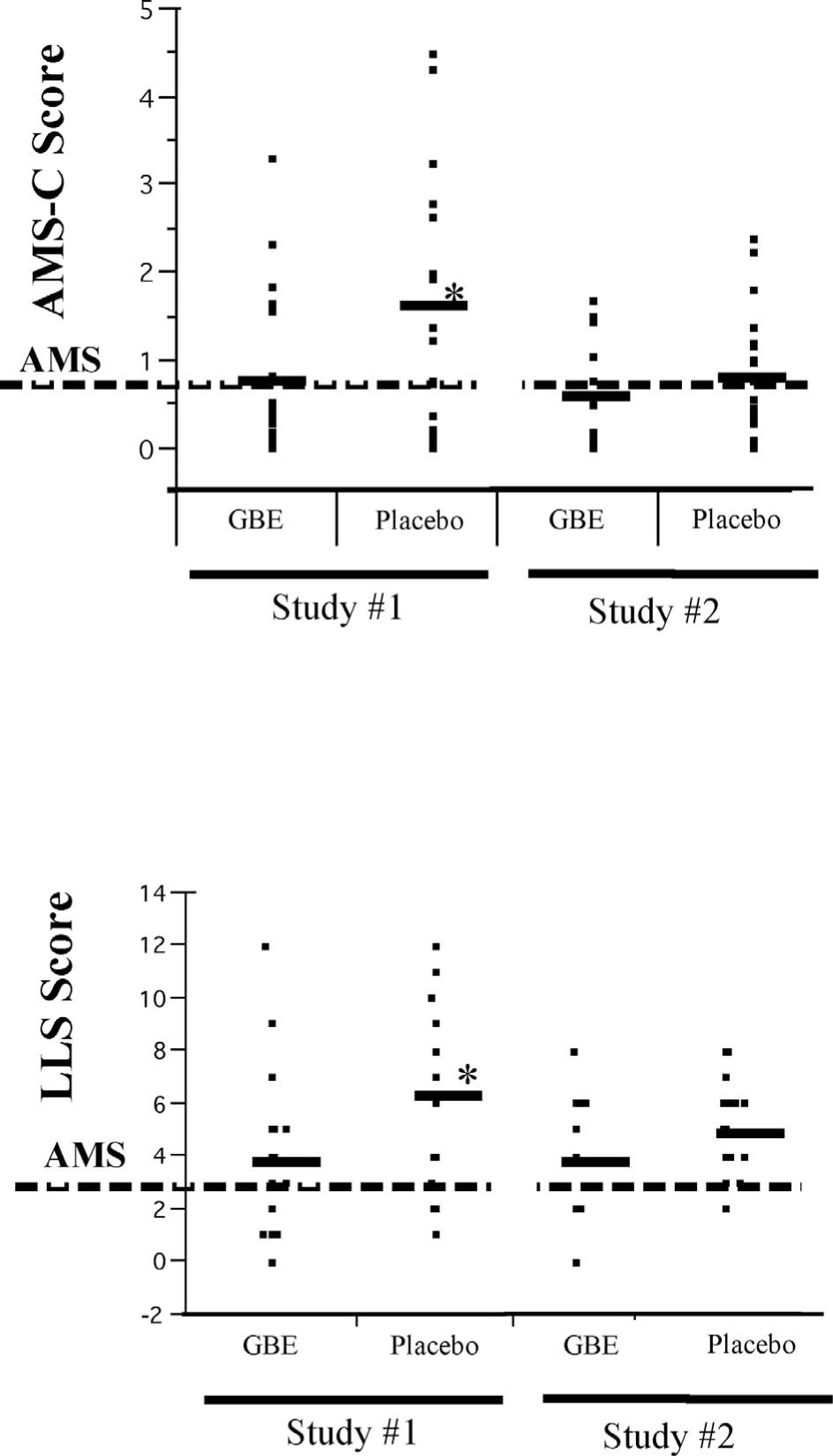
Severity of acute mountain sickness (AMS) symptoms 24 hours after rapid ascent to 4300 m in participants treated with placebo vs Ginkgo biloba extract (GBE). Mean acute mountain sickness–cerebral questionnaire (AMS-C, top) and Lake Louise Symptom questionnaire (LLS, bottom) scores were compared between treatment groups within each study. * indicates significantly different from placebo (P < .05). The dashed lines represent the threshold values for diagnosis of AMS.
Results of Study 2
Treatment with 120-mg GBE twice daily did not reduce either the incidence or severity (Table 4; the Figure, respectively) of AMS. Acute mountain sickness occurred in 45% of participants administered the placebo and in 27% of participants treated with GBE. The number needed to treat was 7. The mean AMS-C and LLS scores were not statistically different between the GBE- and placebo-treated participants (AMS-C: GBE, 0.59 ± 0.15, Placebo, 0.79 ± 0.14; LLS: GBE, 3.8 ± 0.59, Placebo, 4.9 ± 0.38). Four participants in the placebo group and three participants in the GBE group requested dexamethasone and oxygen treatment.
Discussion
Data from these 2 similarly conducted studies yielded differing results. In study 1 Ginkgo biloba reduced the incidence and severity of AMS and in study 2 it did not. These results reflect the literature, in which some studies demonstrated prevention of AMS with the use of GBE,3,4,6 while others showed no effect.1,5
Study Limitations
Our studies were underpowered as a result of the logistical and funding constraints of studying larger numbers of participants with this ascent profile. With these small sample sizes we cannot exclude a type II error. It also is not possible to accurately determine if data are non-normally distributed. Thus, standard parametric analysis was maintained. Nevertheless, a treatment effect was demonstrated in study 1. The Figure demonstrates that AMS scores were generally lower in the GBE group in both studies. Although this difference was not statistically significant in study 2, our results do not exclude the possibility that GBE is effective. Clearly, a larger trial is needed.
Although the difference in incidence of AMS in the placebo group between the 2 studies appears to be responsible for the discrepant results, the statistical power is too low to confirm such interpretations. The observed incidence of AMS in the placebo groups in both studies reflects what is reported in the literature for similar rates of ascent (50%–75%). 11 Therefore, we consider both these data sets reliable. The study by Gertsch et al 5 is the only adequately powered GBE and AMS study published; however, GBE was not administered until participants reached approximately 4300 m without evidence of AMS, thus skewing the population toward those who are less susceptible to the condition. In addition, taking GBE after being at altitude for 5 days and determining its effect with only a 600-m further ascent is not a proper design to determine prophylactic value.
Another limitation to interpretation of these 2 studies was that the pretreatment time differed by a day. Although it is possible that an extra day of pretreatment is required for GBE to have a prophylactic effect on AMS, we believe this is unlikely. Previous studies with positive results have had variable pretreatment times, and, furthermore, it is difficult to postulate a physiologic mechanism by which 1 day would make a difference. At this time there is no report in which various pretreatment lengths have been compared.
Source of GBE
The primary difference between study 1 and study 2 was the source of GBE. We believe this is the important factor in terms of why our 2 studies had differing results. Ginkgo biloba extract product also differed in previous studies by other authors.1,3–6 Although the 2 studies by Gertsch et al 5 used the same commercial product, the GBE was processed from different harvests, which can produce differing concentrations of active components. 12 The known variability in herbal preparations makes studying these compounds and comparing results between studies extremely difficult. Recent studies using advanced methodologies have revealed that although GBE supplements may meet the German Commission E and World Health Organization recommendations, newly identified active components in GBE vary considerably between preparations.13,14 In the current study, the preparation by Spectrum Quality Products, Inc, had less concentration of ginkgolides A, B, and C and more bilobalide than did the preparation from TSI. Further, the first preparation contained ginkgolides other than ginkgolides A, B, and C or bilobalide, possibly ginkgolides J and M. Further, some commercial preparations contain added vitamins and other substances that may act as confounding factors for development of AMS. Because the pathophysiologic mechanism of AMS is unknown, and since the specific percentages of active components and their biological activities may vary greatly, the ability of commercially available Ginkgo biloba to reduce the incidence and/or the severity of AMS is unpredictable.
Prevention of AMS
Because visitors to easily accessible mountain summits are often poorly prepared for altitude ascent, a safe over-the-counter AMS preventative would be useful. Results from previous research on prevention of AMS with Ginkgo biloba have been highly variable. In the current studies 2 sources of over-the-counter preparations of Ginkgo biloba did and did not reduce the incidence and severity of AMS following rapid ascent to Pike's Peak summit (4300 m). To assess whether the different results were due to the different GBE products or to the studies being underpowered will require further work with larger numbers of participants and strict control of the GBE ingredients. At this time the evidence supporting or refuting the use of Ginkgo biloba for prophylaxis of AMS is not definitive.
Footnotes
Acknowledgments
The authors would like to extend our gratitude to Robert Roach, MD, for assistance with determining the AMS scoring systems. The authors would like to thank Jamie Bendrick-Peart, Virginia Beckey, and Julie Meuret for technical assistance with these studies. Special thanks go to the City of Colorado Springs for allowing us to use the venue and mountaintop facilities and to the Pike's Peak Rangers for outstanding assistance on the mountain. Sources of support for this work include Technical Sourcing International, the Wilderness Medicine Society, and the American Academy of Family Physicians Foundation.