
Abstract
Introduction
Illegal gold mining is flourishing in French Guiana, existing outside the law due to both the high cost of gold mining permits and the challenges of law enforcement within the Amazon forest. We report the characteristics of, and the medical responses to, medical emergencies in illegal gold mining sites.
Methods
We performed a retrospective study of all medical emergencies reported from illegal gold mining sites to the centralized call office of SAMU 973 from 1998 through 2000 and from 2008 through 2010. According to the national health care system, any medical emergency within the territory is handled by the prehospital emergency medical service (SAMU 973), irrespective of the patients’ legal status. Data were extracted from the SAMU 973 notebook registry (1998–2000) or the SAMU 973 computerized database (2008–2010) and werre collected using a standardized questionnaire.
Results
Of 71,932 calls for medical emergencies in French Guiana during the study periods, 340 (0.5%) originated from illegal gold mining sites. Of these, 196 (58%) led to medical evacuation by helicopter, whereas the overall rate of evacuation by helicopter after placing a call to SAMU 973 was only 4% (3020/71,932; P<0.0001 for comparison with illegal gold mining sites). Medical emergencies were classified as illness (48%, mostly infectious), trauma (44%, mostly weapon wounds), and miscellaneous (8%).
Conclusions
Medical emergencies at illegal gold mining sites in the Amazon forest mostly include infectious diseases, followed by trauma, and often require medical evacuation by helicopter. Our study suggests that implementation of preventive medicine within gold mining sites, irrespective of their legal status, could be cost-effective and reduce morbidity.
Introduction
French Guiana is an overseas department of France located in the Amazon forest, on the north Atlantic coast of South America. Gold extraction is a major economic activity, accounting for 32% of French Guiana exports in 2012. The expanding and poorly controlled gold market has led to gold rushes, with populations coming from the poorest regions of neighboring countries like Brazil and Suriname. 1 The citizens of French Guiana have the same legal status as those of any French territory and have access to free health care and education, regardless of legal status. Almost 40% of the population is foreign-born, and 20% (40,000) are illegal immigrants. 2 Although population density is still low and heterogeneous, the territory—approximately the size of England—currently experiences the highest annual population growth in South America. Between 1999 and 2009, the mean population increase in French Guiana was estimated at 3.6% per year by the National Institute for Statistics. 3 Future demographic trends will be a further challenge for governmental authorities because the population is projected to double within 15 years due to both high birth rates and extensive immigration.
In this hot and humid environment, infectious diseases and accidents are frequent. As compared to metropolitan France, mortality attributable to infectious diseases and accidents is 3 times and 1.6 times higher, respectively. 4 More than 90% of the territory is covered by dense forest, and such geographic isolation magnifies the vulnerability of patients. In cases of medical emergencies, access to care depends on a reliable alert signal and the availability of medical teams that can rapidly deploy to the emergency sites, often by helicopter due to the limited road access. Out-of-hospital medical emergencies are handled by the Service d’Aide Médicale Urgente (SAMU 973), a public service charged with prehospital emergency medical care. This hospital-based department operates through a centralized call office, supervised by a medical doctor who is responsible for the response to each call. Mobilization may include helicopter dispatch: a Dauphin SA365 (operated by a private company under contract with the hospital), a Dragon EC 145 (civilian security for night mission or winching), or a Puma SA 330 (a military aircraft that may be activated as a last resort). One emergency physician and one emergency nurse from the Cayenne hospital are the minimum medical response team for emergency helicopter deployments. SAMU 973 plays an essential role for medical assistance in illegal gold mining sites because miners have limited to no access to basic health care. For these sites, the decision to deploy a medical response is affected by the information obtained through the call and the existing evacuation means available on site, as well as medical and helicopter resource availability, which may be limited by competing demands, weather constraints, time of day, security concerns, and accessibility to the gold mining site.
Gold miners’ living conditions and access to health care are understandably difficult and limited.5,6 The work sites are isolated, only accessible by helicopter or by several days of boat travel and/or walking. In French Guiana, illegal status does not preclude access to the health care system, 2 ,6,7 but a legal statute dictates that no patient can be attended to by health care providers within the domain of an illegal gold mining site. Due to security concerns for medical teams, since December 4, 2003, it has been unlawful for providers to respond to an illegal gold mining site; therefore, patients in need must be carried to a secure place outside of the gold mining site to be managed by medical teams.
To date, health issues in gold mining sites have been poorly characterized, 8 with the exception of mercury poisoning. 9 –11 We report the characteristics of, and the medical responses to, medical emergencies in illegal gold mining sites.
Methods
Study Design
We performed a retrospective study of all medical emergencies reported from illegal gold mining sites to the centralized call office of SAMU 973 from 1998 through 2000 and from 2008 through 2010. These study periods were selected to analyze the effect and potential consequences on medical emergency services of the 2003 regulation that prohibited the provision of medical care on illegal gold mining sites, with study periods beginning 5 years (1998–2000) before and 5 years (2008–2010) after the law went into effect.
Data Collection
Data were extracted from the SAMU registry for 1998 through 2000 (a notebook with standardized collection of data for each call), and from the computerized database for the years 2008 through 2010 (SAMUSCRIPT software; Scriptal, Paris, France). Of note, more clinical details were available with the notebook registry compared with the software collection. We only enrolled calls that originated from gold mining sites (ie, calls for illegal gold miners who were primarily attended to at a health care center were excluded). Data were collected using a standardized questionnaire, including the following variables: date and origin of call, sex, age group (ie, 0–15, 16–30, 31–45, 46–60, and >60 years), motive of call, suspected severity, delay between the call and medical evacuation, and final decision (ie, transport by helicopter to referral hospital, consultation at the closest health care center by conventional means, or medical advice by phone). The database was authorized for data collection by the French regulatory commission (Commission Nationale Informatique et Libertés, CNIL), and the study was approved by the Cayenne Hospital Institutional Review Board (#2080002).
Data Analysis
Data were analyzed with Excel and STATA 8. The 2 study periods were compared using χ2 tests for qualitative variables and t tests or Mann Whitney U tests for quantitative variables, as appropriate. A P value of <0.05 was considered statistically significant.
Results
Of 71,932 calls for medical emergencies in French Guiana during the study periods, 340 (0.5%) originated from illegal gold mining sites: 113 from 1998 through 2000 and 227 from 2008 through 2010. Of these, 196 (58%) required medical evacuation by helicopter, as compared with 4% (3020/71,932) overall in French Guiana (P<0.0001). The proportion of calls requiring evacuation by helicopter was similar during the 2 study periods: 64/113 (57%) from 1998 through 2000 and 131/227 (58%) from 2008 through 2010. The yearly incidence of calls from gold mining sites increased over time (P<0.01), in parallel with increases in the price of gold (Figure 1). We observed a trend toward a higher incidence of calls for trauma and medical emergencies during the rainy season (November−February, Figure 2; P=0.11).
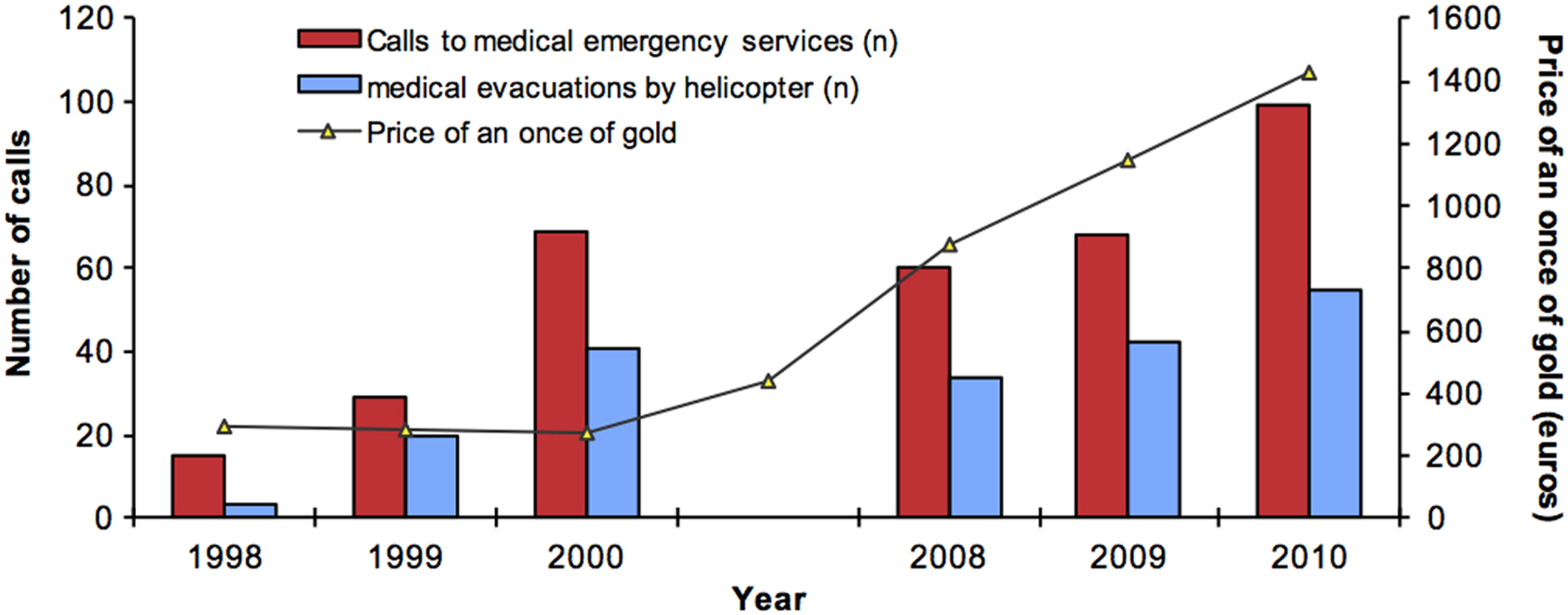
Calls from illegal gold mining sites to prehospital emergency services, medical evacuation by helicopter, and price of gold during the study periods.
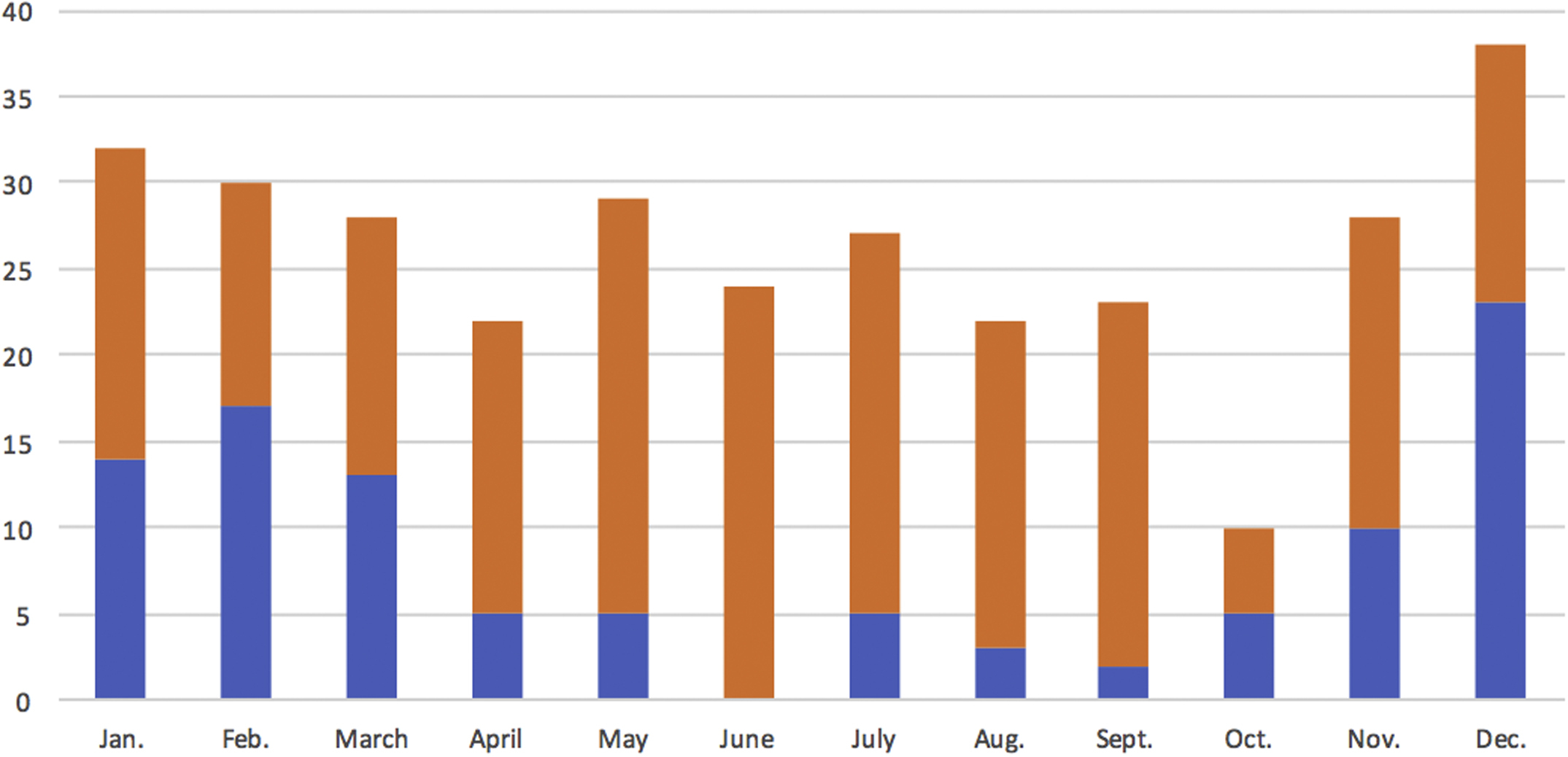
Mean number of monthly calls during the 2 study periods. (Note: rainy season is from December to February.)
Persons for whom the calls were initiated were mostly men (86%) and 31 to 45 years of age (57%). The proportion of women was higher in the latter period: 41/210 (20%) from 2008 through 2010 vs 2/113 (2%) from 1998 through 2000 (P<0.001). Medical emergencies were classified as illness (48%), trauma (44%), and miscellaneous (8%) (Table 1), with no significant difference between the study periods. However, during the 1998 through 2000 period, neither gynecological nor obstetrical problems were reported, whereas 9 obstetrical emergencies were reported from 2009 through 2010.
Classification of health issues that led to call the medical emergency service
Heat stroke, urogenital, skin diseases.
Including polytrauma (n=25), lower extremity trauma (n=20), abdominal trauma (n=13), upper extremity trauma (n=10), head trauma (n=5), chest trauma (n=5), and spinal trauma (n=5).
Snake (n=6), not specified (n=3), scorpion (n=1), spider (n=1).
Full-term delivery (n=3), premature labor (n=3), vaginal bleeding during pregnancy (n=3).
Discussion
We found that the incidence of medical emergencies has increased in French Guiana illegal gold mining sites, mostly related to illness (48%) and trauma (44%). Of note, more than half of the calls for medical emergencies in this setting required medical evacuation by helicopter due to the absence of any road access in most of these sites, at a cost of $97 per minute ($11,640 for a 2-h flight). We presume the increase in emergency calls was driven by the dramatic increase in gold prices over the last decade, which may have boosted the flow of illegal immigrants to work in illegal gold mining sites (Figure 3).1,6 The 2003 regulation that prohibited direct, on-site medical response to illegal gold mining sites has had no measurable impact on the characteristics and number of calls from these sites.
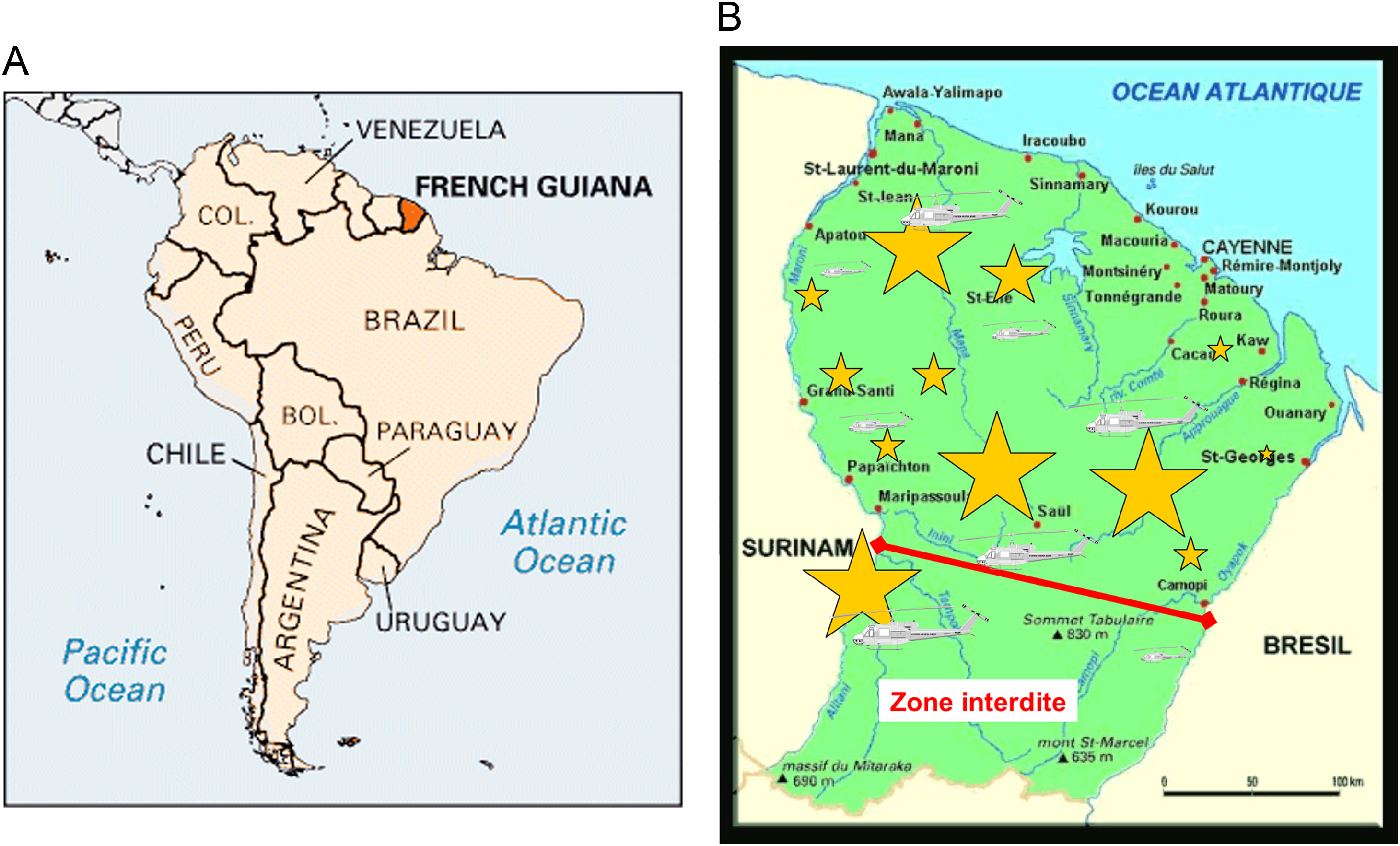
French Guiana (A), major gold mining sites (B). Yellow stars: gold mining sites (proportional size). Source: Wikimedia Commons.
To the best of our knowledge, no systematic study of medical emergencies in gold mining sites has been reported to date. Our study provides original data that may be of value for 1) preparation and training of emergency medical services in areas with illegal gold mining sites; and 2) implementation of preventive services that focus on the diseases most commonly responsible for emergency calls.
We found that febrile illnesses were the most common reasons for calling emergency services, which suggests that infectious diseases rank first among medical emergencies in gold mining sites. Although not surprising in an area endemic for malaria, dengue, Zika, chikungunya, food-borne illnesses, and many other tropical diseases, this finding should stimulate implementation of preventive medicine in these gold mining sites. Such interventions could include permethrin-impregnated mosquito nets and increased efforts to maintain best-practice hygiene in food preparation. Although these measures may not be straightforward to implement in illegal settings, the high cost of medical evacuation in these remote areas implies that successful preventive medicine intervention is likely to be cost-effective. Of note, illnesses are also the most frequent reason for calling prehospital emergency medical services in similar settings, 12 and fever is the most common symptom reported upon admission at the emergency department of the French Guiana referral hospital in Cayenne (unpublished data) as well as at Saint-Laurent du Maroni, the referral hospital at the Suriname border. 7 Malaria is a major public health problem in French Guiana, with an incidence estimated at 3000 to 4500 cases each year, one third being caused by Plasmodium falciparum.13,14 Even in malaria-free areas, migration of gold miners from endemic areas may lead to the re-emergence of malaria due to the presence of competent Anopheles vector, as has been documented in Brazil. 5 ,15,16 Other less common infectious diseases have been reported, such as human rabies (1 case in Cayenne in 2008) and yellow fever (last reported human case in French Guiana, 1997). 17 Outbreaks of Junin, Machupo, and Sabia viruses have been reported in South America in remote, isolated sites, including mining camps. 18 –20 Surveillance of emerging diseases through the analysis of calls for medical emergencies has been proposed by others 21 and may be of particular interest in marginalized populations, such as gold miners, for 2 reasons: 1) because they live very close to the forest, they may be at risk of rare and severe zoonotic diseases (eg, Ebola in Africa, yellow fever in Africa and South America); and 2) because they currently have limited access to medical care, outbreaks in this population may remain undetected for long periods of time.
Some characteristic features of gold mining sites deserve further description because they clarify the high incidence of traumatic emergencies. First, the criminal use of weapons is common in illegal gold mining sites, notably during gold transfer, which highlights the insecurity of the environment.1,6 Forensic investigations of gold mining sites have found ample evidence of nonreported executions (unpublished data). Second, 4-wheel off-road vehicles and motorcycles are extensively used for transport on unstable terrain around mining sites, which may explain a significant proportion of motor vehicle accidents. Third, unlike in legal mining sites, trees are left standing in close proximity to illegal gold mining sites to avoid discovery by law enforcement. As mining operations remove soil through high-pressure hoses, trees may become unstable and fall on workers. 22 The proportion of accidents due to local fauna or envenomation remains limited, commensurate with findings from French Guiana as a whole, where only 10 deaths by envenomation (6 by snakes) have been reported within the last 25 years; aggression by wild fauna was responsible for just 1.3% of calls to the prehospital emergency medicine service. 23 Regarding the demographic characteristics of illegal gold miners in French Guiana, most are Brazilian (>90%), with a male predominance (ratio of 2.4:1) and with significant experience in gold mining (median, 10 years). Overall, 48% of illegal miners either never attended school or did not attend beyond the primary grades. Access to medical care is particularly difficult for illegal miners—one study cited that of 156 miners with hypertension, only 2 had medical follow-up. 24
This study has limitations. First, because it was performed in French Guiana, its findings may not be pertinent to gold mining sites in other parts of the world with different working conditions, endemic diseases, and health care systems. Second, this was a retrospective study and therefore is subject to collection bias. Symptoms reported through patient phone calls do not necessarily reflect diagnoses, especially when the caller has limited medical skills or is not fluent in the local French language.
This study does, however, provide an overview of medical emergencies in illegal gold mining sites reported to the prehospital emergency medicine service for the whole territory and may be used as a pilot study to guide the implementation and evaluation of preventive medicine in the field.
Conclusion
Medical emergencies in illegal gold mining sites in the Amazon forest mostly include infectious diseases and trauma and often require medical evacuation by helicopter. Implementation of preventive medicine within gold mining sites, irrespective of their legal status, could be cost-effective and reduce morbidity. This may include provision of permethrin-impregnated mosquito nets, kits for basic hygiene, prevention of sexually transmitted diseases, and access to primary health care centers where nonsevere trauma could be managed before complications occur.
Author Contributions: Study concept and design (GE, RP, MN); acquisition of the data (GE); analysis of the data (GE, PT, RP, MN); drafting of the manuscript (GE, PT); critical revision of the manuscript (GE, PT, RP, MN); approval of final manuscript (GE, PT, RP, MN).
Financial/Material Support: None.
Disclosures: None.