
Abstract
The crown-of-thorns starfish (Acanthaster planci) inhabits coral reefs, largely throughout the Indo-Pacific region. Its dorsal surface is covered with stout thorn-like spines. When handled or stepped on by humans, the spines can puncture the skin, causing an immediate painful reaction, followed by inflammation and possible infection. Initial pain and swelling may last for days. Effects of envenomation on the liver have been demonstrated previously in animal models, but hepatic toxicity has not previously been described in humans. We describe elevated liver enzymes in a 19-year-old female associated with A planci spine puncture wounds. To our knowledge, this is the first documented report of transaminitis in a human after A planci envenomation.
Case Report
A 19-year-old female presented to the Stanford University emergency department with a chief complaint of right foot pain, redness, and swelling. She reported that 48 hours prior she had inadvertently stepped on a “crown-of thorns” starfish while walking in shallow waters adjacent to a beach in the Republic of Fiji. Several spines of the starfish punctured the plantar aspect of her foot and toes. She was instructed by locals on the beach to place the underside of the starfish over her wound to allow the animal to “suck out the venom,” which she did. The patient reported that she could feel the live animal sucking on her foot, and that the pain was extremely severe. Immersion of her foot in vinegar did not help the situation. She continued to have intense pain in her foot, and, during a period of extreme pain, had a single, brief syncopal episode. Later that day, she sought medical attention at a local hospital. She was given a prescription for oral amoxicillin and an unspecified topical antibiotic ointment. She was also given a combination of propoxyphene and acetaminophen for pain control. A physician parent administered intramuscular ketorolac, which provided only partial pain relief.
The patient reported that 24 hours after being envenomed, she experienced severe abdominal pain associated with nausea and a few episodes of nonbloody, nonbilious vomiting. She denied jaundice.
Forty-eight hours after the incident, the patient continued to experience persistent, severe pain in her right foot. She presented to our Emergency Department on her return to the United States, concerned because her foot had become red and swollen. Her nausea and abdominal pain were resolved at the time of presentation. She denied fevers or chills. She had only taken a single dose of the antibiotic and pain medication at the time of presentation. Review of systems was otherwise negative.
The patient had no significant contributory past medical history. She took no medications chronically. She stated childhood allergies to trimethoprim-sulfamethoxazole and amoxicillin-clavulanate, but was unsure about the precise nature of the reactions. The patient was a high school student, and both of her parents were physicians. She denied tobacco, alcohol, and illicit drug use.
On physical examination, the patient appeared well and was in no acute distress. Blood pressure was 115/70 mmHg, heart rate was 77 beats/min, respiratory rate was 18/min, and oral temperature was 98.1°F (37°C). Skin color was normal, without jaundice or scleral icterus. Her cardiac, pulmonary, and abdominal exams were unremarkable. There were nontender, bilateral palpable inguinal lymph nodes that were thought to be enlarged.
Examination of the right foot showed erythema and edema extending in a sock-like distribution to the midfoot level. Several puncture marks were visualized on the plantar aspect of the foot, especially prominent under the first and second toe (Figure 1). No spines or fragments were visualized. The foot was tender to gentle touch.

Photograph of patient's right foot, taken on presentation to the Emergency Department. Multiple puncture wounds are noted in several toes.
After initial examination, the patient was administered tetanus-diphtheria toxoid, 0.5 mg IM, after which pain control with intravenous morphine sulfate was initiated. Radiographs of the right foot were obtained (Figure 2). These revealed thin, faintly radiopaque densities projecting within the soft tissues of the first, second, third, and fourth digits distally. The foot was then imaged with a computed tomography scan, which revealed associated skin thickening and subcutaneous stranding around the spines, consistent with inflammatory changes (Figure 3). More specifically, multiple thin linear radiopaque opacities were noted in the plantar aspects of the first through fourth toes.

Lateral plain radiograph of patient's right foot. The black arrow denotes a radiopaque spine in the soft tissue of the patient's great toe.
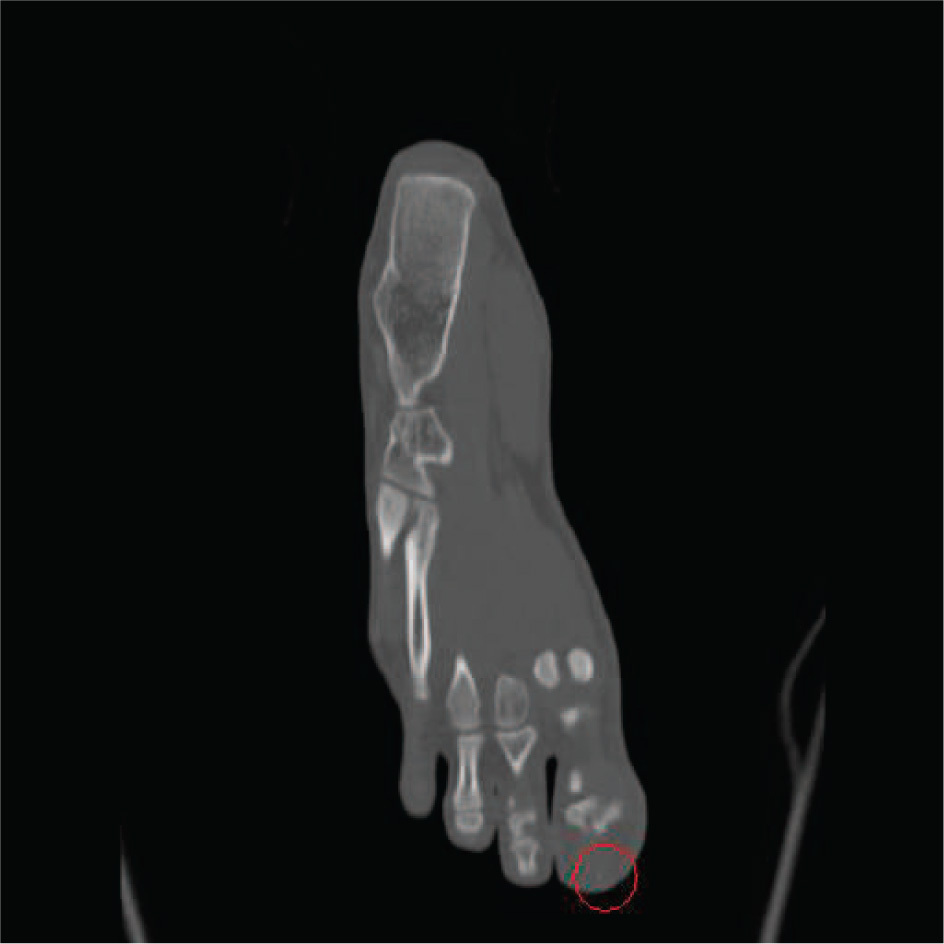
Selected computed tomography image of patient's right foot. A red circle redemonstrates a spine that was seen on the plain radiograph.
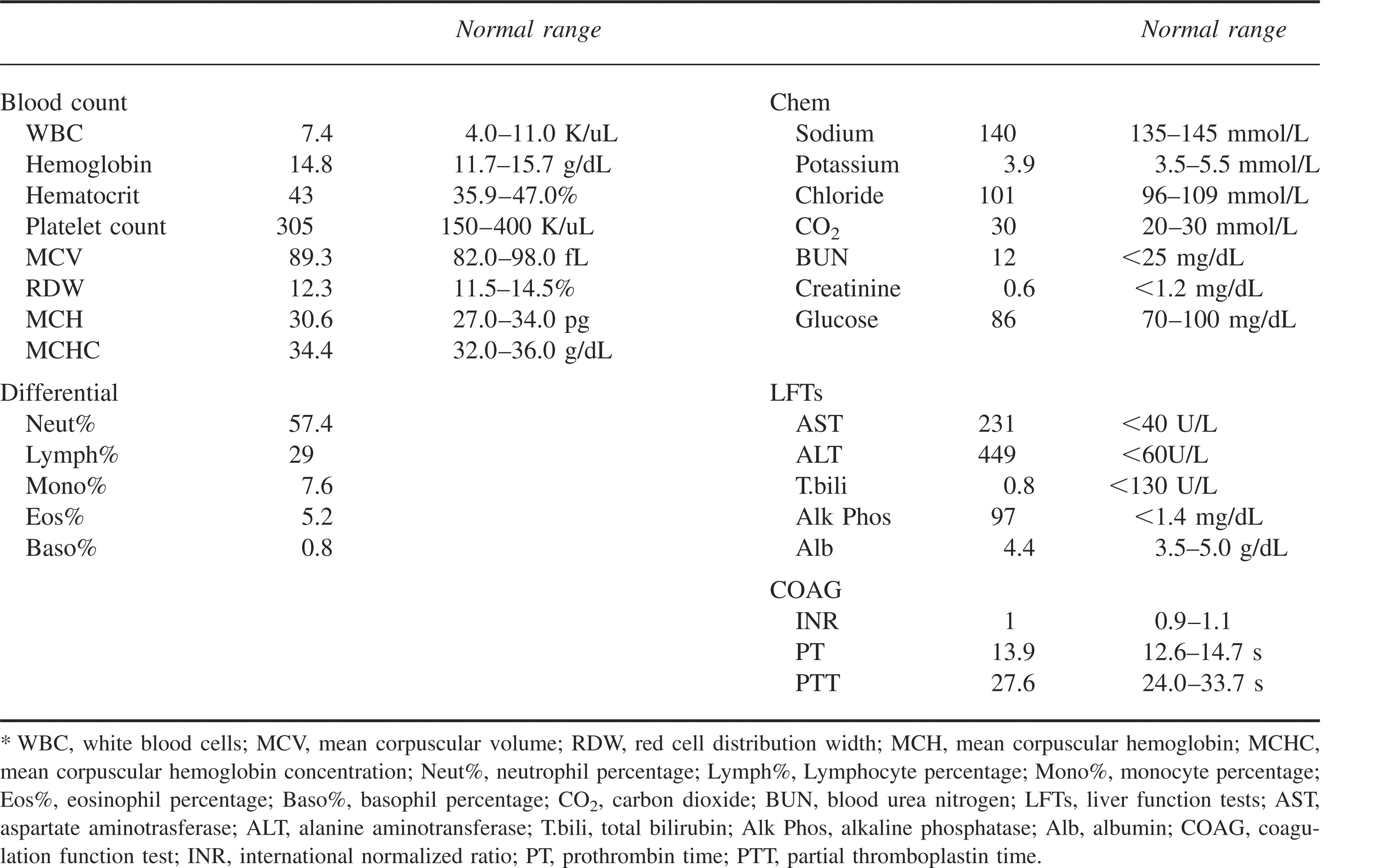
Laboratory testing was obtained (Table 1). Most significantly, there was elevation of liver transaminases, including aspartate aminotransferase of 231 U/L (normal <40 U/L) and alanine aminotransferase of 449 U/L (normal <60). Total bilirubin and alkaline phosphatase were normal.
Initial laboratory values*
An attempt to remove the spines was made in the Emergency Department under local anesthesia by an orthopedic surgeon, but the procedure was poorly tolerated by the patient secondary to pain. She was admitted to the hospital for intravenous antibiotics and pain control. The patient was treated with ciprofloxacin and morphine. She was discharged the following morning.
In a follow-up visit with her personal physician 3 days later, she was noted to have persistent elevations in liver function tests, including aspartate aminotransferase, 95 U/L, and alanine aminotransferase, 268 U/L. The toes of her right foot were noted at the initial follow-up visit to be erythematous with some maceration. In preparation for further surgical intervention, a right foot magnetic resonance image scan was obtained. No obvious foreign body or fluid collections were seen, but interosseous edema was identified.
The patient was referred to a foot surgeon, who evaluated the patient 8 days after her initial presentation. At that time, exam revealed multiple punctuate lesions at the ends of her toes, as well as areas of necrotic and sloughing skin on the first, third, and fourth toes. After assessment of her radiographs, further debridement was advised. The patient was taken to the operating room the following day. Under general anesthesia, the first through fifth toes were meticulously debrided. Per the operative report, tracts were opened wherever there was evidence of purulence or a spine was identified. The largest fragment removed was a 7-mm foreign body in the second toe. Under loupe magnification, at least 6 tracts were unroofed.
On postoperative wound check 6 days later, the patient's foot was judged by the surgeon to be improving, with decreased erythema and no drainage. One area of the third toe was noted to have a small area of white eschar. A follow-up plain radiograph was obtained, which revealed some thin remaining spines deemed too small for removal. The patient was administered a 14-day course of ciprofloxacin and clindamycin.
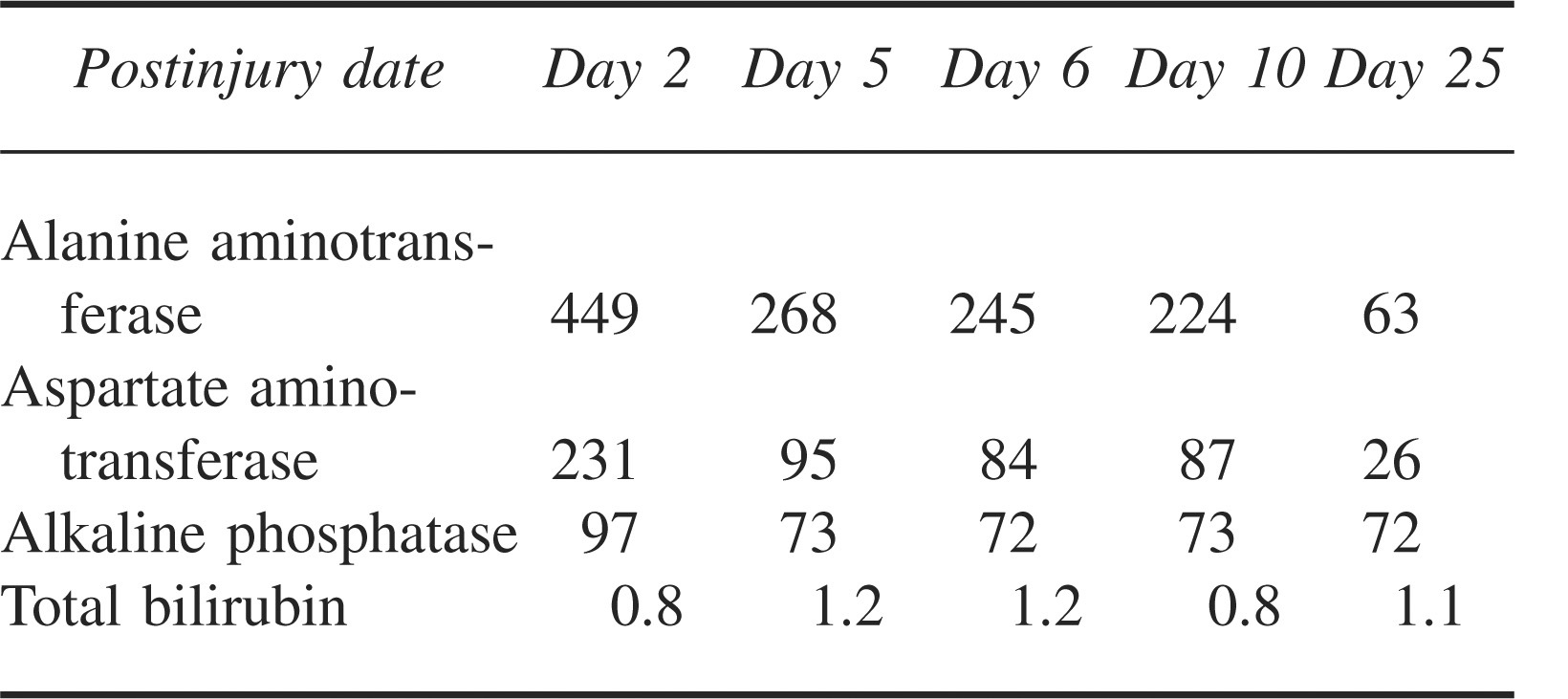
The patient was followed by her personal physician, who observed her liver function tests to normalize 25 days after her initial presentation and 16 days after the surgical debridement. The trend in liver function test normalization is shown in Table 2. She reported no further abdominal pain, nausea, or vomiting. The patient's clinical course was notable for an infection of the third toe, diagnosed 32 days after her original presentation. A culture of drainage from this wound revealed an infection with methicillin-resistant Staphylococcus aureus (MRSA). This infection was hypothesized to be due to household exposure. The infection was treated with a 2-week course of linezolid.
Liver function test values
At 2-months postexposure, the patient reported full weight-bearing status and ability to tolerate wearing shoes. She continued to feel a foreign body sensation in her great toe, “as if some spines are still trying to work their way out.”
Discussion
The crown-of-thorns starfish (or “sea star”) Acanthaster planci has long, sharp, and venomous thorn-like spines (up to 2.4 inches or 6 cm in length) sprouting from its body for protection. The animal can grow up to 32 inches (81 cm) in diameter, and have up to 21 arms extending from its center (Figure 4).
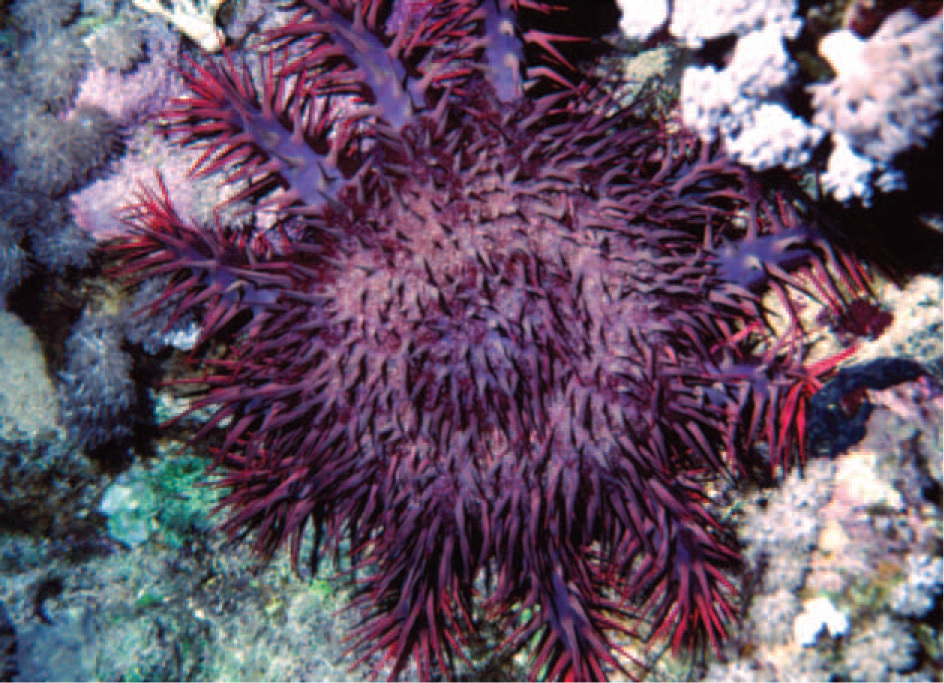
Photograph of the crown-of-thorns in its native environment, a coral reef.
The crown-of-thorns is found on coral reefs in the tropics, Red Sea, Indian and Pacific oceans, and the Gulf of California. These starfish are coral reef predators, feeding on coral polyps by climbing over them and releasing digestive enzymes. At times they pose a hazard to local coral populations.1,2
When an animal is handled or stepped upon, the spines can puncture the skin, causing immediate pain, copious bleeding, and mild edema. A local inflammatory reaction usually follows. A puncture wound usually causes moderate and self-limited (30 minutes to 3 hours) pain. However, it may cause hours of severe pain and swelling that can last for days, depending on the number of spines involved, whether foreign bodies are retained, and the venom burden. Envenomation by the starfish has been associated with nausea and vomiting. 3 Foreign body synovitis, associated with acute monoarthritis, tenosynovitis, and dactylitis has also been reported as a delayed reaction to the local inflammatory response. 4 Multiple puncture wounds may result in localized muscle paralysis. 5
To our knowledge, this is the first documented report of transaminitis in a human envenomed by A planci. Effects on the liver have been demonstrated previously in animal models. Intravenous injection of a purified lethal factor of crown-of-thorns starfish venom in mice has been shown to cause a change in the color of the liver, swelling of the gallbladder, and jaundice. 6 The spine venom was shown to decrease liver microsomal Glutathione S-transferase and cytochrome P450 activity in a rat model. 7 The components of the venom were later identified and further characterized as plancitoxins I and II and noted to have hepatotoxic effects.8,9 Few marine envenomations are associated with documented hepatotoxicity. A species of jellyfish (Phylum Cnidaria, species Chrysaora quinquecirrha) has been shown to induce hepatic necrosis in vitro. 5 Transaminasemia after a sea urchin puncture has been previously reported, but it may have been caused by either the envenomation or by therapy with cephradine and mefenamic acid. 10 In that case, the patient's alanine aminotransferase and aspartate aminotransferase increased to 810 U/L and 320 U/L, respectively.
It remains undetermined in this patient whether the nausea, vomiting, and abdominal pain she experienced soon after the envenomation were due to direct venom effects, hepatitis, a medication reaction, or other cause. However, given the previously studied pathophysiological link between the venom and liver injury, the fairly large dose of venom she may have absorbed (as evidenced by the numerous spines seen on imaging and her pronounced localized inflammatory reaction), and her temporally-related symptom complex, the gastroenteric features may have been caused in part by a hepatic disturbance. It is possible that the nausea and vomiting reported in previous cases of A planci envenomation were due in part to hepatic toxicity. It was felt that her brief syncopal episode was related to her extreme pain.
Failure of her liver enzymes to normalize until after surgical debridement and removal of spine fragments suggests ongoing systemic toxicity from venom present in the spines that remained embedded in her foot. In the event of persistent pain, systemic toxicity, infection, or joint involvement, spine removal should be attempted to limit pain, diminish toxicity, and prevent local inflammatory and infectious complications.
Patients presenting with crown-of-thorns envenomation may become an increasing problem, as animal populations appear to be increasing coincident with increasing numbers of ocean-going individuals, creating a dangerous intersection.
Additional case reports may further delineate the potential for toxicity of the crown-of-thorns starfish in humans. Our experience with this patient suggests that in the event of an apparently severe reaction, it may be prudent to quantify serum liver function tests to determine the presence of a clinically significant venom burden. Furthermore, clinicians should be reminded that envenomation by A planci, and other spined marine creatures, can be exceedingly painful and require the liberal use of narcotic analgesics, nerve block techniques, or other pain control measures.