
Abstract
Okinawa prefecture is a popular tourist destination due to its beaches and reefs. The reefs host a large variety of animals, including a number of venomous species. Because of the popularity of the reefs and marine activities, people are frequently in close contact with dangerous venomous species and, thus, are exposed to potential envenomation. Commonly encountered venomous animals throughout Okinawa include the invertebrate cone snail, sea urchin, crown-of-thorns starfish, blue-ringed octopus, box jellyfish, and fire coral. The vertebrates include the stonefish, lionfish, sea snake, and moray eel. Treatment for marine envenomation can involve first aid, hot water immersion, antivenom, supportive care, regional anesthesia, and pharmaceutical administration. Information on venomous animals, their toxins, and treatment should be well understood by prehospital care providers and physicians practicing in the prefecture.
Introduction
Okinawa prefecture is Japan’s southernmost prefecture, with its main island located approximately 500 km south of Kyushu (the southernmost point of mainland Japan). It has a subtropical climate and is surrounded by coral reefs. The reefs of Ishigaki Island, the Kerama Islands, and Okinawa’s main island make Okinawa a popular tourist destination for recreational divers, snorkelers, and swimmers. With tourism representing 26% of the economy, 1 tourists have a high likelihood of being exposed to the marine environment during their stay. Approximately 10 million tourists visit annually, similar to Hawaii. 2
The reefs around Okinawa are popular, with a tremendous amount of marine life throughout. Although commonly encountered without a direct danger to the swimmer, a variety of venomous species exist within the reefs. Although most envenomations are mild, an understanding of severe envenomation and its sequelae is reasonable for physicians practicing in Okinawa.
This article describes some of the more commonly encountered envenomations around Okinawa prefecture (both clinically seen at our institution and encountered in the environment), with brief descriptions of the venom, clinical findings, and treatment. This overview is aimed toward both the prehospital and hospital care of the patient. Medical providers (both prehospital and hospital) practicing in Okinawa should be familiar with the concerns unique to local marine envenomation.
Marine Animals—Invertebrates
CONE SNAIL—IMOGAI
The cone snail (Conus sp) is a predatory mollusk native to tropical and subtropical waters worldwide. A variety of Conus sp snails exist in the waters around Okinawa, and several are venomous, including the geographer’s cone (Conus geographicus), the textile cone (Conus textile), and the striated cone (Conus striatus) 3 (Figure 1). They are relatively abundant throughout the reefs of the Okinawa islands. The cone snail delivers venom through a harpoon-like device located within a proboscis. The cone snail harpoon can penetrate 5-mm wetsuits, and thus, penetration of skin, even with gloves, is possible.

Examples of cone snail shells found in Okinawa. From left to right: striated cone, textile cone, and geographer’s cone.
The venom itself is a collection of various peptides, with each species producing up to 200 different peptides. 4 Although the various peptides have different actions, they are primarily classified as neurotoxins. In fact, cone snail venom is used clinically in humans, including ziconotide. 5 The venom is able to block the calcium channel Cav2.2 and causes paralysis in prey by blocking acetylcholine release at the presynaptic terminal. 6 Ziconotide is used clinically to treat chronic pain via intrathecal infusion. A variety of clinical responses can be seen with envenomation. Pain, burning, itching, and edema can all be seen locally, while systemic effects range from paresthesias and numbness to respiratory and cardiac arrest. 7 Treatment is generally limited to supportive care. If left untreated, serious cases can result in death in 1 to 8 h. 8
SEA URCHIN—UNI
Sea urchins, part of the Echinoidea class (Echinometra sp, Diadema sp, and others), are ubiquitous in the reefs and water around Okinawa prefecture. Urchins are covered in calcified spines that can easily penetrate skin and are often hidden within the reef (Figure 2). Their venom consists of a variety of different biologically active compounds, including D-galactose–binding lectins, a heparin-binding lectin, glycoprotein Contractin A, and others. 9 Tissue necrosis can occur, and pigment may leak from the spines within the wound.

A large-diameter (30 cm) urchin found within the reef near Sunabe, Chatan, Okinawa.
Local effects of spine puncture typically involve a significant amount of pain but can be a nidus for infection and granuloma formation. Arthritis of the hand has been reported several months after envenomation. 10 Systemic effects include nausea, vomiting, weakness, and respiratory symptoms. 11 No specific antivenoms are available, and the primary mainstay of treatment is supportive care. Urchins have a heat-labile toxin,12,13 and warm water immersion should be attempted when possible. Pressure applied to the wound can worsen symptoms and should be avoided whenever practical. Fasciotomy may be required for significant edema.
CROWN-OF-THORNS STARFISH—TOGEHITODE
The crown-of-thorns starfish (Acanthaster planci) is a venomous starfish present in the reefs and waters throughout the prefecture. It is covered in small spines that can easily penetrate human skin and deliver venom. The venom causes hemolysis and edema, with an estimated median lethal dose of 2.7 mg/kg in mice,14,15 reflecting its relative potency. Other common symptoms include extreme pain at the site with swelling and infection. The spines are very brittle and may require wound exploration and imaging to ensure complete removal. No specific therapy or antivenom currently exists. Supportive care is the primary treatment.
BLUE-RINGED OCTOPUS—HYOMONDAKO
The blue-ringed octopus (Hapalochlaena sp) lives in the shallow reefs and tidal areas around Okinawa prefecture (see online Supplemental Video 1). Although the octopus is a small and docile creature, it is extremely venomous. The primary component of blue-ringed octopus venom is tetrodotoxin (TTX). Interestingly, the TTX is created by bacteria in a symbiotic relationship with the octopus. 16 The TTX is found throughout the entirety of the animal, with the highest concentration in the arms, followed by the abdomen and the cephalothorax. 17
Tetrodotoxin is present in many venomous reef species, including pufferfish. 18 Tetrodotoxin is a sodium channel blocker, preferentially selecting the nerves and motor endplate. 19 There are at least 30 structural TTX analogs, but all contain a guanidinium moiety, and each analog has a different toxicity. Symptoms of TTX intoxication are similar to other sodium channel blockers and appear in a dose-dependent manner. Specifically, this includes paresthesias of the tongue/lips, malaise, headache, vomiting, muscle weakness, ataxia, respiratory depression, and death.
Symptoms generally start 5 to 10 min after exposure, with an initial period of pain at the site followed by systemic symptoms. Treatment largely consists of supportive care. Patients with known exposure should be monitored in an intensive care unit setting for at least 24 h. A monoclonal antibody exists but is not used clinically in humans. 20 Neostigmine has been recommended as a component for supportive care, with consideration of noncompetitive inhibition of TTX through increased concentration of acetylcholine at the neuromuscular junction.21,22 The direct benefit of neostigmine has been called into question. However, with limited specific treatment options, it may be reasonable to consider.23,24 Additionally, glycopyrrolate should be coadministered owing to the risk of profound bradycardia with neostigmine. Like cone snail venom, TTX has been investigated for use clinically in the treatment of chronic pain. Clinically significant reductions in pain have been found in limited studies and may be a novel area for drug development.25,26
BOX JELLYFISH—HAKOKURAGE
Box jellyfish (class Cubozoa) are commonly found in the waters around Okinawa. 27 Jellyfish washed ashore are still venomous even when considered dead. The jellyfish uses specialized structures called nematocysts to envenomate prey. These structures have harpoon-shaped barbs that penetrate the skin, which then allows the nematocyst to deliver venom. 28 The venom varies by species but is generally protein-based and has significant hemolytic, cytotoxic, and hemodynamic effects. 29 It appears to be a sodium channel activator and may indirectly release catecholamines. 30 This catecholamine release may cause a sympathomimetic toxidrome, and patients should be monitored for hemodynamic changes.
Clinical symptoms typically include local severe pain with visible linear tentacle marks on the skin. Systemic manifestations can occur, including severe reactions that can cause respiratory and cardiac collapse, including death. Irukandji syndrome is a related complication that was originally described by exposure to Irukandji jellyfish from Australia. 31 However, Irukandji-like syndromes have been described from exposure to box jellyfish from around the world.32,33 Irukandji syndrome is characterized by a delayed (20–60 min after exposure to jellyfish toxin) reaction of nausea, abdominal pain, hypertension, tachycardia, and even death. 34 Pulmonary edema and cardiomyopathy can develop subacutely in patients with Irukandji syndrome. 35
Treatment involves rinsing the envenomation site with vinegar (4–6% acetic acid) to inactivate the toxin. 36 A pharmaceutical antivenom is clinically available in Australia, but it is not approved by the Food and Drug Administration for use in the United States and is not available in Okinawa. The venom appears to be sensitive to temperature and is inactivated at temperatures >43°C. 37 Hot water immersion has been used clinically with strong response. 38 Regional anesthesia may be considered for symptomatic control of painful extremities. 39 Magnesium has been recommended as a therapy based on its potential to decrease catecholamine activity after envenomation, although the overall benefit is not clear. 40 Because of the sympathomimetic toxidrome that can occur, the patient should be evaluated for hemodynamic changes and a hyperdynamic state. Consideration for evaluation with electrocardiography, creatinine, aspartate transaminase, alanine transaminase, troponin, and chest x-ray may be required in severe cases. Severe hypertension may require multiple vasoactive medications and invasive monitoring, and consideration for treatment of anxiolysis may improve hemodynamics as well.
FIRE CORAL—ANASANGOMODOKI
Fire corals (Millepora sp) are very common in the reefs of the waters around Okinawa (Figure 3). More closely related to jellyfish than true corals, they inject nematocysts with harpoon-shaped barbs, similar to the box jellyfish. The venom is composed of a variety of peptide- and protein-based toxins that cause a variety of effects. 41

Fire corals in the reef near Sunabe, Chatan, Okinawa, with an anemonefish in the foreground.
Clinical symptoms typically involve a localized stinging or burning sensation to exposed skin. Local skin reactions can require treatment similar to that of burns if a significant reaction occurs. 42 Systemic manifestations can occur, although this is uncommon, and local reactions, which can be intense, are more typical. 43 Pain is generally limited to 1 to 2 wk, although subacute nerve palsy has been reported after exposure. 44 Treatment involves local first aid and removal of nematocysts if present. Removal of the nematocyst should include rinsing with 4 to 6% acetic acid (vinegar) solution. Scrubbing and pressure should be avoided. Generally, treatment involves supportive care, including pain control.
Marine Animals—Vertebrates
STONEFISH—OKOZE
Reef stonefish (Synanceia sp) are venomous bony fish. Stonefish lie motionless on the bottom of the reef and are extremely well camouflaged, often with algae growing on their skin matching the surrounding rocks (Figure 4). Because they prefer to sit motionless on the reef floor and are well camouflaged, envenomation typically occurs when patients stand on the reef floor and accidentally step on the stonefish. Clinicians should have a high degree of suspicion for stonefish envenomation in patients who report immediate pain in their feet after standing on a reef floor. Proper buoyancy control for divers is critical to avoid disturbing the stonefish and resultant envenomation. Their dorsal fin spines are hollow and contain venom. The spines are very strong and can penetrate wetsuit boots. The venom contains hyaluronidase, which is composed of hemolytic, edema-inducing, and neurotoxic components. 45 Verrucotoxin is one of the isolated toxins that mediates cardiotoxicity via calcium channel modulation in cardiac myocytes, and animal research suggests that the cardiotoxic effect may be mediated by propranolol administration. 46 Stonustoxin causes hypotension and is myotoxic and neurotoxic.
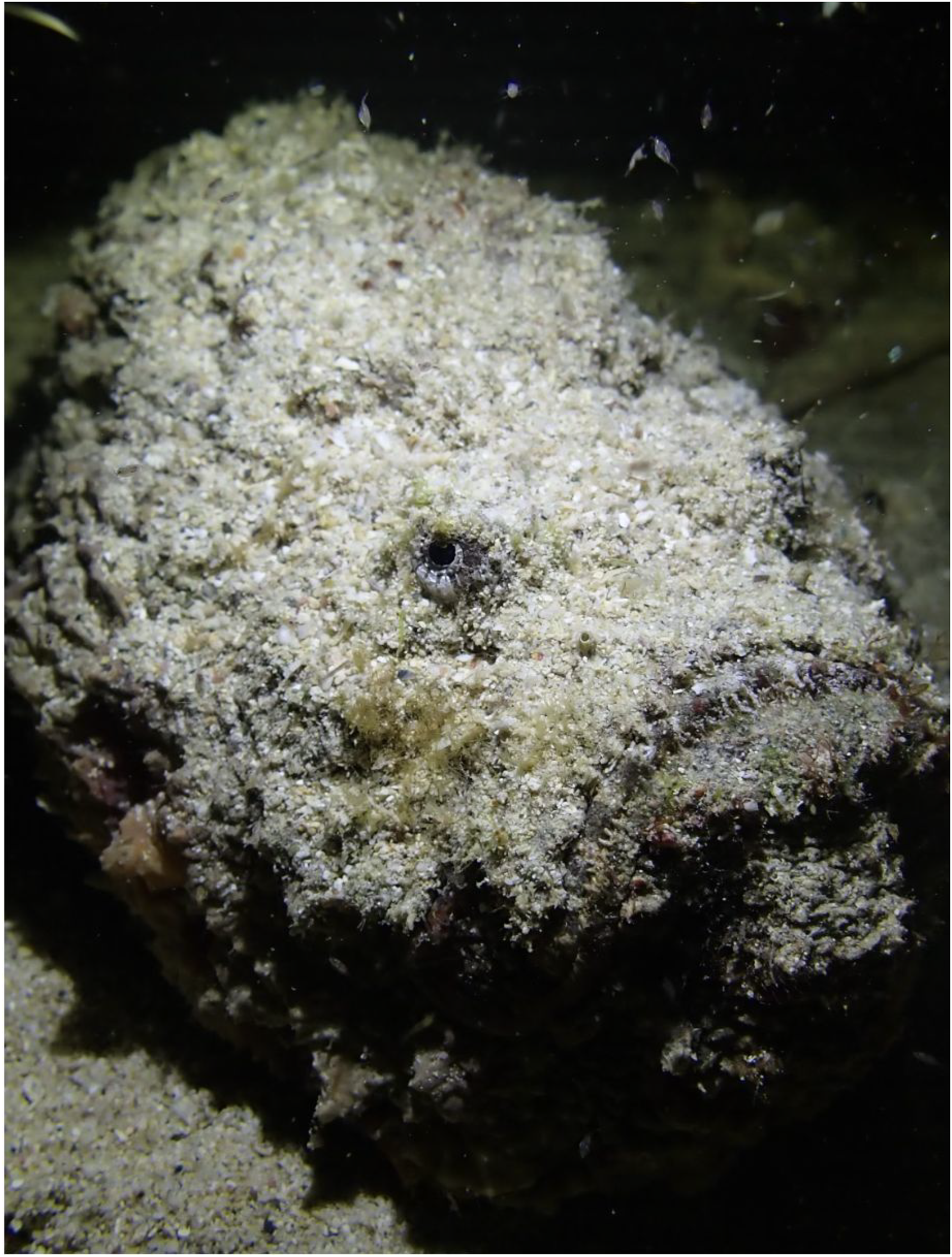
A stonefish resting on the reef near Maeda, Okinawa. Notice the camouflage matching the surroundings.
Clinical symptoms vary from local reactions to systemic effects. Local effects are the most typical response, with intense pain and swelling near the puncture site. Stings to the fingers frequently result in pain and swelling of the entire hand. 46 Compartment syndrome can develop from significant edema. 47 Infection and necrosis of local tissue can also subsequently develop after envenomation. 48 Systemic manifestations include pulmonary edema, 49 hemodynamic collapse, and death. Diaphragmatic paralysis can occur from the neurotoxin, and patients should be treated at a facility that can provide ventilation. In Okinawa, 26% of reported envenomations resulted in severe symptoms. 50 Fortunately, deaths from stonefish are rare in Okinawa, with the most recent reported deaths occurring in 2010 and 1983. 51
Clinical treatment typically involves initial first aid and local wound care, including spine removal if necessary. Stonefish toxin appears to be heat-labile, and hot water immersion in >45°C water for at least 20 min appears to be effective. Observation for compartment syndrome is important in patients with significant edema. Exploration for foreign bodies may be required. Tetanus toxoid and broad-spectrum antibiotics (concern for Vibrio, Aeromonas, Mycoplasma, and Erysipelothrix spp) can be considered owing to the high risk of infection. 52 Because of the risk of paralysis and hemodynamic collapse, supportive care including ventilation may be required. In Australia, antivenom is available for stonefish envenomation, but it is not currently available in Okinawa. Symptoms from the toxin generally start almost immediately and peak approximately 60 to 90 min after exposure, lasting up to 12 h. In cases with severe swelling and tissue necrosis, the patient can develop pain and wounds that may last much longer than 12 h. Fasciotomy may be required for patients with significant swelling.
LIONFISH—MINOKASAGO
The lionfish (Pterois sp) is native to reefs of the Indo-Pacific oceans but is invasive in the Western Atlantic, Caribbean Sea, and the Gulf of Mexico. Lionfish are carnivorous venomous species with few natural predators. They are known to be aggressive toward prey and toward aquatic tourists if bothered (Figure 5). The lionfish is equipped with 12 to 13 dorsal spines, 2 pelvic spines, and 3 anal spines

A lionfish in the waters near Sunabe, Chatan, Okinawa.
Clinical effects are most noticeable, with extreme pain and swelling at the puncture site, followed by paresthesias and widespread myalgias. Systemic effects are seen less frequently; these include tachycardia, hypertension, hypotension, rhabdomyolysis, and paralysis. 56 Treatment includes first aid with local wound care. Patients should have supportive care to manage sequelae of the venom. The venom is heat-labile, and hot water immersion at >45°C should be attempted for at least 20 min. Tetanus prophylaxis should be provided, as should consideration for antibiotic prophylaxis. There is no specific antivenom for lionfish, but there is some cross-reactivity with stonefish antivenom. 57 Lionfish envenomations are rarely severe, and antivenom is infrequently given. Fasciotomy may be required in patients with significant swelling.
SEA SNAKE—UMI HEBI
Sea snakes or sea kraits (Laticauda sp) are semiaquatic venomous air-breathing snakes. They are very frequently encountered throughout the reefs around Okinawa. The snakes are very docile unless provoked and are frequently seen swimming to the surface for air (Figure 6). Generally, the snakes are provoked when divers or swimmers attempt to grab them while swimming. Laticauda venom is reportedly extremely toxic. A single snake is able to kill 3 average-sized adults, 58 and the case fatality rate is 3%. 59 The venom is similar to other snake toxins, with nephrotoxic, hepatotoxic, neurotoxic, and myotoxic effects. The neurotoxin binds nearly irreversibly to both the presynaptic and postsynaptic junction of the acetylcholine receptors, resulting in peripheral weakness, including respiratory function. 60 The clinical syndrome is consistent with a generalized blockade of the neuromuscular junction.

A sea snake swimming near the reef in Chatan, Okinawa.
Symptoms may include malaise, slurred speech, blurred vision, motor weakness, respiratory distress, paralysis, and death. 61 General loss of muscle tone can be expected. Clinical management involves initial first aid to the wound. An Australian antivenom exists, but it is not available in Okinawa. 62 Early intubation and mechanical ventilation may be required, and early transport to a robust medical facility should occur as soon as reasonably possible. Warm water therapy may worsen the symptoms and is relatively contraindicated for sea snake envenomation.
MORAY EEL—UTSUBO
Moray eels (Muraenidae sp) are commonly found throughout the world and are prevalent throughout the reefs around Okinawa. Multiple species exist, and they come in a range of sizes (see online Supplemental Video 2). The primary concern with the moray eel is their strong bite. Although the moray eel is not venomous, they do accumulate ciguatoxin in their tissues, which may cause poisoning when consumed. 63 The eels themselves are often hidden within the reef, and divers may be bitten when they reach into holes within the reef. The jaws of the eels are strong with very sharp teeth. This combination can cause significant tissue damage. There are reports of crush injury 64 and persistent disability after eel injury. 65 Furthermore, the various marine types of flora in their mouth can cause significant problems if the bite becomes infected.
Treatment involves first aid and stabilization of the injury. These injuries can cause significant bleeding, which can attract other predatory species. Egressing the water immediately is of utmost importance. Typical wound care is indicated, but more invasive wounds may require surgical debridement or operative fixation for bony deformity. Antibiotic prophylaxis should be strongly considered, especially for Pseudomonas and Vibrio coverage.
Treatment Approach
The general treatment approach is to first provide safety at the time of injury. If the patient is in the water, generally, we recommend getting to land or surfacing to a boat. First aid should be performed as soon as possible. This includes control of life-threatening hemorrhage. Tourniquets and tight-fitting bandages should be avoided whenever possible. For hemorrhage control, pressure dressings are preferred over tourniquets unless life-threatening hemorrhage is involved. For jellyfish and fire coral, nematocysts should be removed if present. Acetic acid 4 to 6% can be applied to neutralize venom and may be considered in all patients with an unclear envenomation. Sea water can be used to rinse when acetic acid is not available, but caution should be used to ensure toxic particulates, such as jellyfish tentacles, are not present in the water.
Attempts should be made to identify the envenomating animal if possible. Snake, eel, and stonefish bites are generally immediately noticeable, but jellyfish and coral envenomation may not be immediately apparent. Photos, description, animal habitat, and patient activity can help identify the type of envenomation that occurred. Similarly, activity type may help with the diagnosis. Beachcombers may be more exposed to urchin, while divers may be more exposed to stonefish. Box jellyfish and fire coral usually cause erythema at the site of skin contact, which may be helpful in diagnosis. Crown-of-thorns starfish, urchin, stonefish, lionfish, sea snake, and eel injuries have soft tissue wounds, although sometimes differentiating these from one another can be challenging. The nature of the activity can be helpful in identifying the animal as well, for example, if the patient was standing on the reef floor and has a puncture wound on the foot, typical for stonefish envenomation.
Severe symptoms should prompt immediate travel to a hospital or robust medical facility. For patients who are exposed to marine envenomations in more remote parts of Okinawa prefecture, strong consideration should be made for traveling to a medical facility, even if only mild symptoms persist. Symptoms prompting immediate transport to a medical facility include local reactions, intense pain, significant edema, and hemorrhage or presence of any systemic symptoms, such as nausea, fatigue, weakness, respiratory distress, and hemodynamic changes. Consideration for antivenom should be given. Many of the toxins are heat-labile and respond to hot water immersion, although this can worsen symptoms after sea snake envenomation and should be avoided if there is a reasonable suspicion of sea snake envenomation. In serious cases, supportive care may require intensive care–level facilities for care and monitoring. Patients with significant swelling and edema may develop compartment syndrome and require prompt evaluation with surgery for fasciotomy. Similarly, wounds may require exploration and debridement.
At a robust medical facility, patients with open skin wounds should be evaluated for foreign bodies. Of the discussed animals, sea urchin, crown-of-thorns starfish, lionfish, stonefish, and fire coral can leave foreign bodies; therefore, a thorough evaluation of the wound should be performed, with strong consideration for imaging. Prophylactic antibiotics should be given for deep puncture wounds, but they may be considered for any open wounds depending on the severity and location of the injury. Prophylactic tetanus vaccination should be updated for patients with open wounds. For patients with severe symptoms, the Japan Poison Information Center should be consulted for treatment guidance. This is especially important prior to administration of antivenom and with critically ill patients. Despite the potential of some of the more potent envenomations, rapid diagnosis and subsequent treatment in a robust medical facility generally result in lower risk of morbidity and mortality.
Conclusion
Patients who are exposed to marine envenomation should receive prompt treatment. Identification of the animal should be made whenever possible. Ongoing tourism and exposure to the thriving marine environment in the waters throughout Okinawa prefecture make marine envenomation a possible risk. Awareness of the potential animal species, their toxins, and treatment is important for prehospital providers and physicians practicing throughout the prefecture.
Supplemental Material
Supplemental Material
Footnotes
Author Contribution(s)
All authors contributed significantly to the ideation of the project, the background research, the manuscript creation, and final approval of the manuscript.
Disclosures
The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the US Government. The authors are military service members. This work was prepared as part of their official duties. Title 17 U.S.C. 105 provides that “Copyright protection under this title is not available for any work of the United States Government.” Title 17 U.S.C. 101 defines a US Government work as a work prepared by a military service member or employee of the US Government as part of that person’s official duties.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.