
Abstract
Objective
To study the changes in pulmonary function of human male volunteers from 2 different populations: Indians and Kyrgyzis before and after ascent to 3200 m and during a 4-week stay at that altitude.
Methods
Ten healthy soldiers of the Indian army (22–25 years of age) and 10 Kyrgyzis recruits (19–20 years of age), height and weight matched, were volunteers in this study. Their pulmonary functions were evaluated at baseline (Bishkek, 760 m); on days 2, 13, and 25 at a mountain clinic at Tuya Ashuu pass (3200 m) in the northern Tien Shan Range; and on return to Bishkek. A dry spirometer was used to measure lung function at each location.
Results
Results indicated that Kyrgyzis had significantly larger forced vital capacity (FVC) and forced expiratory volume in 1 second (FEV1) than those of the Indians, but their peak expiratory flow rate (PEF), forced expiratory flow rate at 25% to 75% of FVC (FEF25–75%), and maximal voluntary ventilation (MVV) measures were comparable. At high altitude (HA), FVC showed significant reduction on day 2, with subsequent recovery in the Kyrgyzis; but in the Indians, FVC showed gradual reduction, and on day 25, it was significantly reduced compared with the baseline value. FEV1 did not show any change with altitude in either group. Expiratory flow rates and MVV showed significantly higher values at HA in both groups. However, after air density correction for the 2 altitudes, PEF and MVV showed no changes from their baseline values, and the mid-expiratory flow rate (FEF25–75%) was actually reduced in both groups: on day 2 in the Kyrgyzis and on day 25 in the Indians. On day 2 of return from a 4-week stay at HA, all test measures were back to their baseline values.
Conclusions
The major difference between the 2 populations was larger lung volumes in the Kyrgyzis compared with the Indians, with no differences seen in their flow rate measures. Also, there was a different time schedule of altitude-induced reductions in FVC and FEF25–75%.
Introduction
On exposure of sea level dwellers to hypobaric hypoxia at high altitude (HA), changes are seen in several physiologic functions that are generally related to oxygen transport and metabolic rate. Increase in pulmonary ventilation occurs during the early days of acclimatization. However, no great alterations in lung volumes and mechanics have been implicated. The larger lung volumes generally reported in highlander natives seem to be in response to the hypoxic environment that is encountered by the individual during his early phase of growth.1,2 In the sojourners, lung volumes are likely to be compromised with ascent to HA. 3 –7 A progressive drop in forced vital capacity (FVC) on ascent beyond 2000 m has been reported. 5 The reduction in FVC has been recorded to be immediate and sustained, and this is affected by an abrupt increase in intrathoracic fluid volume on arrival.4,8 On the other hand, there are varying reports regarding the net result of the effect of HA on expiratory flow parameters: some indicating reductions in the flow rates and maximal voluntary ventilation (MVV) 9 and others observing improvements. 10 It is quite likely that the improvement seen in ventilatory flow rates are affected simply by the physical factor of a reduced density of air from the hypobaria of the mountains, and an appropriate air density correction will show the true response. 1 Also, ethnicity might have a role in HA-related changes in pulmonary functions, thus resulting in possible variations in different reports. Lung volumes and capacities are known to exhibit strong ethnic differences. 11 –13
We had the opportunity to study the changes in pulmonary function on acute ascent and during a 4-week stay at an altitude of 3200 m in human male volunteers from 2 different populations: Indians and Kyrgyzis.
Methods
Twenty normal healthy men (10 Kyrgyz and 10 Indian), in the age range of 19 to 25 years, were selected from the combatant populations of the respective Armed Forces. They were randomly selected from the respective Army units with the help of a random number table. However, care was taken to see that they did not have a previous HA exposure (defined as >3000 m).
Kyrgyz volunteers were slightly younger (mean age, 19.4 ± 0.5 [SD] years; range, 19–20 years) compared with the Indians (mean age, 23.5 ± 1.0 [SD] years; range, 22–25 years). Their body size was, however, fairly matched. The mean height of the Kyrgyzis was 174.3 ± 2.8 cm (range, 169–176 cm), and mean body weight was 64.0 ± 4.0 kg (range, 56.0–71.5 kg). The mean height of the Indians was 172.8 ± 2.7 cm (range, 169–174 cm), and mean body weight was 63.3 ± 5.2 kg (range, 58.0– 72.5 kg). The study protocol was approved by the Institute's Ethics Committee, and an informed consent was obtained before participation. Subjects were free to withdraw from the study without prejudice at any time.
Pulmonary function tests (PFTs) were performed using a calibrated dry spirometer (Model Ponygraphic; Cosmed srl, Rome, Italy) using standard techniques (as per American Thoracic Society standard/protocol). Test parameters reported in body temperature and pressure, saturated with water vapor (BTPS), were forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), peak expiratory flow rate (PEF), forced expiratory flow rate 25% to 75% (FEF25–75%), and maximal voluntary ventilation (MVV). Baseline measurements were at Bishkek (760 m above sea level; barometric pressure, 694 mm Hg). After traveling by road in a motor transport (on the same day) to a mountain clinic (3200 m; barometric pressure, 513 mm Hg) at Tuya Ashuu Pass in the northern Tien Shan range in Kyrgyzstan, PFTs were studied on days 2, 13, and 25 of sojourn and on day 2 after return to Bishkek. The best of 3 measurements of respiratory functions were taken for analysis. For comparison, HA values of flow rate parameters and MVV for the 2 altitudes (Bishkek: barometric pressure, 694 mm Hg; HA clinic at 3200 m: barometric pressure, 513 mm Hg) were corrected for air density to expected values at sea level (SL). The formula used for gas density correction was:
Statistical analyses were carried out using repeated-measures analysis of variance to compare the changes in PFT parameters on various days. When the F-ratio reached the significance level (P < .05), pair-wise comparisons were performed using the Dunnett test. All analyses were executed using SPSS 14.0 for Windows. 14
Results
The sequential pulmonary function parameters in the Kyrgyz and Indian volunteers are shown in Table 1. During the entire period of the study, the lung volume parameters (viz FVC and FEV1) were found to be significantly higher (∼13%–17%) in the Kyrgyz group compared with the Indians. Flow rate parameters including MVV values were, however, comparable between them.
Respiratory parameters of Indian and Kyrgyz volunteers at baseline and on ascent to high altitude‡
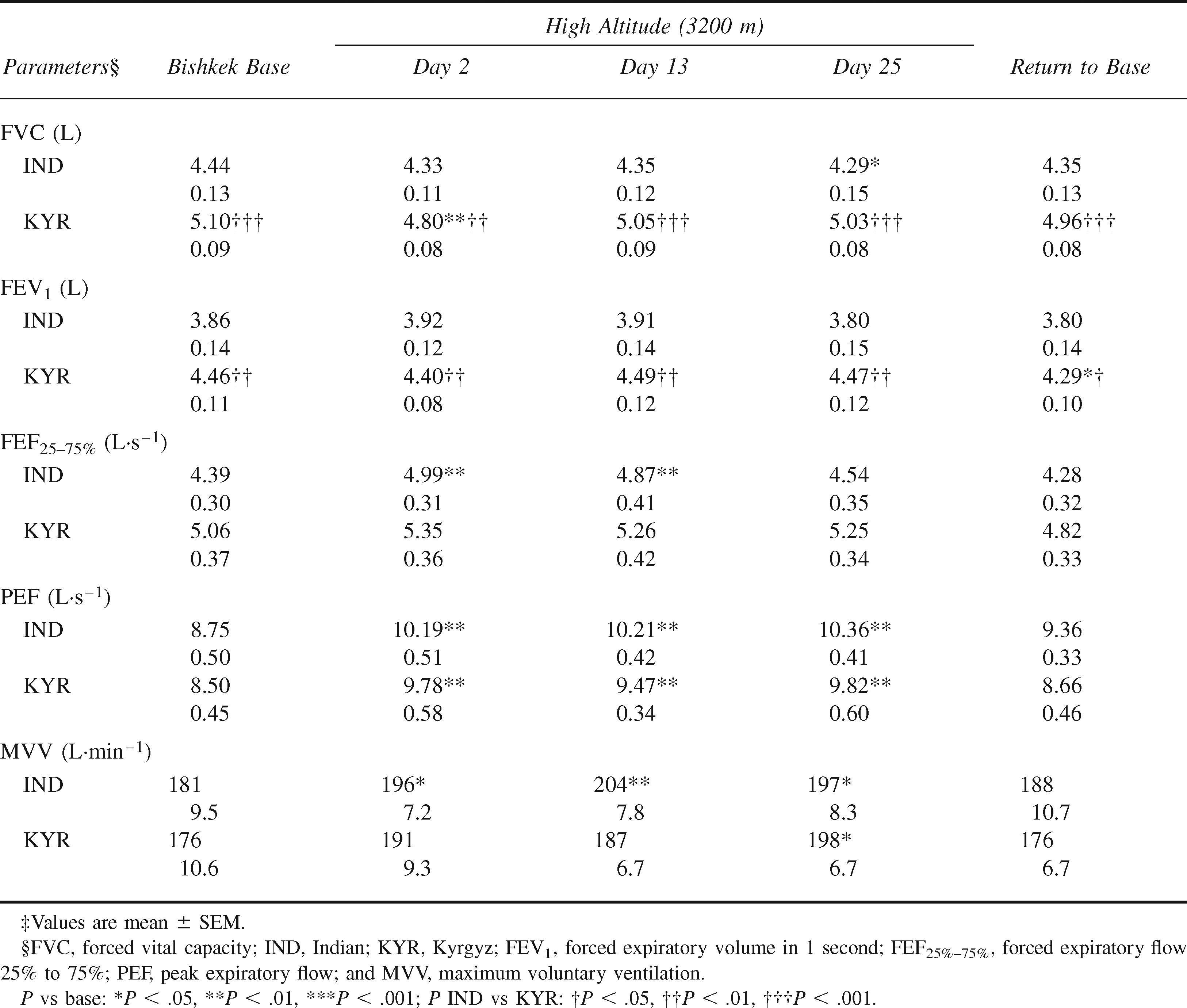
Both groups showed a decline in FVC on reaching HA. In Kyrgyz subjects, decrement in FVC on day 2 (300 mL, ∼6% reduction from baseline, P < .01) was highly significant. Subsequent measurements on days 13 and 25 showed recovery almost to baseline. Indians, on the other hand, showed their lowest mean value of FVC on day 25 of sojourn, with a mean reduction of 150 mL (∼3%, P < .05) from the baseline. FEV1 did not show any significant differences with ascent and acclimatization to HA.
All the 3 major flow rate measures of PFT, namely PEF, FEF25–75%, and MVV, showed significant increases at HA in both groups. Mean values of PEF showed increases of 15% to 16% on day 2 of ascent to HA. MVV increased ∼8% to 9%. These increases were maintained during the 4 weeks of sojourn at HA. In terms of mean FEF25–75%, increases on immediate ascent were 13% in Indians and 6% in the Kyrgyz. In Indians, the initial increase in FEF25–75% was reversed during the sojourn.
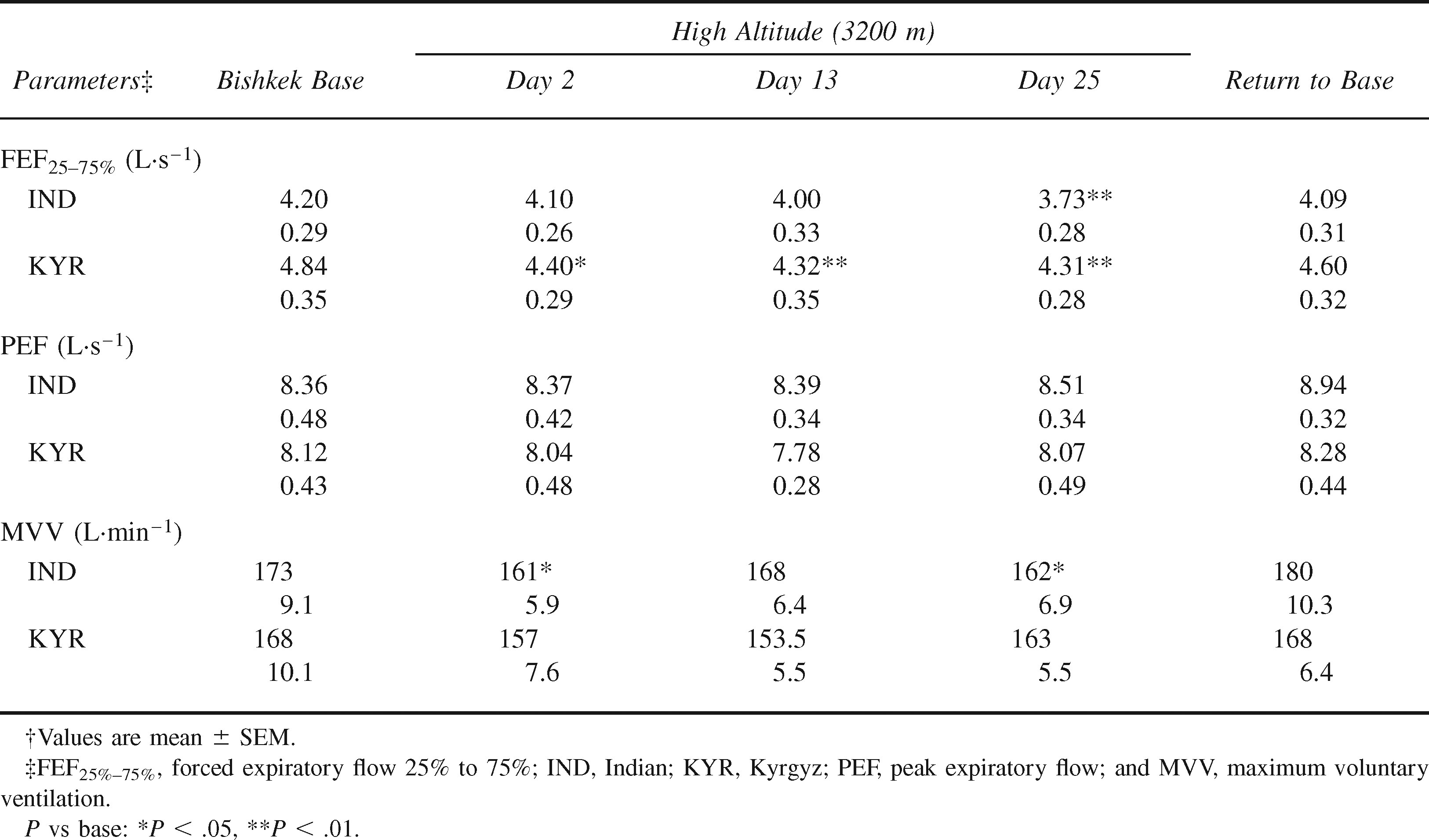
After air density correction, as applied to SL barometric pressure, PEF remained essentially the same at HA. In terms of FEF25–75%, there were significant reductions with HA ascent in Kyrgyzis, and the decrement was significant during the entire stay at HA. However, in the Indians, significant reductions were seen only on day 2 (Table 2). MVV was not affected in Kyrgyzs, but the Indians showed significant declines on days 2 and 25. On return to base, all PFT parameters returned to baseline values in both groups.
Respiratory flow rate parameters and maximum voluntary ventilation of Indian and Kyrgyz volunteers after air density correction†
Discussion
Kyrgyzstan is a mountainous country, with 57% of its total land area being above 2500 m. However, the Kyrgyzis volunteers in this study were natives of low to moderate altitude and not from HA, as defined as >3000 m above sea level. Indian soldier volunteers were consciously selected from low-altitude dwellers.
The lung volume parameters were found to be significantly higher in the Kyrgyz group compared with the Indians. Comparatively lower lung volumes and flow rates in Indians than those in the Europeans, North Americans, and West Asians, even after corrections for age, height, and weight, have been reported by many.12,13 However, in this study, the flow rate values including MVV were not found to be different between the 2 groups when compared with baseline. High lung volumes with normal expiratory flow rates may be a characteristic profile of the Kyrgyzis. A similar kind of observation of significantly higher lung volumes but comparable flow rates was made in the highlanders of Peru compared with a matched low-altitude population. 1
While looking at the changes on ascent to HA, both subject groups showed decreases in FVC. In Kyrgyz subjects, decrement in FVC on day 2 (by 300 mL, ∼6% reduction from baseline, P < .01) was highly significant. Subsequent measurements on days 13 and 25 showed substantial recovery. Indians, on the other hand, showed the lowest mean value of FVC on day 25 of sojourn, with a mean reduction of 150 mL (∼3% from baseline, P < .05). A reduction in FVC on ascent to HA has been a general observation in previous studies, 4 –7,15 and the most plausible mechanisms are an increase in thoracic intravascular volume and increased pulmonary extravascular fluid accumulation caused by hypoxia. In respect to FEV1, no changes were seen on arrival and acclimatization to HA in either group.
Without correction for air density, all the 3 major flow rate measures of PFT (viz, PEF, FEF25–75%, and MVV) showed significant increases at HA in both groups of subjects. Mean values of PEF showed increases of ∼15% on day 2 of ascent to HA. That of MVV showed increases of 8% and 9%. These increases were maintained all through the 4 weeks of sojourn. In terms of mean FEF25–75%, increases on immediate ascent were 13% in the Indians and 6% in the Kyrgyz. Without air density correction, increases in expiratory flow rates at altitude were seen in earlier studies, both in normal healthy subjects1,3 and in patients with obstructive airway diseases. 16 However, these increments of flow rate measures of pulmonary functions are caused primarily by the physical flow dynamics as affected by hypobaria. After air density correction, FEF values remained essentially unchanged on ascent and acclimatization to HA in both groups (Table 2). In terms of FEF25–75%, air density–corrected values indicated reductions with ascent to HA, and the decrement was significant on day 2 in the Kyrgyzis and on day 25 in the Indians. Both populations showed reductions in MVV on ascent to HA. Although the Indians had significant reductions during the sojourn, the decline in Kyrgyzis was not significant. Brody et al 1 observed reductions in flow rates in a majority of individuals on ascent to 3850 m altitude after air density corrections were made.
The temporal pattern of response in the mean value of air density–corrected FEF25–75% was found to be different in Indian and Kyrgyz subjects. Kyrgyz subjects showed significant reduction in FEF25–75% on day 2 at HA, and the effect was sustained. Indians, on the other hand, showed significant reductions only on day 25. It is worthwhile to note that Indians exhibited a similar temporal reduction in FVC late during acclimatization and not on initial altitude exposure. FEF25–75%, which is a measure of patency of the smaller airways in the lungs, is affected by the elastic behavior of the airways and their surroundings. Increased intrathoracic fluid volume on exposure to HA is thus likely to affect a decrease in the FEF25–75%. We have no explanations for the differences in the time course of the event in the 2 groups of subjects. Nevertheless, the 2 major differences observed between the 2 populations are 1) larger lung volumes in the Kyrgyzis and 2) different temporal responses in the decrement in FVC and FEF25–75% on exposure to HA. However, our longitudinal study is limited in that it could only be conducted on a small number of volunteers, and it is, therefore, only possible to observe general directions of major changes occurring in the different environmental conditions. Further research on different populations and larger sample sizes may reiterate the findings and their possible mechanisms.
It was interesting to note that all the HA-induced changes were highly reversible. On day 2 of return from HA, PFT values were found to have come back to their baseline levels in both groups. Thus, HA-related changes seen in the pulmonary volumes and mechanics on initial exposure and early days of acclimatization are caused by short-term adaptive changes that promptly return to baseline on descent.
Conclusion
On the basis of our findings of the pulmonary function measurements in Indian and Kyrgyzis volunteers at baseline and on a 4-week sojourn at an altitude of 3200 m, the following conclusions are drawn. 1) Indian subjects had lower values of volume functions of the lungs (viz, FVC and FEV1) compared with their Kyrgyz counterparts but their flow rate functions as shown in PEF, FEF25–75%, and MVV were comparable. 2) At HA (3200 m), there were significant reductions in FVC in both groups. Kyrgyzis showed a reduction in FVC on acute exposure that recovered with acclimatization. Indians showed a different time course, with FVC showing its lowest value on day 25. FEV1 did not show any changes with sojourn in either group. 3) Pulmonary flow rates, as measured directly, were found to be significantly increased at HA, but these increases seem to be affected by the reduction in air density with no functional improvements in the pulmonary system per se. On air density correction, PEF showed no changes at HA. MVV showed a decline on ascent to HA in both groups, Indians being affected significantly. FEF25–75% was also found to be reduced at HA. In Kyrgyzis, it was affected from day 2 of the sojourn, whereas in Indians, it was reduced later (ie, on day 25 of exposure). 4) HA sojourn of 4 weeks at 3200 m was found to have no lasting effects on pulmonary volumes and mechanics because all measured values returned to baseline by day 2 of return to an elevation of 760 m.
Footnotes
Acknowledgments
The authors thank the Kyrgyz and Indian volunteers for their utmost cooperation in this study.
Funding
This study was funded by the Defence R&D Organisation, Ministry of Defence, Government of India.