
Abstract
Objective
Tibetans and Sherpas have long been revered for their physical aptitude at high altitude, and are thought to have lived at high altitude longer than any other culture. We performed physiologic testing on 2 Sherpas who currently hold world records for: (1) most number of ascents of Mt Everest and (2) speed ascent of Mt Everest from base camp to the summit. In doing so, we describe certain physiological aspects of these individuals that may contribute to their abilities at altitude.
Methods
Anthropometric measurements, blood testing, and electro- and echocardiographic examination as well as pulmonary function tests were performed. Exercise testing consisted of treadmill climbing at increasing incline and speed while wearing a 22 kg backpack in Salt Lake City (1325 m) and Park City (2063 m).
Results
Anthropometry, electrocardiography, pulmonary function, strength, and echocardiography were consistent with predicted parameters for the general population. The Sherpas demonstrated appropriate cardiopulmonary response to dynamic exercise similar to moderately fit individuals while performing treadmill testing, both at moderate and high altitude. As expected, the energetic cost increased at higher altitude, likely due to increased respiratory work.
Conclusion
The 2 world-record Sherpa climbers were within normal ranges for the specific measurements that were tested. They displayed appropriate cardiopulmonary and physiological responses and exercise performance profiles at moderate and high altitude.
Keywords
Introduction
High-altitude natives have long been respected for their physical strength and prowess at altitude. The Sherpas of the Himalaya migrated from the Tibetan plateau to the mountainous areas of Nepal approximately 400 years ago, and are considered of Tibetan lineage. Historically, they are believed to have resided at high altitudes for over 25 000 years, longer than any other prehistoric or modern culture. 1 -6 Sherpas were integral in early exploration of the Indian and Nepal Himalaya well before mountaineers set their sights on high mountains. Since the first British exploration of Mt Everest in 1921, Sherpas have participated in every expedition on the mountain. 7 The strength and endurance of the Sherpa people at high altitude is legendary.
Previous reports suggest that the Sherpas are genetically adapted to the high environment. Their metabolic cost while carrying loads is generally less than matched Caucasians. 8 Sherpas have a larger total lung capacity and larger vital capacity compared to their lowlander counterparts. 6 ,9-11 As a result, they are anatomically and physiologically adapted to the high-altitude surroundings.
We report physiological, hematological, and anthropometrical characteristics of 2 record-holder Sherpas. These 2 men occupy a distinctive place in Sherpa and Everest history, and may possess physiological characteristics that set them apart from other Sherpas and high-altitude mountaineers. This information may help characterize the physiology of these individuals and contribute to the growing body of knowledge of Sherpas' ability at altitude.
Methods
The subjects spoke English well, were explained the procedures, and gave written and verbal consent accordingly.
Subjects
Subject 1 was born in Thame, Nepal, at an altitude of 3900 m. He currently holds the record for the most ascents of Mt Everest. In 1987, he began working as a porter for Everest expeditions. He was noted to have exceptional strength at high altitude and was consistently carrying heavier loads, and in a faster time, than other high-altitude porters. He began working as a climbing Sherpa in 1988.
He has reached the summit of Mt Everest every year from 1990 through 2010 inclusive (with the exception of 1996, during which he did not participate in an Everest expedition). As of May 2010 he has stood on the summit of Mt Everest a total of 20 times, 4 of these without the use of supplemental oxygen. He was 47 years old on the day of testing.
Subject 2 was born in Karicola, Nepal, at an altitude of 2130 m. He holds the record for the speed ascent of Mt Everest, racing from the Nepal base camp at 5400 m to the 8848 m summit in 10 hours 56 minutes 46 seconds. He used oxygen from Camp IV (8000 m) to the summit. He has reached the top of Mt Everest a total of 13 times, all with supplemental oxygen. He was 40 years old on the day of testing.
The subjects were tested approximately 1 month prior to a Mt Everest expedition. They had been living in Salt Lake City (elevation 1325 m) for approximately 6 months prior to testing. Therefore, the subjects were acclimatized to this altitude and had not been exposed to extreme altitudes for over 6 months.
Procedures
General physical examination and hematological techniques were performed in Salt Lake City, UT, according to standards of The Orthopedic Specialty Hospital in Salt Lake City and the University of Utah Health Center.
Anthropometry
Body weight was determined using a digital scale to the precision of 0.1 kg (Conair, East Windsor, NJ). Height was measured with a fiberglass tape measure to the nearest 0.1 cm (Eslon, Sekisui Jushi, Japan). Skinfolds were measured twice at 5 sites: chest, midaxillary, subscapular, abdominal, and suprailiac, using a Lange skinfold caliper (Cambridge Scientific Industries, Cambridge, MD) to the accuracy of 0.1 mm. Body fat equations specific to the Asian population have not been validated in athletes. Therefore, body fat was calculated by summing the average of each site and using the 7-site equation by Jackson and Pollock, 12 which is the standard for male athletes.
Electrocardiography
Electrocardiograms were recorded on an Auto Cardiner FCP-2201 ECG machine in standard 12-lead configuration (Fukuda Denshi Co. Ltd, Tokyo, Japan).
Pulmonary Function
Pulmonary function tests (PFTs) were performed on a metabolic cart equipped with a spirometer (TrueOne 2400, ParvoMedics, Sandy, UT) that was calibrated for flow and volume to ±0.01% via a 3L syringe (Hans Rudolph, Kansas City, MO) and calibrated to references gases (16% O2, 4% CO2, balance N—Scott Specialty Gases, The Netherlands) at atmospheric air.
The accuracy of a PFT is highly dependent on the effort given; therefore, subjects were given instructions as to how to perform the test and were allowed a habituation trial. PFTs were performed prior to exercise testing to determine baseline lung function. During testing, a clip was placed over the nose while the subjects breathed through their mouths into a mouthpiece connected to the spirometer. The PFT consisted of taking a maximal inhalation followed by a maximal exhalation for approximately 5 seconds. Each subject performed 3 tests, with the best of the 3 trials used as the baseline lung function.
Strength
Each subject's leg strength was assessed during a maximal voluntary contraction (MVC) on a custom force plate (3PQ, Advanced Mechanical Technology, Inc., Watertown, MA) mounted on a leg press machine fitted with a displacement sensor (UniMeasure, Inc., Corvallis, OR). After familiarizing the subjects with the equipment and following a standard warm-up protocol, leg strength was measured unilaterally in a supine position at a knee flexion angle of 120°. Subjects were instructed to push as forcefully into the force plate as possible for 5 seconds with the weight stack locked to insure that no movement of the leg press sled could occur. Three separate measurements were taken with a 90-second rest interval between trails, with the average result recorded.
Echocardiography
Two-dimensional and Doppler echocardiographic images were obtained from standard windows as described by the American Society for Echocardiography. 13 Harmonic imaging was performed with a Sequoia 512 echocardiographic system (Siemens, Mountain View, CA).
Exercise testing and oxygen consumption
Testing high-altitude natives on a bicycle ergometer has been questioned because people of these cultures are not typically familiar with this activity. 14 Similarly, running on a treadmill does not replicate motions familiar to most people of the Sherpa culture. 15 Subjects in our study were adept at climbing (but not running or cycling); therefore, were tested while walking on an inclined treadmill wearing a backpack weighing 22 kg. These conditions were chosen to simulate those encountered during a typical Everest climbing expedition.
Subjects were familiarized with the equipment during a practice session prior to the formal testing. Exercise treadmill testing was performed both in Salt Lake City (1325 m) and Park City (2063 m) with 5 days separating sessions. Both sessions were performed following an incremental protocol of 3 steps at submaximal effort. Speed was set and kept constant at 1.4 mph (2.24 kph). The subjects exercised for 8 minutes at each of 3 grades: +25%, +30%, and +35%. Testing was paused for 20 seconds at 8, 16, and 24 minutes to record blood pressure. The stage lengths were set at 8 minutes in order to achieve a steady state phase long enough for metabolic analysis and also to replicate the constant and moderate effort typical of high-altitude mountaineering. At the end of the Park City session, the protocol was extended by increasing the incline by 2.5% each minute until subjects attained voluntary exhaustion. These values were considered “peak” for our study conditions instead of “maximum” because maximal criteria (HR > 85% of maximum predicted, R > 1.1, and blood lactate concentration > 8 mmol/L) were not entirely fulfilled.
Ventilation (VE) and oxygen uptake (VO2) were measured and respiratory exchange ratio (RER) calculated by conventional open-circuit spirometry (ParvoMedics, TrueOne 2400, Sandy, UT). The system was calibrated according to the methods described above for the pulmonary function testing. All parameters were continuously recorded and reported over 20-second averaging periods during the entire test. Heart rate was monitored by a heart rate monitor (Polar NV, Kempele, Finland).
Protocols were reviewed and approved by the University of Utah Institutional Review Board.
Results
Body Composition, General Physical, Physiologic, and Hematological Exam
The general exam of Subjects 1 and 2 revealed heights of 160 and 180.3 cm, weights of 55.3 and 75.3 kg, hematocrit values of 39.3 and 46.2%, and hemoglobin values of 13.6 and 16.1 g/100 mL, respectively. Both Sherpas were normal body weight with Body Mass Indexes (BMI) of 22 and 24.6 kg/m2, respectively (normal range for adults: 18.5–24.9). 16 Skin fold measurements for Subjects 1 and 2, respectively, were as follows: subscapula 11 and 12 mm, chest 7 and 13 mm, tricep 7 and 7 mm, midaxillary 8 and 12 mm, suprailiac 7 and 10 mm, abdominal 17 and 20 mm, thigh 9 and 7 mm, with the sum of these equaling 66 and 81 mm. The Sherpas were not extremely lean with body fat percentages measuring 28.2% and 27% for Subject 1 and Subject 2, respectively.
Electrocardiogram
Electrocardiograms of both subjects showed normal sinus rhythm, normal PR and QRS intervals, no arrhythmia or ectopy, and no evidence of right heart strain pattern.
Pulmonary Function Data
Pulmonary testing results are reported in Table 1. Overall, Subject 1 performed slightly below and Subject 2 slightly higher than predicted for age, gender, size, and race at the altitude at which they were tested. 17
Pulmonary function testing results
FVC = forced vital capacity; FEV = forced expiratory volume; FEF = forced expiratory flow; PEF = peak expiratory flow.
Strength Test
Maximum voluntary contraction results for Subject 1 yielded 73 kg (131.0% of body weight) for the right leg and 69 kg (124.5% of body weight) for the left leg. Subject 2 recorded maximum voluntary contraction results of 82 kg (108.4% of body weight) on the right and 75 kg (99.4% of body weight) on the left. Subject 1 had a higher body weight to peak force ratio (BW:PF) than did Subject 2 on both legs (right leg = 131% vs. 108.4%; left leg = 124.5% vs. 99.4%).
Echocardiogram
Transthoracic echocardiograms showed normal chamber sizes in both individuals. 18 Systolic function of both the right and left ventricles, as assessed by the left ventricular ejection fraction, did not show any abnormalities. Measurements of left ventricular diastolic filling, as assessed by transmitral flow patterns, were within normal limits. Tricuspid regurgitation was graded as “trace to mild” in both subjects. There were no significant structural valvular abnormalities, and neither subject had more than trivial regurgitation of any valve.
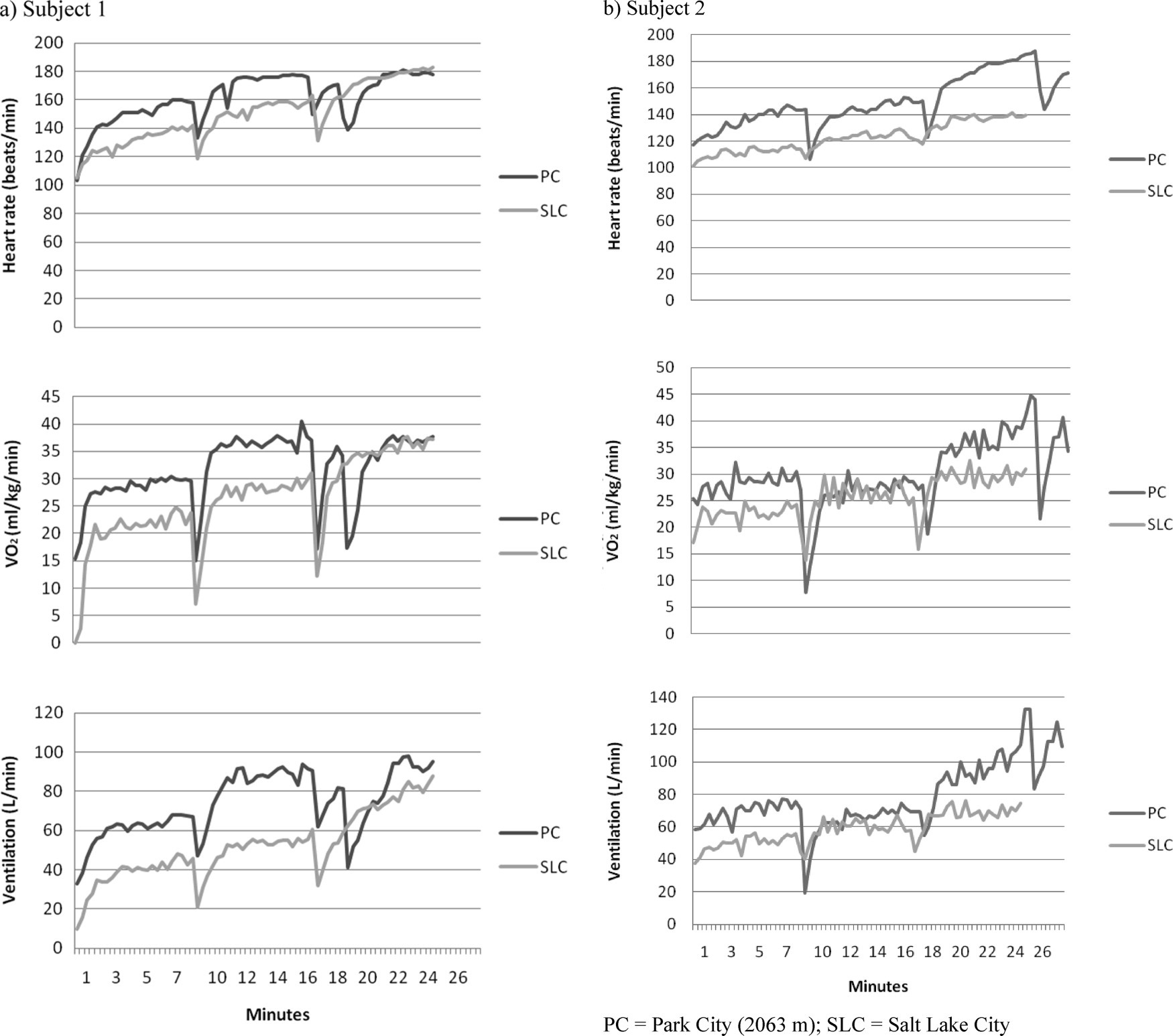
Exercise Testing
Subjects showed an overall appropriate cardiopulmonary response to incremental exercise at altitudes of 1325 and 2063 m with physiological (ie, nonpathological) increases in ventilation, oxygen uptake, and heart rate (Figure). They did not develop any symptoms (eg, chest pain, palpitations, shortness of breath) during or after the test. Peak results during exercise testing in Park City are described in Table 2. During treadmill climbing, Subject 1 was observed to externally rotate his right foot approximately 60° while planting and pushing off throughout the testing while his left foot remained straight.
Exercise parameter results for testing performed in Park City (PC) and Salt Lake City (SLC).
Peak values during Park City testing
VO2 = oxygen consumption; METS = metabolic equivalents; HR = heart rate; RER = respiratory exchange ratio; Vt = tidal volume; VE = ventilation.
Discussion
The Sherpas under study had physiological profiles similar to physically active, but not elite, individuals. Body composition was overall similar to healthy persons of similar age 19 and 6 elite Sherpas, 15 although our subjects had a higher body fat percentage than these elite Sherpas. Their exercise profiles were appropriate for testing conditions and reflected those of moderately fit individuals.
Exercise performance and body fat percentage are generally inversely related. 20 The 2 Sherpa subjects in this study did not exhibit particular leanness relative to other top climbing Sherpas.15,21 Body composition is not the only measure of fitness, and their body fat percentage does not seem to be a hindrance to their physical prowess.
Our subjects displayed no evidence of any persistent adverse effects on the heart as a result of chronic hypoxia or repetitive exposure to extreme elevation. Garrido 22 recorded an ECG in the Sherpa who held the record for the most Everest ascents prior to Subject 1 overtaking his record. This ECG did not show any signs of right ventricular hypertrophy, despite his repeated exposure to extreme altitude. Studies in Bhutanese and other Sherpas at altitude have described the lack of these ECG features as well. 23 Similarly, ECGs of the Sherpas in our study showed no persistent effects on the heart as a result of long-term altitude exposure. Many Andean natives, however, do in fact show effects of right ventricular hypertrophy. 24 The lack of these vigorous responses in Tibetans' pulmonary vasculature represents evidence of their superior genetic adaptation to high altitude.
Other studies of locomotion in high-altitude natives have shown interesting results. Six elite Sherpas in another exercise study 15 were all noted to have genu-valgum-recurvatum and flat foot that contributed to a peculiar running and walking style. Subject 1 in our study also has an atypical treadmill climbing style as described above. Sherpas may have adopted these styles to better balance and climb in the high mountain environment. Alternatively, the styles could represent their adaptation to the artificial testing conditions (and therefore contribute to a slightly lower exercise efficiency) compared to exercising in their natural environment.
Oxygen consumption and ventilation during 2 stages were slightly lower than expected (Subject 1, Step 3 and Subject 2, Step 2). This was possibly due to measurement error, for example, a small leak through the nose clip or mouthpiece. If these 2 steps are removed, the trend of the slope of the metabolic parameters is linear. Furthermore, the slopes of oxygen uptake and ventilation are parallel when comparing Salt Lake City to Park City testing; the absolute oxygen uptake and ventilation are higher in Park City for the same external work. From basic physiology, we know that the oxygen requirement should be the same for the same subject over different testing sessions for equal external work performed. The elevated responses at high altitude could be partially explained by the increased respiratory work at altitude in order to maintain the same alveolar pressure of oxygen versus the lower altitude.
Ge et al 25 demonstrated that Tibetans have lower minute ventilation than acclimatized lowlanders. Lower ventilation results in less dyspnea and more comfortable and efficient work at high altitudes. More efficient exercise capacity at high altitudes translates into superior carrying and climbing abilities on extreme altitude mountains. Sherpas' superiority during high-altitude exercise may not be apparent at low altitudes, but only realized when tested or performing at higher elevations. When descending to lower altitudes, high altitude natives do not experience a marked increase in VO2 max as one might expect.26,27 When ascending to higher altitudes, the aerobic capacity of Sherpas is far less penalized. 9 ,27-31 The Sherpas in our study had been living at 1325 m for a number of months and theoretically lost any temporary acclimatization to higher altitudes. Our Sherpa subjects would be expected to maintain their exercise performance to a far greater extent than matched lowlander counterparts when performing similar testing at higher altitudes.
Despite rigid theoretical speculation, oxygen consumption at sea level has not been shown to consistently predict performance at altitude. 14 Factors such as previous mountain experience and psychological drive may be more important than basic physiological parameters in high-altitude mountaineering. 32 The Sherpas' familiarity with negotiating mountainous terrain gives them a tremendous efficiency advantage while climbing. Overall work capacity is higher, 14 ,29,33 and aerobic metabolism is more efficient compared to acclimatized lowlanders. 34
The Sherpas had little experience with many of the testing modalities in this case study. The Sherpas had no experience with strength or exercise testing, and therefore some of these results may or may not reflect a true measure of their capabilities. We recorded VO2 peak (but not VO2 max) for our study conditions, making direct comparisons with other maximum values difficult. Our case study design did not allow comparison between controls and our Sherpa subjects. Further studies to elucidate these 2 and other Sherpas' physiology could include hypoxic ventilatory response, genotyping for polymorphisms that have been linked to performance at altitude, and controlled experiments matching these world-record-holder Sherpas to other Sherpa and lowlander groups.
Conclusions
The 2 world-record Sherpa climbers under study had anthropometric, blood values, pulmonary, and physiologic parameters similar to other Sherpas and the general population. Exercise response was appropriate to moderate and high altitude.
Footnotes
Acknowledgments
The authors thank the Sherpa subjects for their cooperation in these testing procedures. The authors also thank David Budge, PA-C for his assistance in obtaining the echocardiographic studies and Robert Schoene, MD for his helpful review of the manuscript.