
Abstract
Internationally, health systems face an increasing demand for services from people living with multimorbidity. Multimorbidity is often associated with high levels of treatment burden. Targeting lifestyle factors that impact across multiple conditions may promote quality of life and better health outcomes for people with multimorbidity. Motivational interviewing (MI) has been studied as one approach to supporting lifestyle behaviour change. A systematic review was conducted to assess the effectiveness of MI in healthcare settings and to consider its relevance for multimorbidity. Twelve meta-analyses pertinent to multimorbidity lifestyle factors were identified. As an intervention, MI has been found to have a small-to-medium statistically significant effect across a wide variety of single diseases and for a range of behavioural outcomes. This review highlights the need for specific research into the application of MI to determine if the benefits of MI seen with single diseases are also present in the context of multimorbidity.
Keywords
Introduction
Multimorbidity is defined as the diagnosis of more than one long-term condition in one person [1]. Epidemiological research has found high prevalence rates for multimorbidity [2–4]. This is particularly true in primary care, with studies in Scotland, Australia, and the USA identifying rates of 23.2% [2], 37.1% [3], and 45.2% [5], respectively. Compared with single diseases, multimorbidity is associated with a higher demand on health services, including more primary care contacts, prescriptions, and referrals for specialized care [6–8]. Demands on patients are also higher, due to burden of illness and treatment [9]. Lack of coordination of services [9–11], inattention to patient preference [7, 11], and the prevailing single-disease focus of clinical guidelines [2, 12, 13] all add to treatment burden. Applying single-disease guidelines to multimorbidity is costly, increases polypharmacy, and involves prescription of unrealistic daily self-care activities [13, 14]. Multimorbidity is a significant health issue and effective interventions are needed [13, 15–19].
Research on multimorbidity interventions is limited [8, 19, 20]. A 2013 Cochrane Collaboration review identified only 10 randomized control trials; two of which examined specific comorbidities [19]. Expert consensus recommendations emphasize supporting behaviour change to address lifestyle factors [19, 21–23]. In Canada, Fortin and colleagues examined the association between lifestyle factors and multimorbidity in 1,196 subjects and found that smoking, a diet lacking fruit and vegetables, lack of physical activity, alcohol consumption, and excess weight, are all factors associated with an increased likelihood of multimorbidity [24]. Furthermore, the likelihood of multimorbidity increased with each additional unhealthy lifestyle factor [24]. Medication adherence may also be important, given its impact on chronic condition management [25, 26]. The World Health Organization also promotes a greater focus on patient-centred skills, highlighting communication and support for behaviour change in chronic illness [23]. With its emphasis on the individual patient and focus on health-behaviour change, Fortin and colleagues suggest that motivational interviewing (MI) may be a useful intervention for the lifestyle factors impacting on multimorbidity [24].
MI has been formally defined as “…a collaborative, goal-oriented style of communication with particular attention to the language of change. It is designed to strengthen personal motivation for and commitment to a specific goal by eliciting and exploring the person's own reasons for change within an atmosphere of acceptance and compassion” [27]. MI is characterized by the use of communication skills, such as open questions, reflective listening to express empathy, and emphasis on patient autonomy in a clinical session [27]. First described by Miller in 1983 [28], the original application of MI was in treatment programmes for people with addictions, and subsequent studies demonstrated good clinical outcomes [29]. More recently, MI has been seen as a potentially effective intervention in physical healthcare settings [30]. This has been accompanied by an increase in the publication of primary research [31] and systematic reviews of MI [32–37]. MI has been found to have a small-to-medium effect across settings and a range of target behaviours [33, 37–40]. Lundahl and Burke [41] reviewed the findings of four meta-analyses in 2009, and found that MI was significantly more effective than no treatment, and equivalent to other treatments for a range of behaviour-change outcomes. Given the breadth of application of MI, and its patient-centred focus, further evaluation of its potential in multimorbidity care is warranted.
This systematic review identifies research papers of MI in healthcare where authors have used systematic review methodology to identify primary intervention trials and have also conducted a meta-analysis. This is the first systematic review of the literature to specifically examine meta-analyses. This systematic review has three objectives. Firstly, we will examine the evidence for MI in healthcare and specifically for multimorbidity, including the effectiveness of MI for addressing the lifestyle factors relevant to multimorbidity. Secondly, given the widespread impact of multimorbidity on the healthcare system and the recommendation to integrate multimorbidity intervention into existing healthcare [19], we will examine whether MI can be delivered effectively by a range of healthcare providers. Finally, based on this analysis of the reviews, we will consider and discuss the potential of MI in clinical work of patients with multimorbidity.
Methods
Our systematic review was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement [42, 43]. Review criteria were outlined a priori.
Inclusion criteria
Articles were included if the authors used systematic review methodology to identify relevant primary interventions, and also conducted a meta-analysis of the data from the identified primary interventions. Reviews were only included if participants were recruited from healthcare services, not criminal justice, education, or other sectors. We included reviews that identified studies of MI intervention, where authors of the reviews defined MI according to the general principles outlined by Miller and Rollnick [27], and used these principles in selecting the primary intervention papers. Included reviews were those that compared MI intervention with control, treatment as usual, or other intervention with behaviour change or standardized outcome measures.
Search strategy and article selection
The search included articles published up to and including January 2014. Due to practical constraints, selection was limited to English-language articles that were peer reviewed and published in full. The following electronic databases were searched: PsycInfo, Medline, CINAHL, EMBASE, and Cochrane library. In addition, we searched the online bibliography accompanying the 2013 Miller and Rollnick textbook [44]. Search terms were ‘motivational interview*’ AND [‘systematic review’ OR ‘meta-analysis’]. Terms included both subject index terms and free text. Duplicate articles were removed using the duplicate identification function in EndnoteX5 (Thomson Reuters, New York, Version X5 for Macintosh and Windows, 2011).
The search strategy and initial screening of article titles was performed by K.J.M.; articles clearly not meeting eligibility criteria were excluded. Abstracts were reviewed to determine whether a publication met the criteria for a systematic review or meta-analysis and if MI was an intervention included in the analysis. Full-text articles were reviewed to confirm eligibility. Uncertainty about inclusion of articles was resolved through discussion with the review team at regular meetings.
Assessment of quality of systematic reviews
All included articles were reviewed by K.J.M. using AMSTAR (A MeaSurement Tool to Assess systematic Reviews [45]). AMSTAR is a reliable 11-item tool for assessing the methodological quality of systematic reviews [46]. AMSTAR items include the design and conduct of the systematic review, the presentation of review data, the scientific quality of the methods for formulating conclusions, publication bias, and conflict of interest. A score of 1 is allocated to each item that fully meets the specified criteria for each of the 11 AMSTAR items. A score of 0 is allocated if the item is not met or if there is insufficient information presented in the review article to meet the criterion. The highest score possible using AMSTAR is 11, with the high scores being indicative of better methodology [46].
Data extraction
Effect size data were extracted for the overall efficacy of MI, as well as for alcohol, smoking cessation, diet and exercise, medication adherence, and weight interventions. Interpretation of effect sizes was guided by the benchmarks suggested by Cohen [47]. Information about the health conditions included in each review was extracted from summary tables and a review of the titles of trials included in each meta-analysis. Information about clinician type, MI training, and treatment integrity was also extracted. Data extraction was undertaken by K.J.M. with uncertainty resolved through discussion with the review team. Accuracy of data extraction was checked independently in regular formal meetings between K.J.M. and D.P., and K.J.M. and J.M.G.
Results
Selection of systematic reviews
The selection process is summarized in Figure 1. Twelve articles met the inclusion criteria.
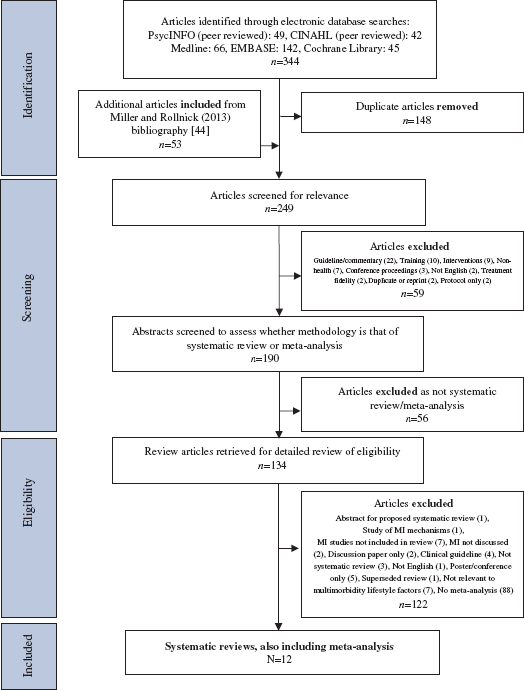
Flowchart of selection process for included articles using the following electronic databases: PsycINFO (database of abstracts produced by the American Psychological Association), CINAHL (Cumulative Index of Nursing and Allied Health Literature), Medline (Medical Literature Analysis and Retrieval System Online), EMBASE (Excerpta Medica dataBASE), Cochrane Library, and the bibliography by Miller and Rollnick [44].
Assessment of quality of systematic reviews
The included articles were assessed using AMSTAR (see Figure 2) [33, 34, 36, 37, 39, 40, 48–53]. The mean AMSTAR rating was 7.25 (SD=1.36). None of the 12 articles met the criteria for items 5 [Was a list of studies (included and excluded) provided?] and 11 (Was the conflict of interest stated?). In addition, the criteria were only met for 5 of 12 studies for item 2 (Was there duplicate study selection and data extraction?) and 6 of 12 studies for item 4 [Was the status of the publication (i.e. grey literature) used as an inclusion criterion?].

Rating for each of the identified systematic reviews that also included meta-analysis, using AMSTAR (A MeaSurement Tool to Assess systematic Reviews) [45].
Systematic review characteristics and effect sizes
The characteristics of the included systematic reviews are summarized in Table 1 [33, 34, 36, 37, 39, 40, 48–53].
Summary of characteristics of the included systematic reviews.

c/f, compared with; Tx, treatment.
Alcohol (15), diet and exercise (4), drug use (5), HIV-risk (2), eating disorder (1), smoking (2), treatment adherence (1).
Alcohol (29), blood pressure (1), diet (2), drug use (14), eating disorder (1), HIV-risk (5), gambling (1), medication adherence (1), public health intervention (1), smoking (6), treatment adherence (4), weight (1), not specified (1).
Alcohol (3), blood pressure (2), drug use (1), health promotion (3), smoking (2), not specified (1).
Alcohol (39), breastfeeding (1), dental health (1), diabetes management (1), diet (2), drug use (23), HIV-risk (4), gambling (2), health promotion (7), medication adherence (2), physical activity (3), public health intervention (1), smoking (17), treatment adherence (10), weight (1) not specified (3).
Alcohol (6), breastfeeding (1), dental health (2), diabetes management (4), diet (3), diet and exercise (1), drug use (3), Functional independence (2), eating disorder (1), HIV-risk (2), injury prevention (2), medication adherence (3), physical activity (1), quality of life (2), safe sex (1), self-management (3), smoking (8), treatment adherence (1), weight (2).
Alcohol (3), diet and exercise (1), drug use (2), medication adherence (1), smoking (2), smoking, diet, and exercise (1), treatment adherence (1), weight (1).
Table 2 summarizes the chronic conditions specified for participant groups in included systematic reviews [33, 34, 36, 37, 39, 40, 48–53]. Participant groups included people living with a range of conditions; however, no systematic review specifically examined multimorbidity.
Chronic conditions specified for participant groups in included motivational interviewing (MI) trials, determined by summary information and title search.
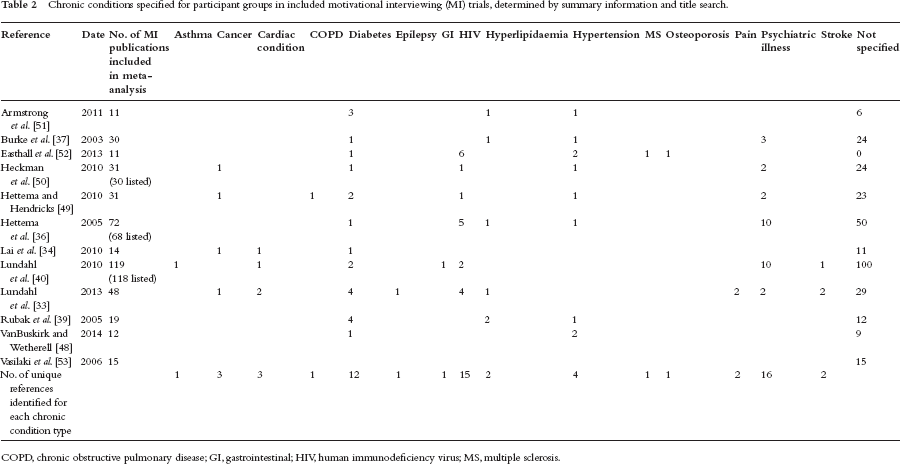
COPD, chronic obstructive pulmonary disease; GI, gastrointestinal; HIV, human immunodeficiency virus; MS, multiple sclerosis.
Table 3 summarizes the effect sizes, limitations, and conclusions for each systematic review [33, 34, 36, 37, 39, 40, 48–53]. Small-to-medium statistically significant effect sizes were reported for the overall effect of MI intervention across a range of health behaviours relevant to multimorbidity. Overall effect sizes ranged from d=0.18 [95% confidence interval (CI) 0.01, 0.37] [48] to d=0.77 (95% CI 0.35, 1.19) [36].
Summary of effect sizes, limitations, and conclusions for included meta-analyses.

[…]: 95% confidence intervals; –, no effect size provided; AC, attention control; AT, active treatment; BA, brief advice; BMI, body mass index; cigs, cigarettes; d, Cohen's d; g, Hedges’ g; I, information; IO, information only; k, no. of included trials; L, longterm follow-up;. MC, minimal contact; NP, non-pregnant sample; NT, no treatment; OR, odds ratio; RR, risk ratio; S, short-term follow-up; SC, standard care; TAG, traditional advice giving; VC, various comparison conditions; WL, waiting list.
Number of references included in this meta-analysis.
Number of references included in this meta-analysis and not in the other listed meta-analyses.
Data provided for 127 trials only.
Sample size data not provided.
Total number of references cited across meta-analyses, including those that were not unique to any one review.
Statistically significant.
Clinicians delivering MI interventions
Summary information about clinicians delivering MI interventions for each of the 12 meta-analyses is presented in Table 4 [33, 34, 36, 37, 39, 40, 48–53].
Summary of available data about clinician type and effect of clinician type in each systematic review.

HCP, healthcare providers; MI, motivational interviewing.
Treatment fidelity and MI training
Table 5 presents a summary of the minimal information available for MI training and treatment fidelity [33, 34, 36, 37, 39, 40, 48–53].
Summary of motivational interviewing training and treatment fidelity measures in each systematic review.

MISC, motivational interviewing skills code; a coding system for motivational interviewing, see Moyers et al. [54].
n/a, not available.
Discussion
Summary of main findings
We identified 12 systematic reviews that also included meta-analysis for MI in healthcare. We did not identify a study specifically examining MI as an intervention for multimorbidity. It appears that MI is as effective as other treatments for each of the lifestyle factors relevant to multimorbidity, and that it can be delivered by a range of healthcare providers. The extent to which these findings apply to the setting of multimorbidity has yet to be determined.
Strengths and limitations
Overall, the included systematic reviews were of a good quality. Similar to other studies [55, 56], some items on the AMSTAR tool were not met by any publication. Items requiring more extensive statements may be affected by publication parameters. This review has synthesized significant amounts of information, and the quality of the reviews supports the conclusions drawn.
This review is limited by the fact that included reviews evaluate the effectiveness of MI for single diseases. We have examined the evidence for the lifestyle factors relevant to multimorbidity, in the absence of specific multimorbidity studies. We are therefore inferring from the available evidence about the potential of MI for multimorbidity; in particular, its potential to address lifestyle factors impacting on the health of patients with multimorbidity.
Additionally, a potential limitation of this review is that selection was limited to English-language publications. In this case, publication bias may be ameliorated by statistical assessment of publication bias in 75% of the included systematic reviews, and searching of grey literature in 50%. There was also a lack of information about cost-effectiveness. The systematic review by Lai and colleagues identified two trials that reported information about cost, but the information was insufficient to draw any conclusions [34]. While some authors of the included systematic reviews suggested that MI may be more cost-effective than other interventions as it is a briefer intervention [40, 50, 53], the need for specific cost–effectiveness analyses was identified as an important consideration in future research [37, 40, 53].
Relating the findings to the existing literature
The lack of evidence for the application of MI to multimorbidity intervention is not an unexpected finding. The Cochrane Review undertaken by Smith and colleagues [19] only identified 10 randomized controlled trials of intervention for multimorbidity and none of these included MI. Despite the lack of intervention trials, expert consensus recommendations identify patient-centred care and communication skills, promoting healthy behaviours, and integrating intervention into routine healthcare as core elements for multimorbidity intervention [4, 12, 19, 23, 24]. Indeed, some of the authors of the included reviews propose implementing MI as an intervention in routine healthcare [33, 36, 39, 40, 48, 52] and for the multiple behaviour-change challenges inherent in primary care practice [48].
Implications for research and clinical practice
MI is a well-articulated and learnable skill [57–59] and appears to be a useful intervention for a range of health-behaviour-change targets, such as diet and exercise, weight management, smoking cessation, medication adherence, and alcohol consumption. All of these behaviours are relevant to people living with multimorbidity.
Further research may benefit from a greater focus on clinician proficiency, and a greater emphasis on the effectiveness of MI when delivered by a range of clinicians. Future research also needs to include treatment fidelity measures [37] to ensure the intervention being studied is indeed MI. In addition, it may also be helpful to use treatment fidelity measures with treatment as usual or comparison conditions to evaluate the degree to which MI can be differentiated from baseline communication styles in routine healthcare delivery [60].
Conclusion
Multimorbidity presents significant challenges to the people who are living with multiple conditions and healthcare professionals alike. MI appears to be a helpful approach to healthcare across a range of single diseases, and for health-behaviour change. Based on the existing recommendations for multimorbidity interventions and the findings of this review, it appears that research that directly examines the application of MI for working with people with multimorbidity is warranted.
Footnotes
K.J.M. is a member of the Motivational Interviewing Network of Trainers. There are no other conflicts of interest to declare.
Ballarat Health Services provided in-kind support for this research.