
Abstract
Multimorbidity, the presence of 1+ chronic condition in an individual, remains one of the greatest challenges to health on a global scale. Although the prevalence of multimorbidity has been well-established, its incidence is not fully understood. This systematic review determined the incidence of multimorbidity across the lifespan; the order in which chronic conditions accumulate to result in multimorbidity; and cataloged methods used to determine and report accumulation of chronic conditions resulting in multimorbidity. Studies were identified by searching MEDLINE, Embase, CINAHL, and Cochrane electronic databases. Two independent reviewers evaluated studies for inclusion and performed quality assessments. Of 36 included studies, there was high heterogeneity in study design and operational definitions of multimorbidity. Studies reporting incidence (n = 32) reported a median incidence rate of 30.7 per 1,000 person-years (IQR 39.5 per 1,000 person-years) and a median cumulative incidence of 2.8% (IQR 28.7%). Incidence was notably higher for persons with older age and 1+ chronic conditions at baseline. Studies reporting patterns in accumulation of chronic conditions (n = 5) reported hypertensive and heart diseases, and diabetes, as among the common starting conditions resulting in later multimorbidity. Methods used to discern patterns were highly heterogenous, ranging from the use of latent growth trajectories to divisive cluster analyses, and presentation using alluvial plots to cluster trajectories. Studies reporting the incidence of multimorbidity and patterns in accumulation of chronic conditions vary greatly in study designs and definitions used. To allow for more accurate estimations and comparison, studies must be transparent and consistent in operational definitions of multimorbidity applied.
Introduction
Multimorbidity continues to increase world-wide, presenting one of today’s biggest challenges to individual and population health, and to health systems.1,2 Multimorbidity results in poorer patient outcomes3,4 and excess mortality.5–20 Patients with multimorbidity also present with unique medical care needs; while specialized treatment approaches are appropriate for single diseases, patients with multimorbidity require complex and structured care plans. 21 This poses substantial impacts on disease management, healthcare utilization, and costs.22–24 The study of multimorbidity, and its epidemiology, may help in better understanding its development; determine reasons for variations in patient outcomes; and design targeted interventions to manage adverse outcomes of multimorbidity.25–27
Existing literature on the epidemiology of multimorbidity has increased substantially, moving from a nascent body of evidence in the 1970s to a now well-established and distinct field of research. Consistent with a growing area of study, the epidemiological research was concerned first with defining multimorbidity and summarizing studies concerning its prevalence.26,28 Determining prevalence has permitted us to quantify the burden of multimorbidity in populations and health care systems. However, prevalence is limited in its ability to tell us when and why people accumulate multimorbidity. In order to better understand the etiology of multimorbidity and to project the healthcare needs of patients with multimorbidity, we must turn our attention to determining its incidence.
The incidence of multimorbidity is, by definition, the incidence of multiple chronic conditions that are accumulated in a particular order. Therefore, it is important to study both the incidence of multimorbidity and the accumulation of its component chronic conditions. Currently, there is a growing body of research addressing incidence of multimorbidity. As well, there is emerging literature using innovative and heterogenous methods to describe the accumulation of chronic conditions in multimorbidity. Our goal was to summarize available evidence on the incidence of multimorbidity across the lifespan. More specifically, our objectives were: 1. to determine the incidence of multimorbidity overall and by age groups, including children; 2. to determine the order in which people accumulate the component chronic conditions leading to multimorbidity; and 3. to catalog the methods used to assess and report accumulation.
Methods
We conducted a systematic review (registered in PROSPERO, reference no. CRD42020191876) in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and checklist (Supplementary Table S1). 29 An a priori review process was established and followed; this protocol was not published. As this was a systematic review of literature, Research Ethics Board review or approval was not required. There were no participants or patients enrolled and so no consent was needed for participation, or for patient information and images to be published.
Literature search strategy
Following the recommendation from Chapter 4: Searching for and Selecting Studies in the Cochrane Handbook for Systematic Reviews of Interventions, 30 searches of the health-related bibliographic databases, MEDLINE, Embase, CINAHL, and The Cochrane Library were undertaken by the Health & Medicine Librarian (MS1), utilizing both free-text and subject headings (MeSH) to identify an initial batch of relevant and eligible studies reporting incidence of multimorbidity and/or patterns in accumulation of chronic conditions. Databases were searched from inception to May 26, 2020.
Search terms used in the database query for multimorbidity, with its various spelling, were “multimorbidity,” “multi-morbidity,” “multimorbidities,” “multi-morbidities,” “multiple morbidities,” “multiple-morbidities,” “multiple chronic diseases” and “multiple chronic conditions.” We searched for incidence and accumulation and their different meanings, using “inciden*,” “accumulat*,” “trajector*,” “longitudinal,” “acquire,” “acquisition,” “predict*,” “cohort,” and “epidemiology.” The full search strategy is provided in Supplementary Table S2.
Study selection
After removing duplicates, titles and abstracts of initial search results were screened by the two reviewers (PK, BS) independently for eligibility. Reviewers initially screened two sets of 10 articles and discussed decisions with the senior study coordinator (BLR) to ensure consistency in applying selection criteria. Eligible articles included peer-reviewed studies using primary or secondary quantitative analyses, including mixed methods studies, published in English and/or French language. Studies with participants of all ages, including children, and specifically reporting 1. incidence of multimorbidity and/or 2. patterns in accumulation of chronic conditions as primary or secondary outcomes, were included. Conference presentations, books, letters, editorials, non-human literatures, and abstract-only studies were excluded. Articles deemed suitable for full-text review were identified and full-texts were then reviewed to confirm eligibility criteria by the two reviewers first independently and then collaboratively to reach consensus. Studies which still satisfied inclusion and exclusion criteria upon full-text review were selected for data extraction. Disagreements were initially discussed by reviewers for resolution. The study coordinator worked with reviewers to resolve any disagreement through consensus. Within the articles identified for review, reference lists were hand-searched for additional articles meeting our criteria.
Quality assessment
The two reviewers independently performed quality assessment using the Newcastle-Ottawa Scale (NOS) for assessing study methodology of non-randomized studies. 31 NOS assessment guidelines were followed and, where dictated by NOS guidelines, some assessment criteria were further defined by study authors as described in Supplementary Table S3. Randomized controlled trials (RCTs) were assessed for study methodology and risk of bias (RoB) using the Cochrane Collaboration’s RoB tool. 32 Of the 36 included studies, 35 observational studies and one RCT underwent quality and risk of bias assessment (Supplementary Table S4). Individual NOS ratings were converted to Agency for Healthcare Research and Quality (AHRQ) standards as one of three levels: Good, Fair, and Poor. A priori scores to exclude studies of low quality were not established in order to include the entire landscape of literature in this review; as such, studies of all scores were included.
Data extraction
The two reviewers independently extracted data from eligible studies following full-text review. A comprehensive data extraction sheet was developed to collect data pertaining to: study characteristics (authors, date of publication, study design, geographic locations, data collection period, follow-up period, data sources, sample size, populations of interest); sample demographics (ages, sex and/or gender, race and/or ethnicity, body mass index (BMI), education levels, smoking status, alcohol consumption levels, physical activity levels, and marital statuses); definitions of multimorbidity; number and selection of conditions included in definitions of multimorbidity; incidence rates and/or cumulative incidences of multimorbidity; patterns in accumulation of chronic conditions; methods used in accumulation studies; and risk factors for multimorbidity. The sheet was pilot tested using three studies. The two reviewers then reconciled any differences, consulting the senior study coordinator as required. Study authors were contacted by email for further information as needed for clarification.
Incidence data were recorded in separate tables for studies reporting incidence rates (IRs) and for studies reporting cumulative incidence. IRs were extracted as the number of incident cases per 1,000 person-years. Results from studies not already reporting per 1,000 person-years were adjusted to meet this format. Cumulative incidence was extracted as a percentage. Results from studies not providing percentages were standardized to meet this format by dividing the incident cases by the number of baseline participants without multimorbidity and multiplying by 100. When multiple IRs were reported, overall IRs across the population were reported in tables if available; additional IRs were not reported; however, in the tables, the availability of additional IRs is noted. If overall IR or cumulative incidence was not available, incidences provided by study authors were presented in the following priority, as available: by age, sex and/or gender, other demographics.
Results
Overview of studies
The process used for study selection is reported in the PRISMA flow diagram (Figure 1) and PRISMA checklist 33 (Supplementary Table S1). We identified 4,579 studies from the initial database searches; all were published between 1976 and 2020. After removing duplicates and non-original articles, 2,926 studies were identified, of which 109 were retained for full-text screening. A total of 73 articles were excluded following full-text review or qualitative synthesis,34–106 with reasons; the majority of excluded studies were those that did not report incidence of multimorbidity; reported incidence of specific chronic conditions and not of multimorbidity; and/or did not account for temporal components when determining patterns in accumulation of chronic conditions, amongst other reasons. Of the articles that underwent full-text review, 36 studies were included in further synthesis. No additional articles meeting our inclusion criteria were identified during hand-searches of study reference lists.

PRISMA flow diagram for study selection.
Study quality and characteristics
Of the 35 observational studies, most studies (n = 26) were rated as Good quality according to AHRQ standards. Nine studies were ranked as Poor quality due to their omission of information regarding: representativeness of their data, ascertainment of exposure, controlled factors, assessment of outcome, adequacy of follow-up duration, case definition(s), case representativeness, selection strategy(ies), and/or non-response rate(s).107–115 RoB assessment for the one RCT 116 yielded low risk (Supplementary Table S5).
Of the 36 included studies, one examined both incidence and accumulation 117 ; 31 studies reported only the incidence; and four studies reported only the accumulation of chronic conditions resulting in multimorbidity. Multimorbidity was defined as the presence of 2+ chronic conditions in all but six studies. Of these six, one study 107 defined multimorbidity as the co-occurrence of 3+ conditions and four111,116,118,119 did not specify a definition (Supplementary Table S6). However, all authors referenced consideration of 2+ conditions in their prose and/or tables. The number of chronic conditions used to identify multimorbidity varied extensively, ranging between 3 and 506. At the extremes, in one study of accumulation, 117 three conditions were included (cancer, diabetes, and cardiovascular diseases); whereas, in another, 118 132 clusters of chronic conditions were included.
Table 1 reports the characteristics of the 32 studies that reported incidence of multimorbidity: 14 reported IR and 18 reported cumulative incidence. Studies were heterogeneous across all descriptive variables, including geographical location of study, data collection and follow-up periods, data sources, sample size and population, and demographics. The majority of studies reported either national or local incidence in high income (HIC) (n = 30) or middle income countries108,120 (MIC) (n = 2). The majority of studies sourced data from a combination of sources,108,109,112–114,117,119–128 and sampled general populations,109,110,112–117,120,122,124,126,128–135 with the remainder focused on specific patient populations.25,107,108,119–121,136–138 Samples were generally larger for studies examining general populations. All except two115,130 studies included different age groups across the lifespan. The majority of studies did not report race and/or ethnicity (n = 16/36), and, of those that did, there was heterogeneity in the terminology used to describe race and/or ethnicities.
Baseline characteristics for studies reporting incidence of multimorbidity (n = 32).

ANM, age at natural menopause; ART, antiretroviral therapy; HIV, human immunodeficiency virus; IR, incidence rate.
a As provided by study authors as either mean or median years, or person-years. Group-specific mean (or median) follow-up periods are included for studies which did not report an overall mean or median follow-up period.
b Without multimorbidity at baseline, as defined by study author(s).
c Age at baseline; reported as range or mean or median if an exact range was not reported.
d Ethnicity is reported using terminology directly reported by study authors. Elaboration of ethnicities included in groups is provided where reported.
e This age refers to the age of participants at baseline among all study participants irrespective of multimorbidity status as the age specific to participants without multimorbidity at baseline was not provided by authors.
f This proportion of females refers to the proportion at baseline among all study participants irrespective of multimorbidity status as the proportion of females specific to participants without multimorbidity at baseline was not provided by authors.
Table 2 reports characteristics of the five studies reporting patterns in accumulation of chronic conditions resulting in multimorbidity. Similar to studies reporting incidence of multimorbidity, accumulation studies were heterogeneous across all descriptive variables, including geographical location of study; data collection and follow-up period; sample population and size; and demographics. The majority of studies reported either national or local patterns in accumulation of chronic conditions in HICs.25,107,111,118 Most accumulation studies sampled general populations and sample sizes ranged from 9,160 and approximately 5 million. Comparable to studies reporting incidence of multimorbidity, study population ages ranged across the lifespan with most studying older adults only. One study reported race and ethnicity, 107 and data were most commonly sourced from medical records.
Baseline characteristics of studies and participants reporting accumulation of chronic conditions (n = 5).
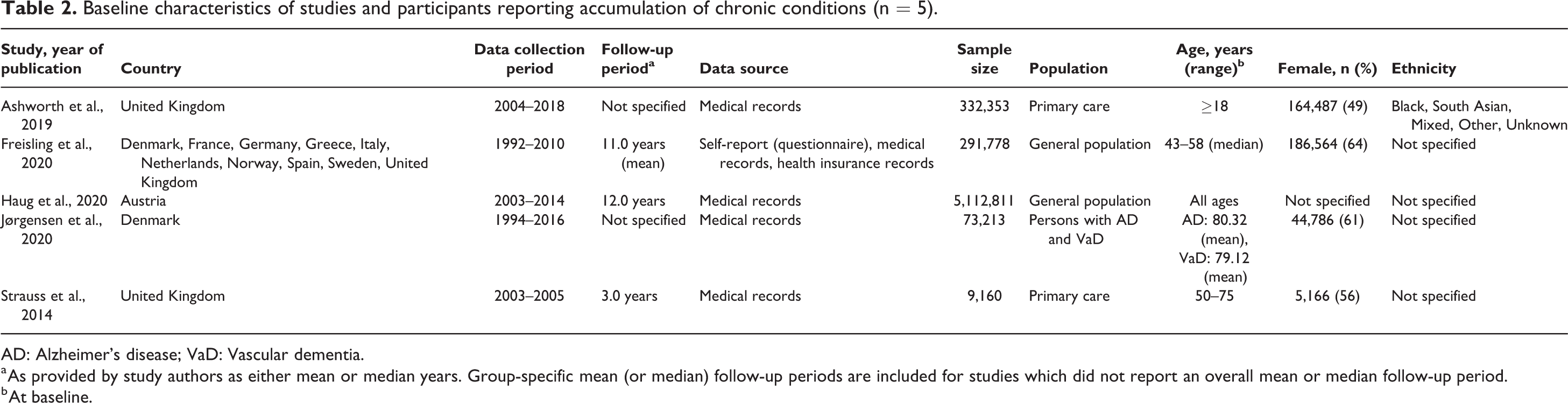
AD: Alzheimer’s disease; VaD: Vascular dementia.
a As provided by study authors as either mean or median years. Group-specific mean (or median) follow-up periods are included for studies which did not report an overall mean or median follow-up period.
b At baseline.
Incidence of multimorbidity
The incidence of multimorbidity for the 32 incidence studies are reported in Table 3 .
Incidence of multimorbidity by study (n = 32).

ANM, age at natural menopause; BMI, body mass index; CVD, cardiovascular disease; DEP, depression; DM, diabetes mellitus; HIV, human immunodeficiency virus; T2D, type II diabetes.
a Additional incidence rate(s) and/or cumulative incidence available in study text.
Among the 14 studies reporting IRs, rates were highly heterogeneous. Only five of the 14 studies reported an overall IR in addition to group-specific rates.109,121,123,126,132 Across studies reporting incidence, the median (unadjusted) incidence rate was 30.7 per 1,000 person-years (IQR 39.5 per 1,000 person-years) and the median (unadjusted) cumulative incidence was 2.8% (IQR 28.7%). Incidence rates ranged from 1.26 to 342 per 1,000 person-years. Of all incidence studies, two adjusted incidence for age, sex, and/or ethnicity.129,130 IRs across the lifespan increased with age, with studies of middle-aged to older participants (50+ years of age) reporting higher IRs than those consisting of younger and adult populations (0–40 years of age). Most studies did not stratify IRs by sex, with only one reporting IRs among male and female participants separately 130 ; this study reported a higher IR among women than in men. Of the 11 studies reporting race and/or ethnicity, five reported incidence rate(s) stratified by race and/or ethnicity,109,112,123,129,132 one adjusted incidence rates for race and/or ethnicity, 136 and two presented both adjusted overall and stratified incidence rate(s) by race and/or ethnicity.129,130 Two studies consisting solely of South and East Asian ethnicities (Malay, Chinese, and Indian)110,112 reported higher IRs than the remaining studies reporting IRs in White, Non-White, Black/African-American, Hispanic, and Māori populations.
Cumulative incidences of multimorbidity are presented in Table 3. Of the 18 studies reporting cumulative incidence, 10 studies reported overall unadjusted cumulative incidence ranging from 1.3% to 61.0%. Group-specific values ranged between 0% of participants developing multimorbidity (expressed in a European study as development of four chronic conditions over 2-year follow-up) 116 and 76.8% of participants developing multimorbidity (defined in an Australian study of women as development of two or more chronic conditions over 20-year follow-up). 139 Amongst five studies of specific patient populations, three had higher cumulative incidence108,137,138 compared to those conducted in general populations.
Across studies reporting either incidence rate or cumulative incidence, studies of older (45+ years of age) populations reported higher cumulative incidence than those which included younger population (<21 years of age).119,133 Additionally, in studies which presented incidence stratified by baseline disease counts, persons with one chronic condition at baseline had higher incidence of multimorbidity by the end of study follow-up, compared to those with zero at baseline.110,113,116,128,134,137,139 With the exception of one, 112 studies including nine or more chronic conditions in their definition of multimorbidity reported higher incidence than those including fewer conditions.
Patterns in accumulation of chronic conditions
The five articles that studied the accumulation of chronic conditions varied in the methods used to determine patterns, format of reporting, and in the component chronic conditions making up multimorbidity (Table 4). Four studies reported overall pattern(s) in accumulation25,107,111,118 and, of these, only one reported additional patterns by demographic subgroups 107 and one reported patterns in accumulation by starting condition among participants. 117 Three studies characterized the order of component chronic conditions as trajectories,25,111,118 one as transitions, 117 and one as pathways. 107 All but two studies25,107 reported patterns in accumulation of chronic conditions in populations of individuals with specific underlying diseases.
Patterns in accumulation of component chronic conditions in multimorbidity and methods used to ascertain patterns (n = 5).
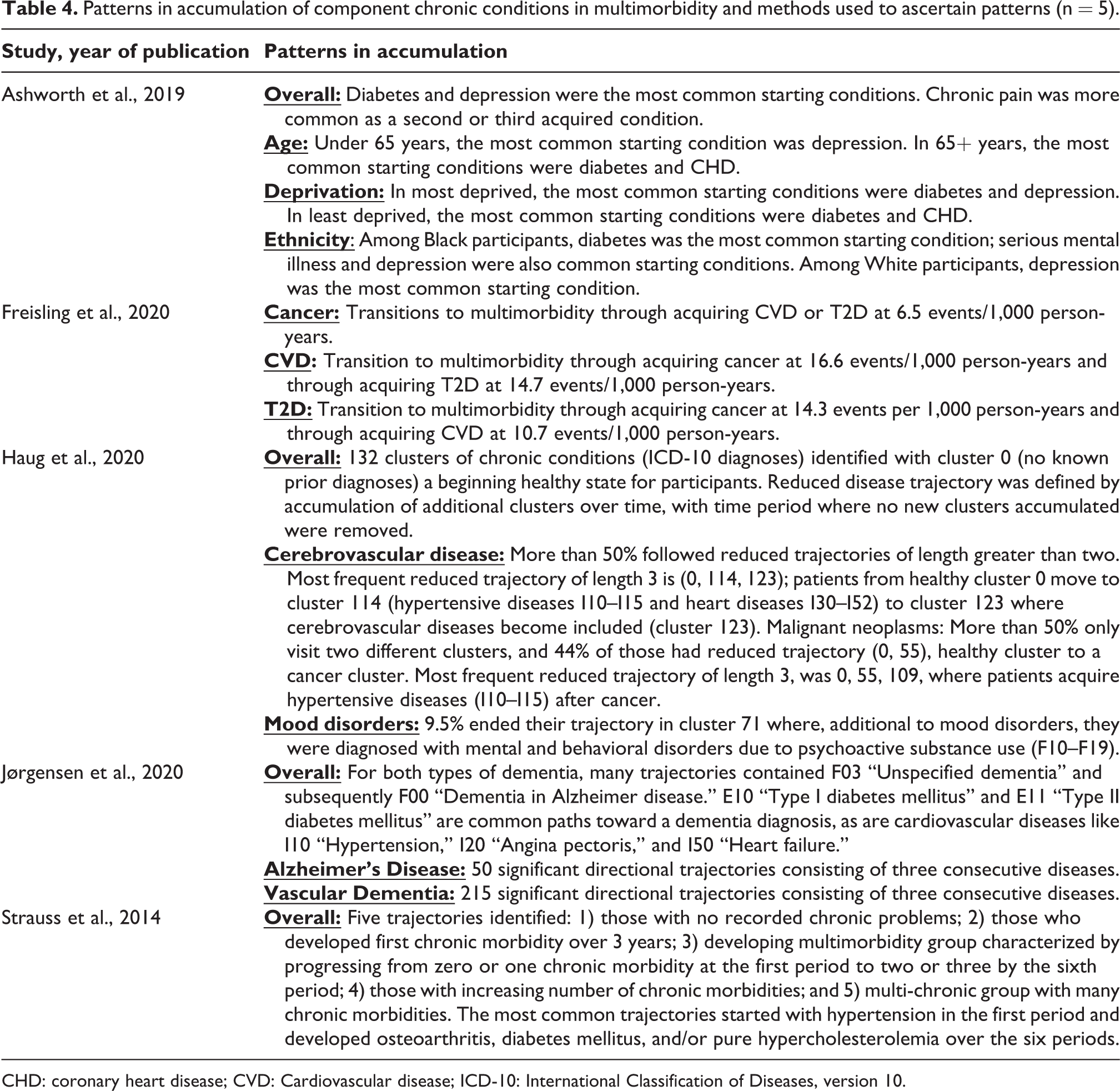
CHD: coronary heart disease; CVD: Cardiovascular disease; ICD-10: International Classification of Diseases, version 10.
As reported by Ashworth et al., 107 starting conditions varied by age, social deprivation, and ethnicity. For example, depression was more common as a starting condition in individuals under 65 years of age, while diabetes and CHD were more common in those 65+ years of age. 107 Four studies reported hypertensive and heart diseases as among the common starting conditions resulting in later multimorbidity25,111,117,118 and two reported diabetes as the most common starting condition.107,111 Second and third conditions contributing to multimorbidity were highly variable amongst reported patterns; two studies indicated cerebrovascular diseases and mental health illness (i.e. mood disorders) as common second conditions resulting in multimorbidity status.111,118 This is in contrast to one study reporting a mental health illness (depression) as a common overall starting condition. 107 Additional second- and third-component conditions reported include chronic pain, osteoarthritis, cancer, diabetes, and hypercholesterolemia.25,107,117
Methods in determining patterns in accumulation of chronic conditions
There were diverse methods used by the five studies to determine and report the accumulation of component chronic conditions leading to multimorbidity; despite this diversity, each study reported their results diagrammatically.
Ashworth et al. 107 employed alluvial plots, 140 whereby the chronic conditions in the accumulation sequence are assigned to vertical axes. Bar heights of the vertical axes were used to represent the number of persons with a particular chronic condition, and the widths of “streams” joining bars were used to represent the number of persons in each adjoining pair of chronic conditions. Freisling et al. 117 identified chronic conditions and calculated hazard ratios for movement from one starting condition to another, reported as the number of cases per 1,000 person-years. Separate pathway diagrams representing acquisition sequencing of three conditions were presented.
Haug et al. 118 employed machine learning to develop trajectories for risk of cardiovascular mortality based on divisive cluster analysis, in which all persons started in the same cluster and were algorithmically divided into different clusters according to the chronic conditions acquired over time. The study presented cluster trajectories as a multilayer network diagram.
Jørgensen et al. 111 examined pre-dementia temporal accumulation of multimorbidity for persons with Alzheimer’s disease and vascular dementia. Disease pairs were examined to determine which condition came first. The relative risk for acquiring the second condition for those with dementia compared to matched controls, was calculated. In addition to relative risks, the study presented temporal disease trajectory networks of diagnoses for persons with dementia, where each condition is a node joined by lines that indicate accumulation pathways.
Strauss et al. 25 conducted a latent class growth analysis to identify distinct multimorbidity trajectories. The analysis began with a one-cluster model (all persons having the same trajectory). The number of clusters was increased until most heterogeneity was explained. Quadratic growth curves were applied, and persons were assigned to a cluster in which their posterior probability of membership was highest. The trajectories of numbers of accumulating conditions were presented graphically using latent class growth trajectories.
Discussion
This systematic review contributes to a growing body of literature concerning the epidemiology of multimorbidity by providing a comprehensive, qualitative analysis of multimorbidity incidence and patterns in the accumulation of chronic conditions. The purpose of most included studies was to determine the incidence of multimorbidity and/or accumulation of component chronic conditions leading to multimorbidity. However, nine studies had other primary objectives and were able to opportunistically examine incidence.111,112,116,119,122,123,134,136,141
Of the 32 studies reporting incidence, five studies reported overall IRs ranging from 1.26 to 68.5 per 1,000 person-years, and 10 studies reported overall cumulative incidence ranging from 1.3% to 61.0%. The wide variation among incidence estimates in these 15 studies may be attributed to differences in: study populations being examined, with some sampling general populations and others sampling patient populations with specific baseline conditions; age and race or ethnicities of study participants; follow-up duration; as well as a lack of uniformity in the criteria that were used to define multimorbidity. The remaining 17 incidence studies reported incidence stratified by sociodemographic and medical factors. This helps elucidate factors impacting multimorbidity; however, it would facilitate comparisons across studies if authors report, where possible, overall rates adjusted for factors known to be associated with multimorbidity, including (at minimum) age, sex/gender, and number of baseline conditions.58,142 Only two studies in this review adjusted overall incidence for age and sex.129,130
The findings from this review regarding the relationship between multimorbidity and the number of baseline chronic condition(s), age, and sex generally aligned with previous literature. In studies which presented incidence stratified by baseline disease counts, persons with one chronic condition at baseline had higher incidence of multimorbidity later in life, compared to those with zero at baseline. This may be due in part to underlying genetic mechanisms of chronic diseases 143 ; systemic health impacts of chronic conditions in diagnosed individuals 144 ; and/or persons with a baseline chronic condition being more likely to seek medical help, 145 and therefore more likely to be diagnosed with other illnesses unrelated to the initial illness. Both incidence rates and cumulative incidence were higher in older populations, consistent with the well-documented relationship between age and multimorbidity.146–148 Amongst studies reporting incidence by sex, IRs and cumulative incidence were higher for women than men. This relationship between sex and multimorbidity is consistent with literature indicating that women may be more likely to be diagnosed with chronic conditions because they are more likely to seek medical help149–152 and have higher life expectancies than men.142,153,154
Of all identified studies reporting patterns in the accumulation of multimorbidity’s component chronic conditions, only five studies met our selection criteria. This review indicates distinct patterns in accumulation of chronic conditions, as reported by studies elucidating cardiovascular and metabolic conditions amongst the most common starting conditions, and cerebrovascular and mental illnesses as common second conditions resulting in multimorbidity. Together, cardiometabolic conditions including stroke, heart disease, and diabetes, contribute to leading causes of morbidity, mortality, lower quality of life, and health resource use globally.117,155–157 Understanding disease trajectories as discussed in this review may help clinicians identify persons at greater risk of developing such conditions and better understand their prognosis in order to effectively prevent and manage this set of diseases. Depression was noted as a common starting condition in persons below 65 years of age, which may be attributed in part to cultural trends in digital and communication media, sleep deprivation, and social deprivation in younger persons, contributing to rising rates of mood disorders and suicidal thoughts and behaviors since the mid-2000s, factors which may have a greater impact on younger persons compared to older generations.107,158 This result was found only in one study in accumulation, demonstrating the need for future research to confirm these findings in other populations. There is significant diversity in the definition of “patterns” in multimorbidity research, with some studies employing a temporal component25,107,111,117,118 and others using the term almost synonymously with patient clusters. 63 Methods used to discern accumulation were highly heterogeneous and showed novel applications of advanced statistical techniques. A common feature of the five articles was the use of diagrams to demonstrate temporal relationships. Ongoing innovation in this area bodes well for future research that examines the accumulation of component chronic conditions in multimorbidity and may inform preventative efforts.
We identified articles that used the term accumulation differently than we had initially set out in our objectives, which was to examine the order of chronic condition accumulation leading to an individual having multimorbidity. As such, we excluded studies that measured speed of accumulation of chronic conditions 46 and those that measured accumulation as most commonly occurring incident dyads and triads of chronic conditions without consideration for order or disease onset. 130 However, this diversity in the definition of accumulation can add to the richness of understanding multimorbidity incidence, and therefore an in-depth examination taking into account all aspects and forms of accumulation reported across the literature is warranted.
Our review found limitations in the included studies with respect to age, sex and gender, and race and ethnicity. The study of multimorbidity is heavily focused toward adult and elderly populations159–161; however, incidence of multimorbidity amongst children and adolescents who have chronic conditions warrants more attention given their increased risk of developing additional diseases later in life.162,163 Additionally, most studies reported patterns by chronic conditions and only one reported patterns by demographic factors, such as age.
All studies in our review were not explicit in their definitions of sex and gender. Such studies are failing to define sex and gender as non-binary variables when studying the health of populations.164,165 Among studies that reported race and/or ethnicity, data were collected from different sources ranging from medical records to self-report. The COVID-19 pandemic underscored the importance of calculating race and ethnic-specific incidence of multimorbidity.166,167 Routine collection of these data is a necessary step to understanding the role of race and/or ethnicity in multimorbidity incidence.
The findings from our systematic review demonstrate heterogeneity across studies with respect to incidence of multimorbidity and with respect to the order in which component chronic conditions that lead to multimorbidity were accumulated. This is consistent with reviews reporting the prevalence of multimorbidity26,28 for similar reasons as have been found in these prevalence studies. The heterogeneity across articles may be due in part to diverse study objectives, study designs, and operational definitions for multimorbidity across the included studies. More specifically, the widely varying number and selection of chronic conditions contributing to the definition of multimorbidity poses significant challenges to the comparison of findings among studies. For example, there is well-established evidence that hypertension is a precursor to multimorbidity in adult populations168,169; however, some studies did not include hypertension in their definition of multimorbidity. This finding may be the result of specific studies’ consideration of hypertension as a risk factor and not as a disease. 170
While study specificity in design or operational definition of multimorbidity may allow for more targeted study of multimorbidity within a given population, it contributes to the complexity of comparing incidence and accumulation of multimorbidity across studies. Given the heterogeneity among incidence studies, authors should be transparent in reporting results. At minimum, authors should explicitly state their definition of multimorbidity, clearly indicating the number of co-occurring conditions required to define multimorbidity, and the number and selection of chronic conditions included in their list of component chronic conditions. Additionally, where the available data permit, studies are encouraged to limit defining conditions of multimorbidity to five relevant chronic conditions, including those with well-established links to increased risk of multimorbidity development, including cardiovascular diseases,171,172 hypertension,168,170 and diabetes.173,174
This systematic review studied the incidence of multimorbidity and patterns in accumulation of chronic conditions across the lifespan, including children. Our consideration of all age groups is a strength of this review in light of evidence demonstrating the onset of a number of morbidities at younger ages; possibilities for illnesses to transition to chronic status; and the value of early identification in timely intervention and mitigating disease progression. 127 In addition, incidence rates were stratified by reporting format (IR or cumulative incidence) for more accurate comparison among study findings. This review was conducted in accordance with PROSPERO guidelines by two reviewers, with title and abstract screening, full-text review, data extraction, and quality assessment of studies completed independently. Included studies were mostly of high quality in accordance with the NOS, AHRQ, and Cochrane RoB criteria.
An inherent limitation amongst all systematic reviews is the omission of potentially relevant articles. Due to our inclusion criteria requiring articles to be of either English or French language, 122 non-English/French studies were excluded early in the review process without consideration for inclusion, some of which may have been relevant to our study. In addition, studies of low quality in reporting were not excluded to ensure the full spectrum of literature in multimorbidity was included in this review. This may have impacted the accuracy of these studies’ estimates. For example, studies which scored low on representativeness may produce estimates that do not represent the true estimates for their target population; however, it is not possible to discern whether such estimates are inflated or deflated. Similarly, studies which scored low on reporting outcome assessment may have estimates lower than actual because they did not adequately capture every occurrence of multimorbidity. Finally, while studies in this review reported on chronic conditions or non-communicable diseases, three studies also included a small count of acute conditions in their definitions and four did not specify a definition of multimorbidity (Supplementary Table S6). Despite the lack of explicit definition of multimorbidity in these studies, we were confident in including their work given reference to 2+ conditions in prose and/or tables.
Conclusion
Establishing the incidence of multimorbidity is a critical step in understanding the etiology and informing prevention of multimorbidity in general and specific patient populations across the lifespan. This systematic review of 36 studies presents that nearly 31 per 1,000 person-years (IQR 39.5 per 1,000 person-years) and 3% (IQR 28.7%) of the studied populations included in this review are affected by multimorbidity, and that component chronic conditions contributing to the development of multimorbidity are highly heterogenous. We recommend that researchers be transparent in reporting the components of their operational definitions of multimorbidity, and that patterns in multimorbidity be differentiated by age group and sex and/or gender to allow more specific analyses of the incidence of multimorbidity, and its implication for health care and health systems. Our findings support the importance of work underway to determine a standardized operational definition of multimorbidity. 175 These practices will allow for more accurate comparison and estimation of the incidence and progression of multimorbidity, and subsequently, more effective disease management and preventative interventions across all stages of life.
Supplemental material
Supplemental Material, sj-docx-1-cob-10.1177_26335565211032880 - The incidence of multimorbidity and patterns in accumulation of chronic conditions: A systematic review
Supplemental Material, sj-docx-1-cob-10.1177_26335565211032880 for The incidence of multimorbidity and patterns in accumulation of chronic conditions: A systematic review by Prtha Kudesia, Banafsheh Salimarouny, Meagan Stanley, Martin Fortin, Moira Stewart, Amanda Terry and Bridget L Ryan in Journal of Comorbidity
Supplemental material
Supplemental Material, sj-docx-2-cob-10.1177_26335565211032880 - The incidence of multimorbidity and patterns in accumulation of chronic conditions: A systematic review
Supplemental Material, sj-docx-2-cob-10.1177_26335565211032880 for The incidence of multimorbidity and patterns in accumulation of chronic conditions: A systematic review by Prtha Kudesia, Banafsheh Salimarouny, Meagan Stanley, Martin Fortin, Moira Stewart, Amanda Terry and Bridget L Ryan in Journal of Comorbidity
Supplemental material
Supplemental Material, sj-pdf-1-cob-10.1177_26335565211032880 - The incidence of multimorbidity and patterns in accumulation of chronic conditions: A systematic review
Supplemental Material, sj-pdf-1-cob-10.1177_26335565211032880 for The incidence of multimorbidity and patterns in accumulation of chronic conditions: A systematic review by Prtha Kudesia, Banafsheh Salimarouny, Meagan Stanley, Martin Fortin, Moira Stewart, Amanda Terry and Bridget L Ryan in Journal of Comorbidity
Footnotes
Authors’ note
Banafsheh Salimarouny and Prtha Kudesia are joint first authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.