
Abstract
Objectives
This is the first systematic review and meta-analysis of the prevalence of multimorbidity, its risk factors including socioeconomic factors, and the consequences of multimorbidity on health systems and broader society in India.
Methods
A systematic review of both published and grey literature from five databases (Medline, Embase, EBSCO, Scopus, and ProQuest) was conducted including original studies documenting prevalence or patient outcomes associated with multimorbidity among adults in India. We excluded studies that did not explicitly mention multimorbidity. Three independent reviewers did primary screening based on titles and abstracts followed by full-text review for potential eligibility. The risk of bias was independently assessed by two reviewers following the Appraisal Tool for Cross-Sectional Studies. We presented both qualitative and quantitative (through meta-analysis) summaries of the evidence. The protocol for this study was prospectively registered with PROSPERO (CRD42021257281).
Results
The review identified 5442 articles out of which 35 articles were finally included in this study. Twenty-three studies were based on the primary data while 12 used secondary data. Eleven studies were conducted in hospital/primary care setting while 24 were community-based. The pooled prevalence of multimorbidity based on (n=19) studies included for meta-analysis was 20% (95% CI: 19% to 20%). The most frequent outcomes were increased healthcare utilization, reduced health-related quality of life, physical and mental functioning.
Conclusion
We identified a wide variance in the magnitude of multimorbidity across age groups and regions with most of the studies from eastern India. Nation-wide studies, studies on vulnerable populations and interventions are warranted.
Introduction
Multimorbidity, the co-occurrence of two or more chronic conditions in an individual is becoming a norm in low-and middle-income countries (LMICs). 1 This can be attributed to the rise in the ageing population along with an increase in non-communicable diseases (NCDs) vis-a-vis prevailing infectious diseases. 2 Multimorbidity encompasses all long term conditions (LTCs) including NCDs of chronic nature such as hypertension, diabetes or an infectious disease of longer duration such as filariasis or a mental health condition such as depression. This often leads to an increase in healthcare utilization, expenditure along with poorer patient outcomes. 3 Further, it also deteriorates the health-related quality of life (HRQoL). 4
In LMICs such as India, multimorbidity is on the rise; evident by a recent study that estimated a 55% prevalence among adults attending public healthcare facilities. 5 However, the evidence on multimorbidity burden is scattered across various studies done in either small samples or particular regions, but no study to date has synthesized the national estimates. Although, the high prevalence indicates an additional burden on the already swamped healthcare system, the national estimate of multimorbidity burden could help in evidence based guidance to plan changes to the structure and delivery of primary care. Primary care is the first and foremost point of contact between multimorbid individuals and the healthcare systems. 6 It is thus imperative to strengthen primary care along with healthcare advancements to mitigate multimorbidity and its challenges such as polypharmacy, and unplanned emergency healthcare use. This also lays a financial burden on families making them vulnerable to impoverishment. 7 Additionally, multimorbid patients face convoluted care pathways as they navigate to multiple care providers and specialists for each of the condition. 8 Moreover, the existing guidelines focus on single disease-based management which makes it challenging for the healthcare providers to manage multiple long-term conditions. 8 Hence, multimorbidity and primary care research needs to be prioritized, for both resource and planning, and to identify effective interventions.
With emerging epidemiological trends of chronic conditions and transitioning demography, generating evidence on the burden of multimorbidity is new in Indian context. 9 Although, multimorbidity has become a norm, still multimorbidity and primary care research has not gained pace in the country. 9 A systematic review conducted in 2015, estimated 4.5% to 83% prevalence of multimorbidity in South Asia. 10 Given the increasing prevalence, there is a pressing need to assess the burden and outcomes of multimorbidity in India. Moreover, India has the second-largest population in the world which in itself reflects the need for special attention. Recent programs such as Ayushman Bharat and the establishment of Ayushman Arogya Mandir formerly Health and Wellness Centres along with integrating AYUSH (Ayurveda, Yoga & Naturopathy, Unani, Siddha, Sowa Rigpa, Homoeopathy) system in the mainstream medical facilities shows India’s commitment to Universal Health Coverage (UHC) which could be given direction with a shred of cumulative evidence. 11 Nonetheless, various LMICs face similar situation in managing multimorbidity despite its rising prevalence. Additionally, the social determinants of multimorbidity remain alike for most of the LMICs and hence, identifying these determinants through the present review would generate relevant evidence for a wider population. These determinants can help in making the healthcare system aware and resilient towards the chronic care needs of local people. Therefore, this systematic review aimed to estimate the prevalence of multimorbidity, identify its risk factors including social determinants or consequences of multimorbidity in India.
Methods
Protocol and standards
This systematic review was prospectively registered with the International Prospective Register of Systematic Reviews (Registration ID: CRD42021257281). 12 It was performed and reported following Preferred Reporting Items for Systematic reviews and Meta-analysis (PRISMA) guidelines (Supplementary Table S1). 13
Eligibility criteria
Original studies documenting prevalence, determinants or patient outcomes associated with multimorbidity; studies with participants aged ≥18 years; conducted either in a primary care/outpatient or community based setting from India were included. Studies in which multimorbidity was not explicitly defined; or included an index condition i.e. comorbidity were excluded. Additionally, systematic reviews, commentaries, editorials, newsletters and qualitative studies were also excluded.
Information sources and search strategy
We searched both medical literature databases and grey literature to make our search exhaustive. A comprehensive search was conducted using electronic databases Medline through PubMed and Embase along with EBSCO host and ProQuest. Google Scholar search engine was also used to retrieve articles. The reference list of included studies was hand-searched as an additional source of information.
The basic search syntax comprised of two concepts: multimorbidity and prevalence. We used PubMed to build the basic search strategy, although the individual search strategy for each database was developed separately. In PubMed, medical subject headings (MeSH) term for “multimorbidity” was entered in 2018. 14 However, for other databases the terms specific to database such as Emtree for Embase along with various other keywords were used to make the search strategy comprehensive. Thereafter, search strategy was refined to include data from India only. The detailed search strategy used for each database is provided in Supplementary Table S2. We included articles published up until August 2021.
Study selection, data extraction and synthesis
The studies retrieved from various databases were merged and screened for duplicates. Primary screening based on the titles and abstracts (following inclusion and exclusion criteria) was done by three reviewers (RV, AS and MB) independently. The articles were categorized as relevant, irrelevant or unsure; if any article was marked as irrelevant by all three of the reviewers it was eliminated. In the next stage, full texts of all included articles from primary screening were reviewed by three independent reviewers for potential eligibility (RV, AS and MB). This round strictly followed inclusion and exclusion criteria based on which studies were finally included. Any dissent was resolved by forming a consensus with the help of another reviewer (SP).
Data from relevant studies were extracted using a preformed and piloted data extraction sheet and entered by three independent reviewers (RV, AS and MB). This data was assessed by another reviewer (SP) to check for disparities. Differences in the data extraction were resolved by the entire team in consensus. Additionally, if the data was not clear, we contacted the respective authors for further clarity. We extracted the following information from the included studies: author, journal title, year of publication, study design, study setting, age, sex, sample size, prevalence, patterns and patient outcomes of multimorbidity. Additionally, we also collated data on definition of multimorbidity used, tool used for measuring multimorbidity, self-reported or objectively assessed, total number and list of long term conditions included.
Risk of bias in individual studies
The risk of bias was independently assessed by two reviewers (RV, AS) following the Appraisal tool for Cross-Sectional Studies (AXIS) that addresses cross-sectional study reporting and overall quality. 15 The AXIS tool comprehensively assesses studies based on twenty questions from the introduction (one question), methods (ten questions), results (five questions), discussion (two questions) and others (two questions). The AXIS tool covers the following key domains: study design, sample size, sampling method, and methods. Any potential differences between the reviewers were resolved by the third reviewer (SP). Each of the criteria was evaluated on its presence (“Yes” =1) or absence (“No”/ “Do not know”=0). The percentage of items presented as ‘yes’ was then calculated. Each question was scored with a possible score of one, with scores of each question summed to provide an overall score of twenty. The AXIS repartition: 0–50% has high risk of bias, 51–80% has medium risk of bias and 81–100% has low risk of bias.
Summary measures
The findings were summarized as qualitative and quantitative summary of the evidence. We qualitatively described the characteristics of the included studies whereas pooled prevalence estimates represented the quantitative summary. We used STATA version 17.0 (STATA Corp., Texas) for data analysis. We used ‘metan’ command to calculate the pooled prevalence based on random-effect model. The I2 statistic was used to assess the variability between studies; this statistic can take values between 0% and 100%, with high values indicative of strong heterogeneity. We anticipated a high heterogeneity due to the nature of selected studies such as nationally representative samples vs. primary studies with relatively smaller sample size; and age group variations in the study i.e. 18 years and above or older adults like ≥45 years or ≥60 years. Hence, we planned sub group analysis based on the nature of data i.e. primary data or secondary data and age group considered i.e. ≥18 years or ≥45 years.
Patient and public involvement
We did not involve patients or the public in the design, or conduct, or reporting, or dissemination plans of our research.
Results
We retrieved 5442 articles from the electronic databases after excluding 584 duplicates. A total of 35 articles5,16-49 met the inclusion criteria after primary as well as full-text screening, and quality appraisal (Figure 1). PRISMA flow diagram representing selection of studies included in systematic review.
General characteristics of selected studies
Characteristics of the included studies.

NR: Nationally representative, UT: Union Territory, IHDS- India Human Development Survey, WHS-World Health Survey, SAGE-Study on Global Ageing and Adult Health, LASI-Longitudinal Ageing Study in India, UNFDPA-United Nations Population Fund, BKPAI
Assessment of risk of bias
A total of 36 studies qualified for the quality check. We excluded one study which explored management of geriatric multimorbidity in old age home residents in India 50 as it scored only four points (20%). The quality appraisal of the remaining 35 included articles revealed that 15 studies scored 81-100% and were categorized as having low risk of bias,17,18,20,28,29,32,33,37,39,41-43,46-48 whereas 20 studies scored 51-80% and were grouped as having medium risk of bias5,16,19,21-27,30,31,34-36,38,40,44-45,49 (Supplementary Table S4).
Prevalence
The prevalence of multimorbidity was reported in 32 of the included studies and this ranged from 1.16% to 65.9% (Table 1). Three studies did not report the prevalence of multimorbidity.20,41,44 The prevalence from twelve studies with a nationally representative sample ranged from 8.9% to 63.3% while the prevalence of multimorbidity from primary studies ranged from 16.2% to 65.9%. 5 17,19,20,22,25-29,32-35,37,39-43,45-48 The estimate of multimorbidity for Odisha (state with maximum studies, n=15)5,17,19,25,26,28,32-34,39,40,42,45,47,48 ranged from 23.3% to 63.06% whereas for other states the prevalence ranged from 16.2 % to 65.9%.20,22,27,29,35,37,41,43 Based on the age, among ten studies with a population of ≥60 years, the prevalence ranged from 30.7% to 65.9%. Similarly, the prevalence reported for studies that considered population aged ≥18 years (n=13) and ≥45 years (n=5) ranged from 1.16% to 55% and 9% to 63.06% respectively.
We included 19 studies for meta-analysis which gave a pooled prevalence of multimorbidity to be 20% (Figure 2). Separate meta-analysis was also conducted for studies reporting multimorbidity based on primary data which yielded the pooled prevalence of 43% (Supplementary Figure 1) while studies based on secondary data showed the pooled prevalence to be 4% (Supplementary Figure 2). We also conducted a separate meta-analysis on the basis of age group selected i.e. studies reporting multimorbidity among participants aged ≥18 years that showed the pooled prevalence of 14% (Supplementary Figure 3) while studies among respondents aged ≥45years showed the pooled prevalence of 23% (Supplementary Figure 4). The list of studies excluded from meta-analysis along with their reasons for exclusion is presented in Table 2. Pooled prevalence of multimorbidity in India. List of studies excluded from meta-analysis along with their reasons for exclusion.

Pattern
Patterns of multimorbidity.

as per the availability of information; Dyad: combination of frequently occurring two condition; Triad: combination of frequently occurring three conditions; Tetrad: combination of frequently occurring four conditions; NA: Not Available.
Risk factors
Risk factors/determinants/correlates for multimorbidity reported in studies.

APL: Above poverty line; ARRR: Adjusted Relative Risk Ratio; AOR: Adjusted Odds Ratio; BMI: Body Mass Index; SES: Socioeconomic status; IRR: Incidence risk ratio; SC: Scheduled Caste; ST: Scheduled Tribes; OBC: Other backward class; CI: Confidence Interval.
Outcome/consequences
Summary of the relationship between multimorbidity and its patient outcomes (health outcomes, expenditure, and utilization).
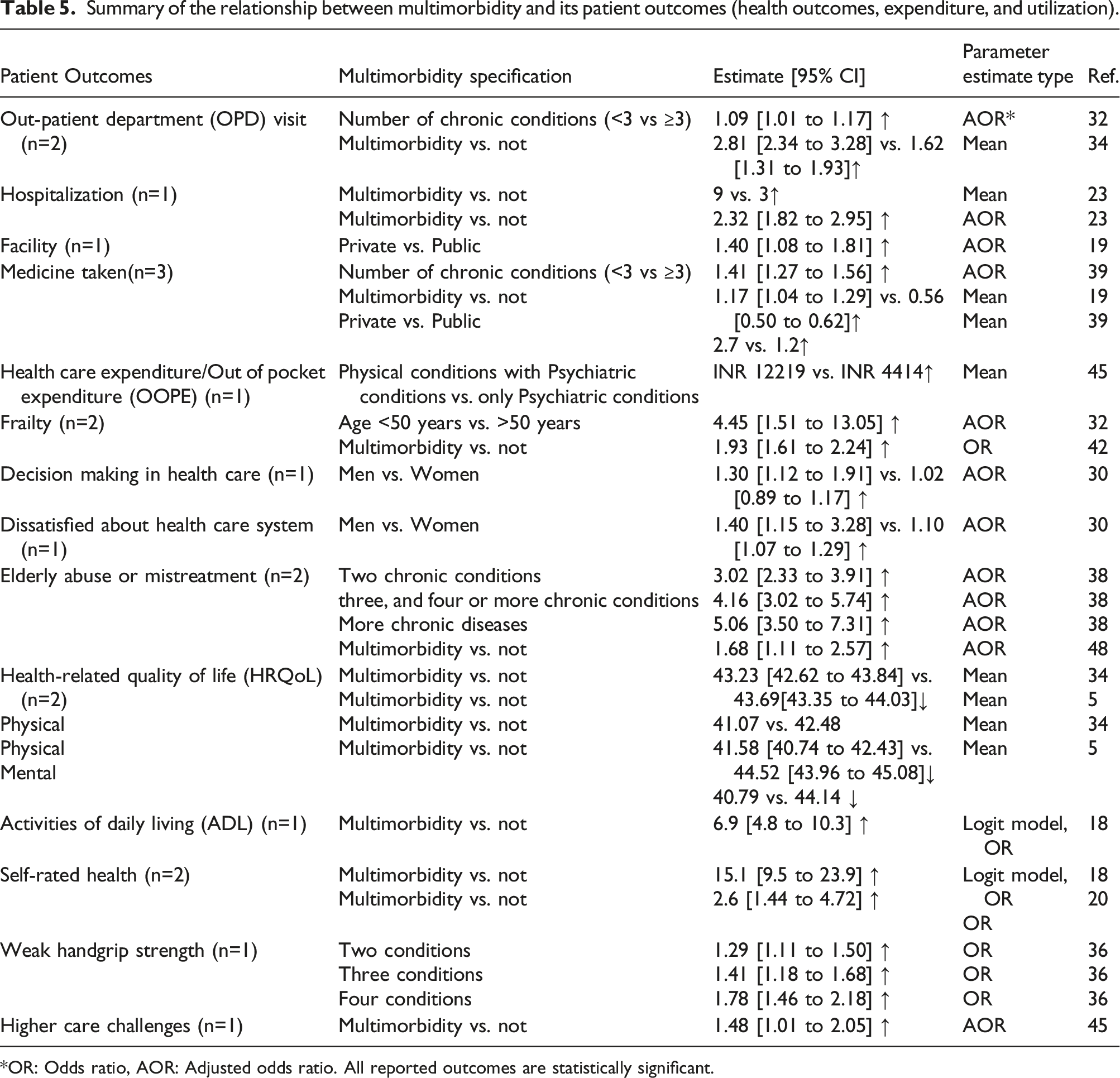
OR: Odds ratio, AOR: Adjusted odds ratio. All reported outcomes are statistically significant.
Discussion
Summary of evidence
This systematic review provides comprehensive evidence on the burden of multimorbidity in India. The prevalence of multimorbidity was observed to vary from 1.16% to 65.9%. Nonetheless, the retrieved studies were heterogeneous in the characteristics while the prevalence was quite similar between the different subgroups i.e., nationally representative samples and samples from different provinces in India. The prevalence was high among participants aged 60 years and above (range 30.7% to 65.9%). The studies which were planned a-priori focused on more number of chronic conditions (median 18) whereas the median conditions considered in studies based on secondary data was 9 while the overall median number of diseases considered was 12.
Comparison with existing literature
There is considerable heterogeneity among the measures used to assess multimorbidity in terms of number of diseases considered. In this review, the median numbers of diseases identified were 12 which is lower than the median number [Median: 17 (IQR: 11-23)] of conditions reported by a systematic review of 566 studies on multimorbidity. 51 Additionally, there was a variance in the median number of conditions considered in primary and secondary studies. A probable reason for the wide variance between the two is that the latter does not intend to assess multimorbidity rather the data is extrapolated to do so due to a lack of nationwide data pertaining to multimorbidity. Hence, there is an urgent need towards building a consensus on the number of diseases or groups to be included to assess multimorbidity which would help in improving inter-regional comparisons. 52 Moreover, LMICs such as India should plan to conduct nation-wide surveys on multimorbidity to elicit its real burden. 53 Here, the findings of a systematic review of systematic reviews is worth considering that recommended meaure selection (eg., using a cut-off of two or more conditions) be used for tools validated for the outcome of interest, and where there is no validated measures, or where multiple outcomes or populations are being considered, disease count should be used as an alternative. 54 Additionally, debates around the consideration of definition for complex multimorbidity is also worth considering where a study suggests that complex multimorbidity must consider complexity of conditions rather than simple count of diseases across body systems. 55
We observed that the population aged 60 years and above had a higher prevalence (range 30.7% to 65.9%) of multimorbidity which is in contrast with the findings reported from China 56 which showed a very wide range (6.4% to 76.5%), though the latter was based on a narrative review. However, the pooled prevalence of multiple chronic illnesses reported in Caribbean and Latin American countries 57 was 47% which is higher than the pooled prevalence reported in our review. An Australian study 58 reported 52% prevalence which is also higher than the prevalence of multimorbidity in India. The presence of clusters of conditions or complexity (the number of domains present) increased with age. Similar findings were also observed from another study in Australia 59 where 83.2% of the surveyed participants aged 75 years or older had multimorbidity; with 58.2% having morbidity in three or more domains, and 33.4% in four or more. As the ageing population increases, multimorbidity will continue as a major health problem in the years to come 60 which needs urgent action.
In this review, we observed an increase in the health care cost and utilization which is consistent with the findings of Bori et al 61 in UK. Only twelve studies reported patterns/ clusters/disease combinations but it indicated a shift in the conceptualization of multimorbidity from purely disease count to specific disease combinations/clusters. Additionally, we also noted the focus on specific age groups to be a trend in this review. These findings are consistent with the report of Bori et al. 61 Nonetheless, it is worth mentioning that these findings were not elicited by an earlier systematic review conducted among South Asian population 10 as the term multimorbidity was not defined in the MeSH (Medical Subject Headings of PubMed) terminology at that time.
Multimorbidity assessment largely depends on considering the simple count of diseases, however future studies should explore the most common combinations and frequently occurring clusters of diseases that could help in providing insights for the complex care needs of patients with multimorbidity. The health research as well as practice has conventionally focused on single-disease framework rather than multiple conditions. Therefore, a complementary strategy is needed, supporting general physicians to provide personalized patient centered, comprehensive continuity of care, especially in socioeconomically deprived areas. 62 Additionally, future studies eliciting the burden of multimorbidity among vulnerable populations such as urban poor, and tribal are warranted. Social determinants of health are equally relevant for chronic conditions and studies report that socio-economic marginalization increases the risk of multimorbidity.63,64 Furthermore, the difficulties for these individuals are exacerbated by the ‘inverse care law’ which states that the rising demand for healthcare access leads to fewer consultations, decreased patient enablement and increased physician stress. 65 Hence, these factors highlight the importance of estimating the burden of chronic conditions and identifying their care seeking pathway so as to make the existing programmes more equitable and design future policies based on the evidence. Nonetheless, few studies have been published covering these vulnerable groups which were beyond the date of last search of this review.66-74
We also observed that studies were mostly conducted among patients attending out-patient department of primary care though no studies document the prevalence of multimorbidity among in-patients (IPD). A major gap exists in enumerating the care seeking pathway of these multimorbid individuals which may support in further taking steps towards primary care strengthening. We observed Multimorbidity Assessment Questionnaire for Primary Care (MAQ-PC) was the only validated tool which was designed to explicitly assess multimorbidity in India. 25 With a lack of gold standard, this tool has been developed following an iterative process that can be used for undertaking multimorbidity studies in future.
We observed affluence to be associated with multimorbidity which is consistent with the findings of a systematic review on multimorbidity in LMICS that observed an increased risk of NCD multimorbidity [Pooled OR from 10 studies: 1.35 (95% CI: 1.02 to 1.80)] among well-off individuals. 75 A possible explanation to this could be that affluent group has a higher capacity to pay for healthcare services which lead to better diagnosis and hence, self-report of multimorbidity. However, these findings differ from that of high-income countries where deprivation is associated with multimorbidity as suggested by a systematic review. 76 Additionally, most studies reported that the individuals with more years of schooling (either primary or secondary schooling) had a higher chance of having multimorbidity as compared to those with no formal education which is consistent with the findings of a systematic review that included studies from Southeast Asia. 72 A probable reason for this could be that with education, people tend to be more health conscious, and hence have better chances of diagnosis and self-report of chronic conditions.
Implications for research and practice
India is a federal union comprising of 28 states and 8 union territories, forming a total of 36 entities. The studies on multimorbidity within a state are very limited preventing the assessment of the actual burden in the country. The present evidence may be considered as a tip of the Iceberg. More studies specific to different zones of the country, state/province is required to assess the real burden of multimorbidity in India. India is a country of medical pluralism wherein apart from conventional medicine system, traditional and alternative system of medicine popularly known as Ayurveda, Yoga and Naturopathy, Unani, Siddha, and Homeopathy (AYUSH) are also instrumental in contributing to health care. AYUSH care utilization is higher among patients with chronic diseases and also for treating skin-related and musculo-skeletal ailments. 70 The current epidemiological transition has been a major driver impelling a radical rethink of the structure of health care, especially concerning the role, quality and capacity of primary health care. The development of new clinical care guidelines should be addressed to focus on multiple systems and not just only on one disease. Sensitization of frontline workers such as Accredited Social Health Activist (ASHA) and Community Health Officer (CHO) towards the needs of multimorbid individuals is required with a focus on family-level interventions for shared risk factors. 77 Capacity building of primary care staff to manage multimorbidity is also needed. Nonetheless, most LMICs face a similar healthcare challenge in combating multimorbidity where the determinants, patient outcomes as well as impact of multimorbidity on health system remain alike. Hence, the findings of this study could also be extrapolated to countries with similar demographic and epidemiological transition along with similar health systems by targeting these determinants.
Strengths and limitations
We employed a comprehensive search strategy in various databases to find out exhaustive list of all available articles in the domain. Further, screening, data extraction and analysis were performed following prospectively registered protocol. Meta-analysis was done to synthesize the pooled prevalence which was a major strength of this study. However, heterogeneity and repetition in data led us to include only 19 articles in the meta-analysis. This review includes sample from both community and primary care set ups which is an additional strength. However, the fact that this study is restricted to India alone may be seen as a drawback. Nonetheless, India is the second-most populous nation in the world, hence it was imperative to perform this review for future policy decisions.
Conclusion
Multimorbidity has become a norm in India. The increasing burden of multimorbidity among older adults cannot be overlooked. Nation-wide primary studies to investigate the real burden of multimorbidity are warranted. Additionally, studies pertaining to vulnerable groups such as urban poor and tribal along with interventions are also warranted. Uniform methods to assess multimorbidity are required.
Supplemental Material
Supplemental Material - Epidemiology and impact of chronic disease multimorbidity in India: a systematic review and meta-analysis
Supplemental Material for Epidemiology and impact of chronic disease multimorbidity in India: a systematic review and meta-analysis by Roja Varanasi, Abhinav Sinha, Meenakshi Bhatia, Debadatta Nayak, Raj K Manchanda, Rajeev Janardhanan, John Tayu Lee, Simran Tandon, Sanghamitra Pati in Journal of Multimorbidity and Comorbidity
Footnotes
Acknowledgements
We thank Dr. Banamber Sahoo, Library and Information Officer, ICMR-Regional Medical Research Centre, Bhubaneswar for his support in developing search strategy and providing access to databases. We are also thankful to Dr. Srikanta Kanungo, Scientist-D, ICMR-Regional Medical Research Centre, Bhubaneswar for helping us with the meta-analysis.
Author contributions
Concept and design: RV, AS and SP. Acquisition, analysis, or interpretation of data: RV, AS, MB, DN, RKM, RJ, ST, JTL and SP. Drafting of the manuscript: RV, AS, DN and SP. Critical revision of the manuscript for important intellectual content: MB, RKM, RJ, JTL and ST. Statistical analysis: RV and AS. Administrative and technical support: RJ, ST and SP. Supervision: SP. All authors have agreed on publishing the final version of manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Correction(August 2024):
Article updated to include department name “Faculty of Medical & Health Sciences” in the affiliation of author “Rajiv Janardhanan”. The revised affiliation is “Faculty of Medical & Health Sciences, SRM Institute of Science & Technology, Kattankulathur, India”.
Ethical statement
Data availability statement
All data underlying this research will be made available on reasonable request to the authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.