
Abstract
The protooncogene product HER-2/
T
IHC is faster and more economical than FISH. However, results from IHC are subjective and semiquantitative, at best. The method, therefore, is difficult to standardize and highly dependent on use of proper controls. Different antibodies and IHC techniques have been used for detection of HER-2/
Several studies have demonstrated that breast cancers positive for HER-2/
Theoretically, a more appealing approach to identify candidates for Herceptin (Genentech) treatment would be to use trastuzumab as the primary antibody in IHC. Trastuzumab is a hybrid molecule consisting of the antigen-binding fragment (Fab) of the murine monoclonal antibody 4D5 and the Fc fragment of human IgG (Press et al. 2002). Humanization of the Fc fragment minimizes host immune response against the drug and enhances recruitment of immune cells to the binding site (Tokuda et al. 1996). However, this modification also makes it impossible to use traditional IHC amplification systems because anti-human secondary antibodies bind to endogenous antibodies present in human tissue sections. This results in high background staining making unambiguous interpretation of the results impossible. To overcome this, researchers have used biotinylated trastuzumab with the streptavidin system for revealing antibody staining (Bussolati et al. 2005). This approach demonstrated the potential of using the therapeutic antibody for identification of patients for treatment.
We have developed a novel method to perform IHC for detection of HER-2/
Materials and Methods
Tissue Samples
All tissue samples were obtained from the fixed tissue biorepository of Asterand (Detroit, MI). All samples were collected from surplus surgical material with full informed patient consent under Institutional Review Board-approved protocols for research purposes.
Four breast cancer tissue microarrays (TMA) were prepared from formalin-fixed, paraffin-embedded tissues with 0.6-mm diameter cores using a TMA arrayer (Beecher Instruments; Silver Spring, MD). TMA 60 with 342 tissue cores from 58 patients (including tumor tissue cores and adjacent normal tissue cores from the same cases); TMA 188 with 231 tissue cores from 77 cases (including tumor tissue cores and corresponding normal tissue cores); TMA 126 with 360 tissue cores (including 10 cases of normal mammary tissues and 110 cases of breast adenocarcinoma); TMA 203 with 360 tissue cores from 120 cases. All tissues on each array were represented by at least three cores that were selected after diagnosis was confirmed and representative areas were marked by a pathologist. Various histological forms of the breast cancer were represented on the arrays. Four-μm sections were cut and placed on coated glass slides using a tape-transfer system (Instrumedics Inc.; Hackensack, NJ).
Biotinylation of Trastuzumab
Biotinylation of trastuzumab was performed using the Biotintag Microbiotinylation kit from Sigma (St Louis, Mo) according to manufacturer's instructions. Briefly, trastuzumab was diluted with PBS to 100 μl, to which 10 μl BAC-Sulfo NHS at 5 mg/ml in DMSO was added. The mixture was incubated at room temperature for 30 min. Biotinylated trastuzumab was purified using a G-50 column (supplied in the kit). Four fractions at 200 μl each containing biotinylated trastuzumab were collected, and protein concentrations were determined using the Bradford assay (Bradford 1976). Protein concentration of the biotinylated trastuzumab in the first fraction was 10 μg/μl. This fraction (200 μl) was used for staining, and the concentration is equivalent to that of the unmodified trastuzumab in this study.
Pilot Studies for Optimal IHC Staining Conditions
Optimal IHC staining conditions were tested on full sections from breast HER-2/
IHC Manual Staining Procedures
IHC using antibodies of HercepTest (Dako) unmodified trastuzumab, ani-HER-2/
Manufacturer's instructions were followed for HercepTest staining. Briefly, epitope retrieval was performed at 97C for 40 min with the supplied epitope retrieval solution. Slides were cooled for 20 min at room temperature in the same solution. All subsequent steps were performed at room temperature. Peroxidase was blocked using the supplied reagent. Arrays were incubated with the primary antibodies for 30 min, then with the visualization reagent for 30 min, and finally with DAB. Arrays were counterstained with hematoxylin and mounted in permanent medium.
For staining with unmodified trastuzumab, sections were incubated in antigen-retrieval solution (Dako) for 20 min. The slides were cooled for 20 min at room temperature. All subsequent treatments were at room temperature. Slides were washed three times with PBS (pH 7.6) and incubated for 10 min in peroxidase blocking system (Dako). They were washed three more times in PBS and incubated for 5 min in Super Block (ScyTek Laboratories; Logan, UT) to block general nonspecific tissue reactivity. They were washed again with PBS and incubated with Human-to-Human blocking reagent (prepared for Asterand by ScyTek Laboratories) for 60 min. They were washed with PBS before incubation for 30 min with trastuzumab (Herceptin, Genentech; a generous gift from Dr. Weizen Wei, Barbara Ann Karmanos Cancer Institute, Wayne State University, Detroit, MI) diluted 1:100 in antibody diluent (Dako). Slides were washed in PBS and incubated in 1 μg/ml of mouse biotin-conjugated anti-human IgG (BD Pharmingen; San Diego, CA) diluted in antibody diluent, followed by PBS washing and 10-min incubation in prediluted streptavidin-peroxidase from LSAB2 system (Dako) according to the manufacturer's instructions. Slides were washed again in PBS, the color was developed by 5-min incubation in DAB/H2O2, and then counterstained with hematoxylin.
For staining with rabbit polyclonal antibody, deparaffinization and antigen retrieval were performed as described for unmodified trastuzumab. Slides were incubated for 20 min with the ani-HER-2/
The same deparaffinization and antigen-retrieval procedures were also used for staining with biotinylated trastuzumab. Slides were incubated in a final dilution of 1:50 of this reagent in antibody diluent for 1 hr at room temperature, followed by incubation with streptavidin-peroxidase from the LSAB2 system (Dako) for 15 min. Color was developed by 5-min incubation in DAB/H2O2. Slides were counterstained with hematoxylin.
IHC Automated Procedure
Following deparaffinization and antigen retrieval as described, the slides were immersed in Tris buffered saline with Tween 20 (TBST) for 15 min. They were placed on a Dako Autostainer and were rinsed again in TBST.
Staining protocol with trastuzumab was as follows: peroxidase block for 5 min, followed by TBST wash; Superblock (ScyTek Laboratories) for 5 min, excess blown off, no rinse; Human-to-Human blocking reagent (ScyTek Laboratories) for 70 min followed by TBST washes; trastuzumab 1:100 dilution for 30 min followed by TBST wash; biotinylated anti-human IgG (1 μg/ml) for 30 min followed by TBST wash; LSAB2 streptavidin-horseradish peroxidase (HRP) labeled ready-to-use (RTU) for 15 min, TBST wash; DAB substrate and chromogen for 5 min followed by TBST wash.
Staining protocol with polyclonal anti-HER-2/
Double-staining protocol was the same as for trastuzumab alone except trastuzumab and the rabbit polyclonal anti-HER-2/
Slides were removed from the autostainer, washed twice for 5 min with PBS, and incubated in BCIP/NBT substrate until a bright blue color developed (∼2 hr), followed by washes in PBS. No counterstaining was performed.
Counterstaining, dehydration, and placement of coverslips were performed manually.
Scoring
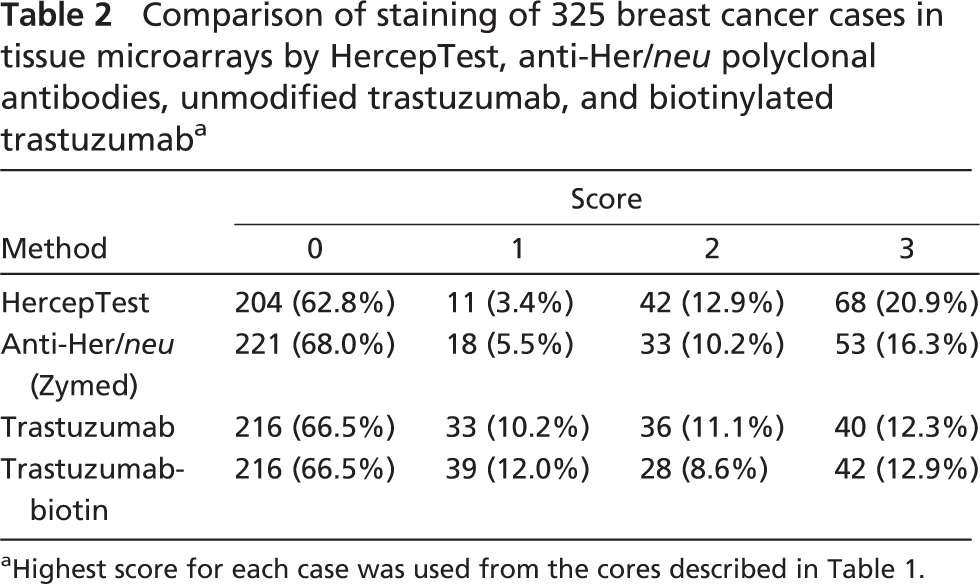
Slides were evaluated by a single pathologist (AG) according to routine procedures (Birner et al. 2001). The four-tiered scoring system (0, 1+, 2+, 3+) was applied. On arrays, each case was represented by three spots. The highest of the scores was attributed to the case. Samples with scores of 0 or 1 can be classified as ‘negative’ and those with scores of 2 or 3 as ‘positive’ in the manner used for clinical testing. There were 325 cases for which results were obtained using all four staining methods.
Results
All antibodies except the standardized HercepTest (Dako) were titrated on full sections of breast HER-2/
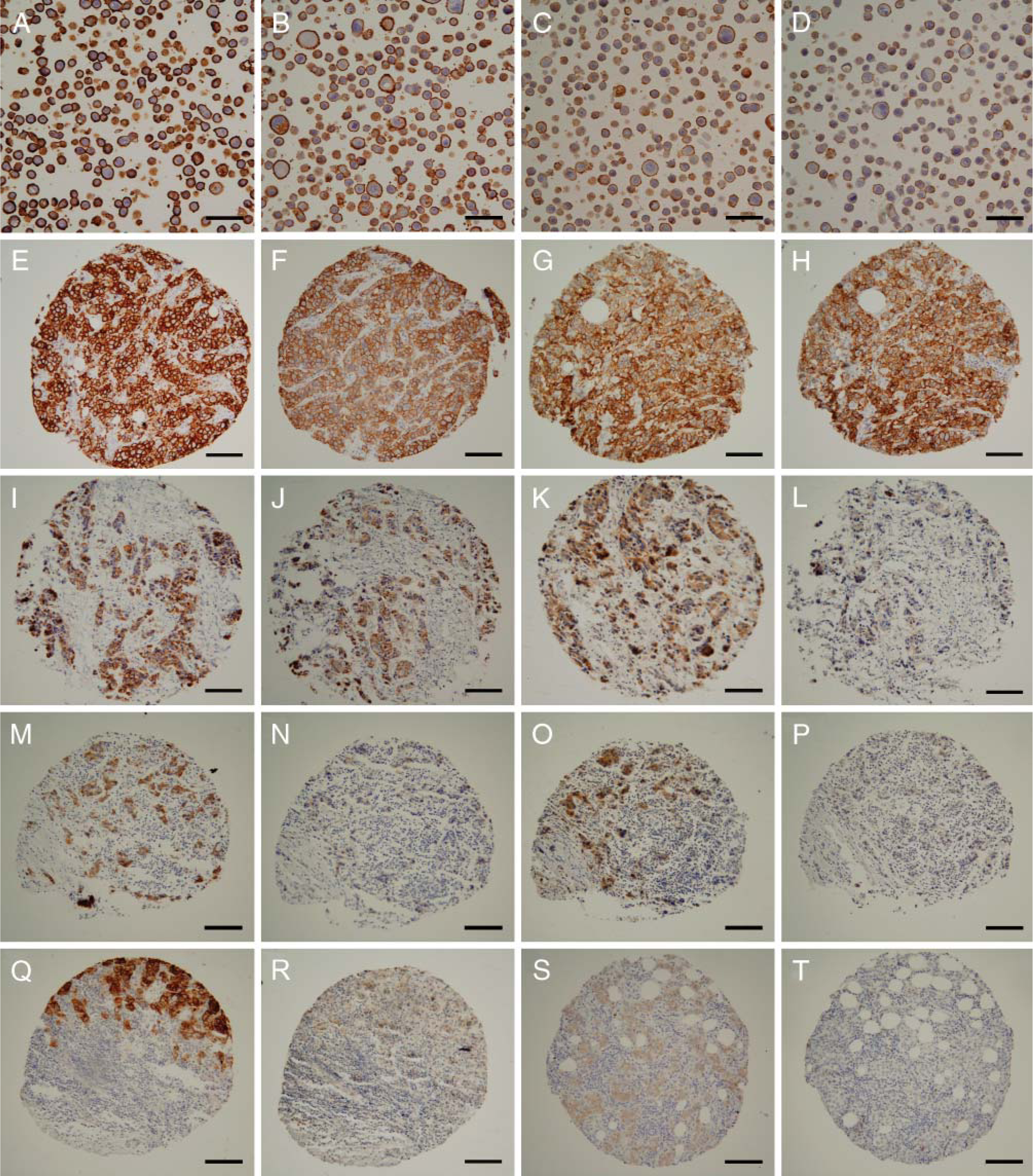
All methods were tested on the control cell line slides provided with HercepTest (Dako). Results demonstrated valid staining by all four methods, with strong brown (3+) membrane staining on SK-BR-3 cells (Figures 1A-1D), weak staining (1+) on MDA-175 cells (results not shown), and no staining on MDA-231 cells (results not shown). Although all methods resulted in 3+ staining of the positive cell line, there was some variation in staining intensity among the different methods. Staining intensity was highest with HercepTest (Figure 1A), followed by the Zymed polyclonal anti-HER-2/
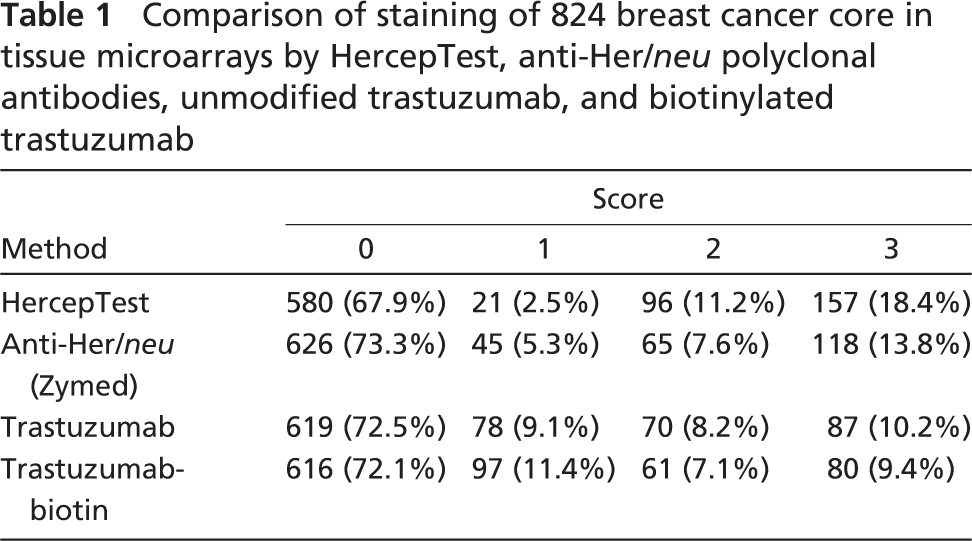
To compare the staining of the four antibodies over a large number of patient samples in a high-throughput fashion, four breast cancer TMAs were used. The results for staining of 824 individual cores representing 325 cases of breast cancer are shown in Table 1 and Table 2. In the majority of cases, similar staining patterns were seen with all four methods. There was prominent membrane staining on cancer cells and no significant staining of stromal cells or neighboring normal cells (Figures 1E-1H). None of the antibody preparations gave perceptible staining with normal samples present on the arrays. When serial sections stained with the different antibodies were compared, corresponding cores showed the most intense staining (2+ and 3+) with HercepTest (Dako) (Table 1). In some cases, cores reacted with all of the antibodies except biotinylated trastuzumab (Figures 1I-1L). This is also evident by the fact that only 16.5% of the cores were scored as 2+ and 3+ with this antibody. Staining by the Zymed polyclonal anti-HER-2/
Results for cases represented in TMA experiments based upon the highest score for any of the replicates are summarized in Table 2. The majority of cases were recognized as positive or negative by all methods used. There were 156 (48%) cases that were given a score of 0 with all four assays and 31 (9.85%) cases were scored 3+ by all methods. Intermediate scores showed little concordance between assays with only one case with a score of 1 and six cases with a score of 2 in all assays. There were six cases scored as 3+ using HercepTest (Dako) that were 0 or 1+ with both methods using trastuzumab. For cases scored as 2+ with HercepTest, there were 28 cases not recognized by the trastuzumab methods. Interestingly, there were three cases that scored 2+ or 3+ with unmodified trastuzumab, which were not recognized by HercepTest (score 0) and two of these had a score of 0 with the Zymed polyclonal. The remaining case was scored as 2+ with the Zymed reagent.
It is possible that the discrepancies between results obtained with the different antibodies are due in part to the small (0.6 mm) cores on these high-throughput TMAs. Therefore, experiments were performed using whole sections of breast cancer samples to compare staining with the Zymed polyclonal antibody and unmodified trastuzumab. An autostainer was used for these sections to standardize staining. There were no significant differences in staining with either antibody between the manual method and the autostainer when serial sections were compared (data not shown). All further experiments were performed using the autostainer. A total of 32 cases were examined using full serial sections. Of these, half (16 cases) were negative by both methods. There were nine cases that were positive with both trastuzumab and the anti-HER-2/
Reactivity of the two antibodies was examined in more detail using a double-labeling procedure. Studies were performed on full sections from 14 cases, some negative for both antibodies, some positive for both, and several where there was staining discordance in the TMA study. TMA-negative cases were negative when full sections were examined (data not shown). Samples reactive with both antibodies displayed membrane staining that was usually uniform, giving a mixed color as depicted in Figure 2A, and other slides displayed wide areas of mosaic staining (Figures 2B and 2C).
Comparison of HercepTest, polyclonal anti-HER-2/
Comparison of staining of 824 breast cancer core in tissue microarrays by HercepTest, anti-Her/
Cases that were positive with the polyclonal anti-HER-2/
Discussion
Targeted therapies in oncology such as trastuzumab require accurate selection of patients whose tumors express the target molecule. None of the current methods used for selecting responsive patients for trastuzumab therapy is completely satisfactory. The most widely used and cost-effective method is IHC, where there are a number of different antibodies in use worldwide (van de Vijver 2001). Each antibody performs differently depending on the fixative conditions and is associated with different parameters of sensitivity and specificity (Gancberg et al. 2000). One study demonstrated that monoclonal antibody A0485 and HercepTest (Dako) were the most sensitive antibodies, whereas TAB250 was the most specific (Ginestier et al. 2004). HercepTest was less sensitive than the R60 polyclonal antibody and the monoclonal 10H8 in another study (Press et al. 2002). In our hands, HercepTest also demonstrated the highest sensitivity among the methods used. The importance of the choice of antibody used to detect HER-2/
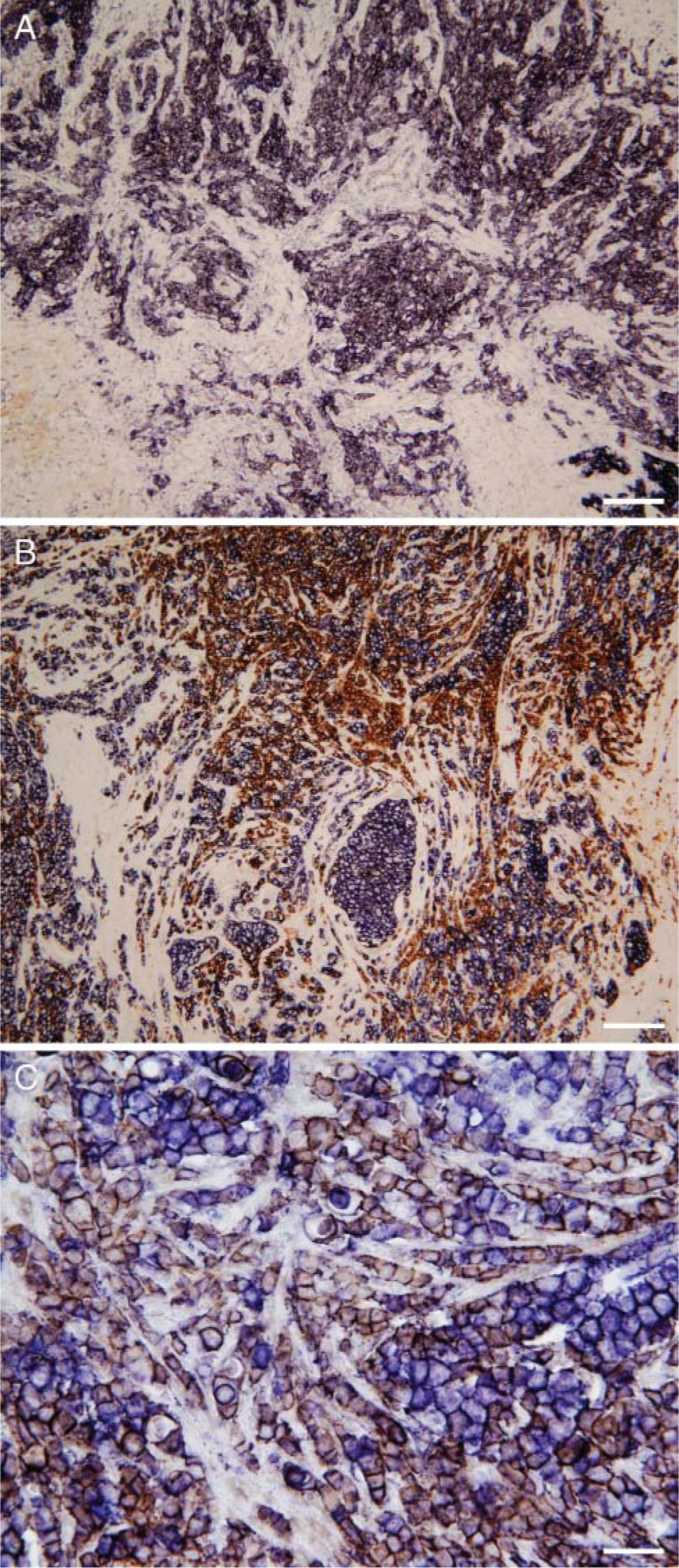
Double staining of a breast cancer case positive for both polyclonal anti-HER-2/
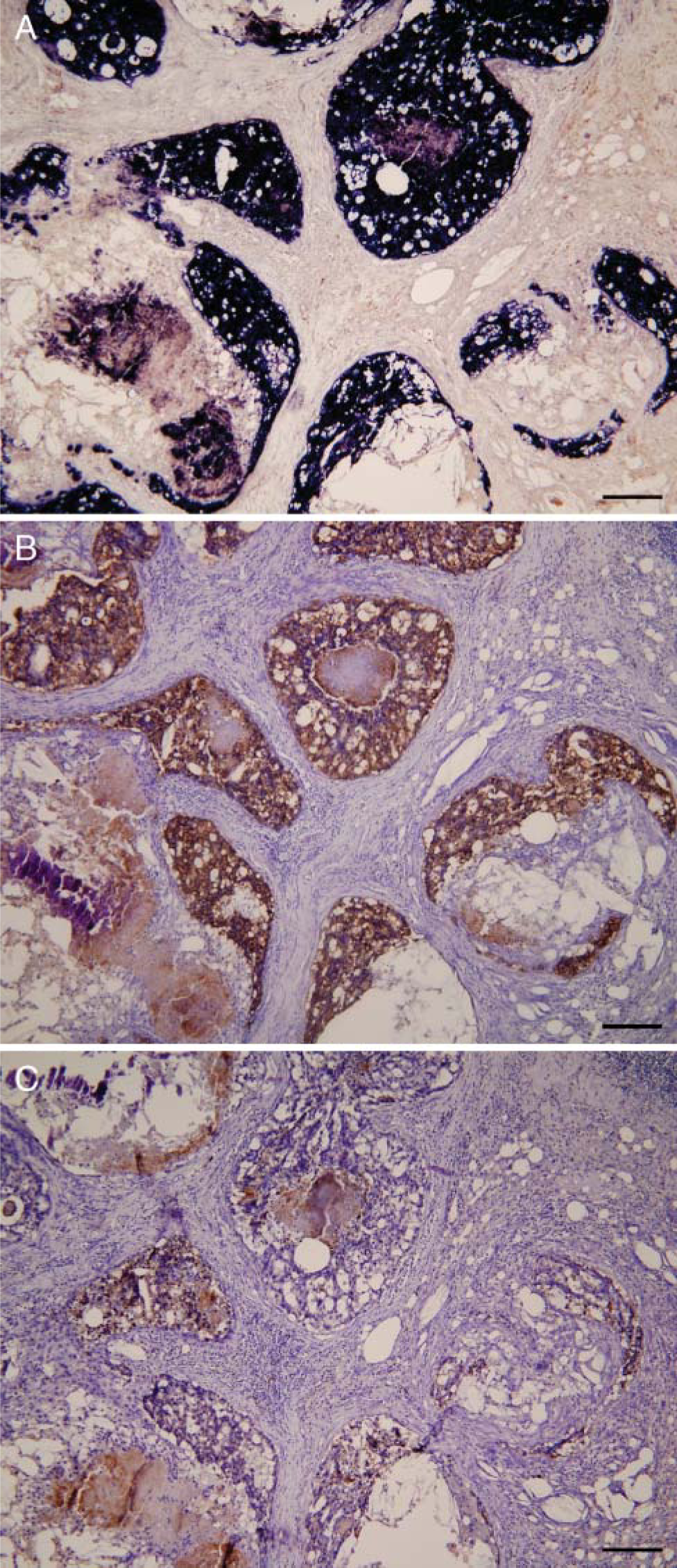
Breast cancer case positive for polyclonal anti-HER-2/
One reason for relatively low specificity and clinical predictability of the IHC tests for selecting candidates for Herceptin (Genentech) therapy is that the antibodies used for diagnosis may recognize different epitopes from that recognized by the drug. False positive results reported with polyclonal anti-HER-2/
We have established a procedure that minimizes nonspecific staining of the humanized therapeutic antibody, trastuzumab, to examine staining of human breast cancer tumors. A similar approach was recently reported using trastuzumab labeled with biotin (Bussolati et al. 2005), which showed good correlation with clinical outcome. However, there are drawbacks to the direct labeling method for routine diagnosis: (1) antibody biotinylation requires expertise that clinical pathology laboratories may not have; (2) it is time-consuming; (3) immunoreactivity was lost at 3 months after biotinylation (Bussolati et al. 2005), affecting reproducibility of the results after minimal storage; (4) biotinylation of primary antibodies can reduce their affinity and specificity to a considerable extent (Dale et al. 1994; Hoyer-Hansen et al. 2000); (5) direct biotinylation of primary antibodies permits only limited amplification of the staining, thereby decreasing sensitivity as compared with use of secondary antibodies. In the present study, use of biotinylated trastuzumab resulted in a high level of cytoplasmic nonspecific binding. The nonspecific binding limited the amount of antibody that could be used so that 2.2% of the cases were scored negative (0 or 1+) with biotinylated trastuzumab, although they were positive (2+ or 3+) using all the other antibodies. Clearly, biotinylation of trastuzumab decreases assay sensitivity. Our results demonstrate that therapeutic antibodies without further modification can be used as diagnostic tools using a standard secondary amplification system to give high sensitivity. The method is applicable with an automated stainer so it could be adapted for use in a clinical pathology laboratory.
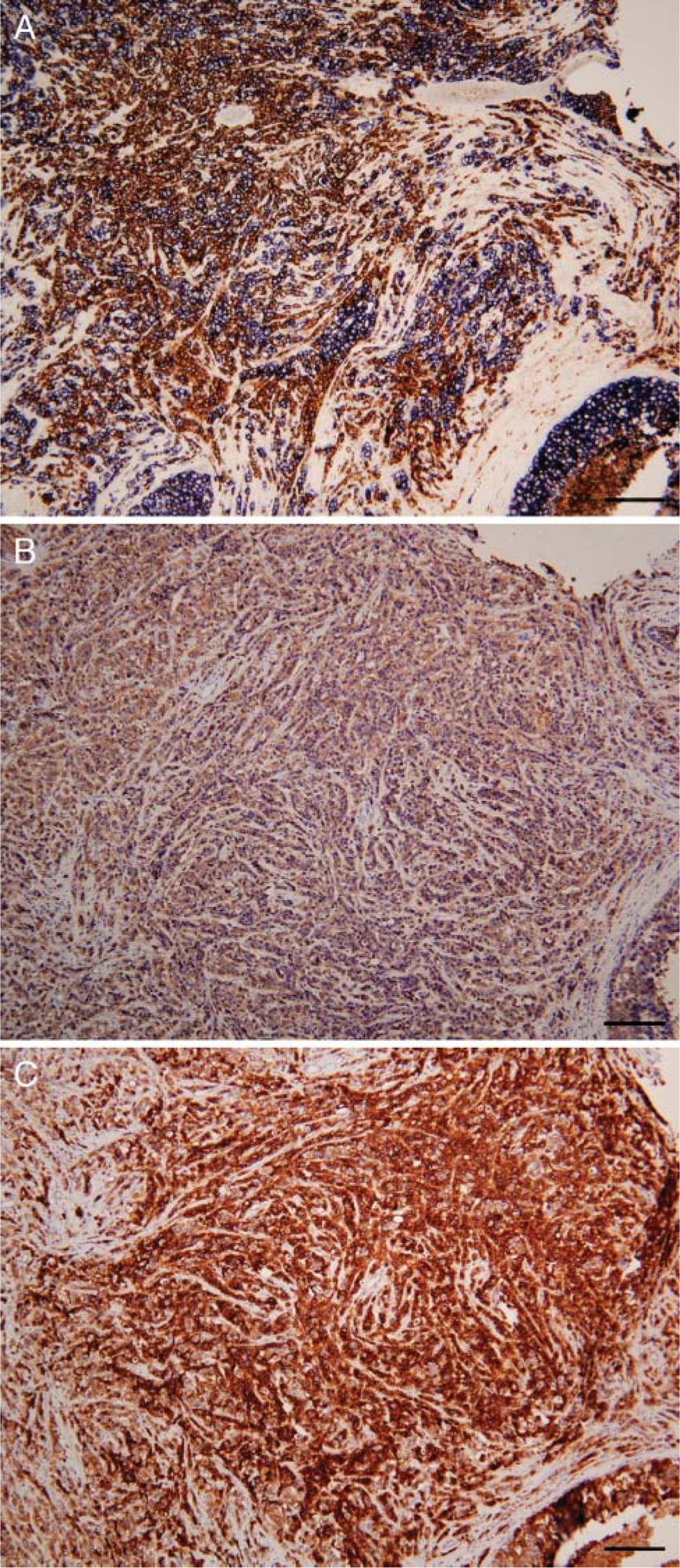
Breast cancer case predominantly positive for trastuzumab. (
We initially tested our method on breast cancer TMAs, which enabled us to screen a large number of cases in a single experiment. TMAs were constructed with triplicate 0.6-mm cores from each case, a strategy shown to provide ∼98% concordance for detection of HER-2/
We have used this method to examine staining of other monoclonal antibodies of human origin (data not shown), demonstrating that the approach could be applied for other human antibody-based therapeutics as well. The applications could be beneficial for the preclinical stage of antibody drug development to examine specificity and cross-reactivity of new antibodies. It also could be used for screening patients in clinical trials. A number of human or ‘humanized’ antibodies have recently entered the market such as cetuximab (Erbitux; ImClone Systems Inc., New York, NY), which targets the epidermal growth factor receptor, or bevacizumab (Avastin; Genentech), which neutralizes the vascular endothelial growth factor (Holbro et al. 2003; Caponigro et al. 2005). The use of polyclonal antibody-based IHC appears to be unsatisfactory for selecting patients for cetuximab therapy (Dei Tos and Ellis 2005). Of relevance to our findings is the observation that patients who had tumors that were negative in this diagnostic IHC test in fact responded to therapy with the therapeutic antibody. Clinical studies will be required to determine if IHC assays using therapeutic antibodies can provide better selection of responsive patients for these drugs.
Footnotes
Acknowledgements
The authors thank Nancy Lemke for her valuable assistance in this work and Dr. Julian Beesley for critical reading of the manuscript.