
Abstract
Coronary microembolization (CME) is associated with progressive myocardial dysfunction despite restoration of coronary flow reserve (CFR). The potential pathophysiological role of mast cells (MCs) remains unclear. Therefore, we induced CME in 18 miniswines and determined whether MC accumulation occurs and their effects on local cytokine secretion [interleukin (IL)-6, IL-8, tumor necrosis factor-α (TNF-α)]; cardiomyocyte apoptosis; and collagen formation at day 1 (D1), day 7 (D7), and day 30 (D30) after CME. Four sham-operated animals without CME (controls) and six animals treated with a MC stabilization agent (tranilast) for 30 days after CME were also studied. CFR decreased at D1 but returned to baseline level at D7 and D30. Coronary sinus levels of IL-6, IL-8, and TNF-α increased significantly at D1 and D7 (p<0.01 vs baseline). Levels of IL-6 and IL-8 at D30 returned to baseline level, but not those of TNF-α. The numbers of total and degranulating MCs, % apoptotic cardiomyocytes, and collagen volume fraction (CVF) over CME myocardium at D1, D7, and D30 were significantly higher than controls (p<0.01). Treatment with tranilast significantly reduced the serum level of TNF-α, numbers of total and degranulating MCs, % apoptotic cardiomyocytes, and CVF at D30 (all p<0.05). There was a significant positive correlation between the numbers of MCs with % apoptotic cardiomyocytes (r = 0.77, p<0.001) and CVF (r = 0.75, p<0.001) over the CME myocardium. Despite restoration of CFR, cardiomyocyte apoptosis persisted after CME and was positively correlated with the number of MCs but was prevented with tranilast treatment. These findings suggest that MCs contribute to cardiomyocyte apoptosis after CME. (J Histochem Cytochem 54:515-523, 2006)
E
Human mast cells (MCs) have been implicated in playing a complex role in inflammatory reaction, neovascularization, and repair process after myocardial injury (Marone et al. 1995; Kennedy et al. 2005). However, the potential roles of MCs in the pathogenesis of CME have not been defined. In this study, an experimental model in swine was used to study whether MC accumulation occurs after CME and their effects on local cytokine secretion and cardiomyocyte apoptosis. Furthermore, the effects of treatment with N(3,4-dimethoxycinnamoyl) anthranilic acid (tranilast), a MC stabilization agent (Nishigaki 1988) used after CME, were also studied.
Materials and Methods
Experimental protocols were approved by the Animal Care and Use Committee of Fudan University, and the study conforms to the Guide for the Care and Use of Laboratory Animals published by the National Institutes of Health, Bethesda, MD.
Experimental Preparation
Twenty eight miniswines of both sexes (20-25 kg body weight) were initially sedated with IM injection of combination ketamine/diazepam (5-10 mg/kg). After endotracheal intubation, anesthesia was maintained by ventilation with 2% isoflurane. Vascular sheaths were placed in the right femoral artery and vein, respectively, by cutdown technique. Prior to coronary cannulation, animals were anticoagulated with 5000 IU heparin bolus IV injection. A 7 Fr Judkins right coronary guide catheter was placed under fluoroscopic guidance via the femoral artery into the left main coronary artery for coronary angiography and monitoring of proximal coronary artery pressure. A 6 Fr Amplatz right diagnostic catheter was advanced via the femoral vein into the coronary sinus for coronary venous blood sampling. Systemic blood pressure and heart rate were continuously monitored during the procedure.
Experimental Protocols
Animals were divided into three groups. Sham-operated miniswines without CME (n=4) served as controls. In a second group of miniswines (n=18), CME was induced by infusion of microspheres into the left anterior descending (LAD) artery. After coronary angiogram, a 2.8 Fr infusion catheter (Cordis Rapidtransit; Johnson and Johnson, Miami, FL) was placed in the LAD artery between the second and third diagonal branches for selective intracoronary infusion of 1.5 × 105 white-stained polystyrene microspheres (45-μm diameter; E-Z Trac, Los Angeles, CA). An incremental dose of microspheres was administered until there was ECG evidence of myocardial ischemia with ST-segment elevation. Lidocaine (100 mg/kg) was given prophylactically to prevent ventricular arrhythmias after CME. In these animals, coronary flow reserve (CFR) assessment and blood sampling for serial measurement of coronary sinus serum levels of IL-6, IL-8, and TNF-α were performed at baseline (n=18) and day 1 (D1) (n=6), day 7 (D7) (n=6), and day 30 (D30) (n=6) after CME. A third group of miniswines (n=6) received tranilast, 10 mg/kg orally twice daily, in gelatin capsules (China Pharmaceutical University; Beijing, China) beginning 2 days before CME and continuing for 30 days until death (Ward et al. 2002). In these animals, CFR assessment and blood sampling for measurement of IL-6, IL-8, and TNF-α were performed at baseline and at D30 after CME. All animals were sacrificed after the repeated CFR assessment for histological examination of MC accumulation and degranulation, apoptosis, and collagen volume fraction (CVF).
Coronary Flow Reserve Assessment
A diagnostic coronary angiogram was performed to visualize the LAD artery. Following intracoronary (IC) administration of 200 μg of nitroglycerin, a 0.014-inch Doppler wire (15 MHz; FloWire, Endosonics, Rancho Cordova, CA) was calibrated, equalized to the guiding catheter, and then advanced to the distal two third portion of the LAD artery to measure CFR before and after CME (Doucette et al. 1992). After acquiring the resting Doppler signal, coronary artery flow hyperemia was induced by IC bolus injection of 18 μg adenosine into the LAD artery through the 2.8 Fr infusion catheter to maximally vasodilate the coronary arterial bed (Figure 1). CFR was calculated as the ratio of hyperemic average peak velocity (hAPV) and baseline average peak velocity (bAPV) (Klauss et al. 1997). Heart rate obtained from the ECG and blood pressure obtained from the guiding catheter were recorded simultaneously during Doppler flow analysis. Variability for repeated measurement of CFR in sham-operated pigs was 5 ± 8%.
Coronary Sinus Levels of IL-6, IL-8, and TNF-α
EDTA-anticoagulated blood samples were collected from the coronary sinus. Immediately after collection, blood samples were centrifuged at 4000 rpm for 15 min, and serum samples were stored at −70C until assay. Serum levels of IL-6, IL-8, and TNF-α were measured with commercially available radioimmunoassay kits according to manufacturer's instructions (Radioimmunology Institute of People's Liberation Army; Beijing, China). All measurements were determined in duplicate. Threshold detection level in serum was 50 pg/ml for IL-6 and 0.1 ng/ml for IL-8 and 0.3 ng/ml for TNF-α.
Postmortem Analysis
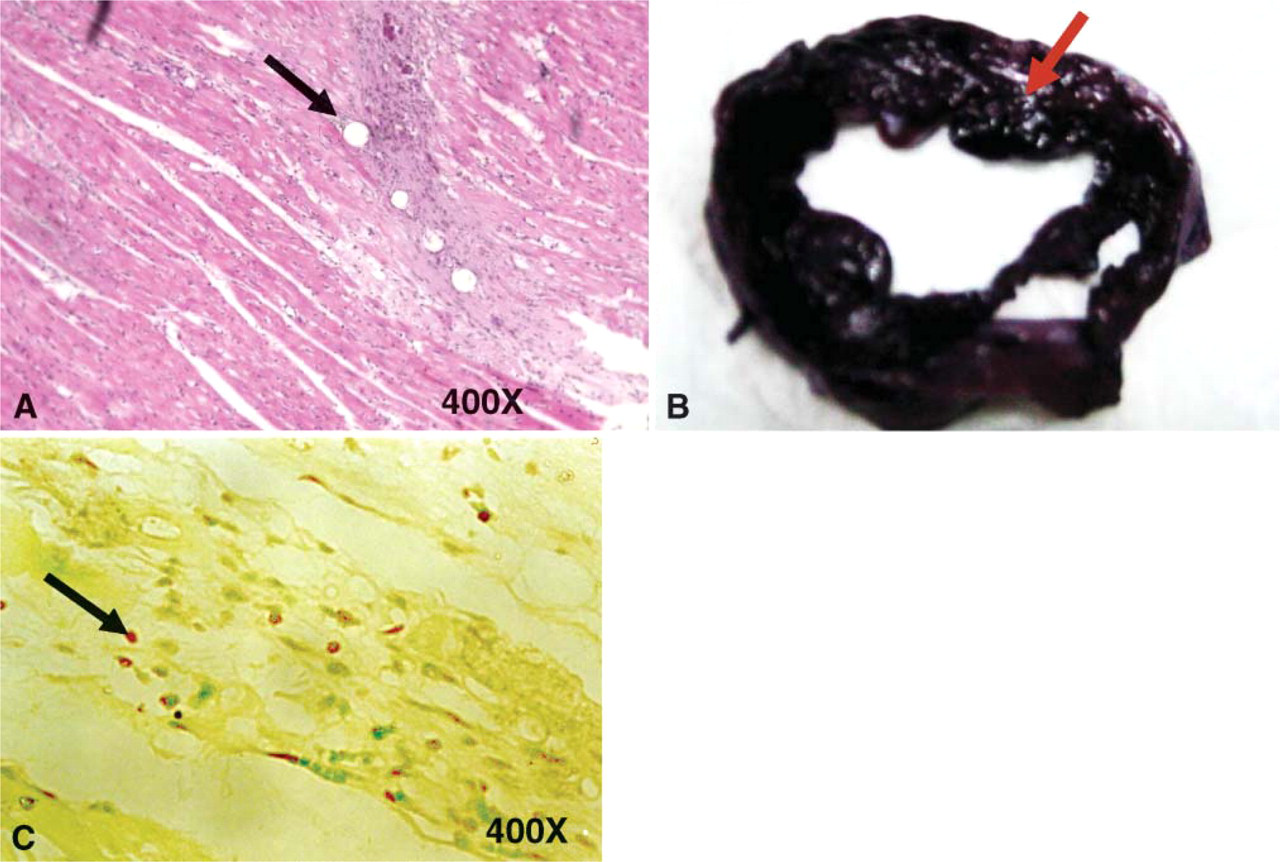
Hearts were excised and sectioned from base to apex into slices for conventional histology, apoptosis analysis, and electron microscopy. Samples were taken from the anterior (LAD territory with CME) and posterior walls [left circumflex (LCX) artery territory as control] of left ventricular myocardium for comparison. Formaldehyde-fixed specimens were embedded in paraffin and sectioned into 5-μm-thick slices. Hematoxylin and eosin staining and nitroblue tetrazolium dye were used to demonstrate the presence of myocardial necrosis after the experimental protocol for CME (Figures 2A and 2B).
Mast Cell Analysis
Light microscopic examination was performed on 5-μm formalin-fixed left ventricular specimens stained with Bismarck brown (Figure 2C). This differential tissue stain has been shown to selectively stain and differentiate MCs (Spatz 1960). The total number of MCs in the Bismarck brown-stained left ventricular section were counted in 40 random high-power fields (HPF) (X400) and expressed as the mean number of MCs per HPF. A detailed microscopic examination for the presence of degranulation in MCs as defined by >50% of the cytoplasmic granules that exhibited fusion and extrusion was counted in 40 random HPFs using X1000 magnification and expressed as the mean number of degranulated MCs per HPF.
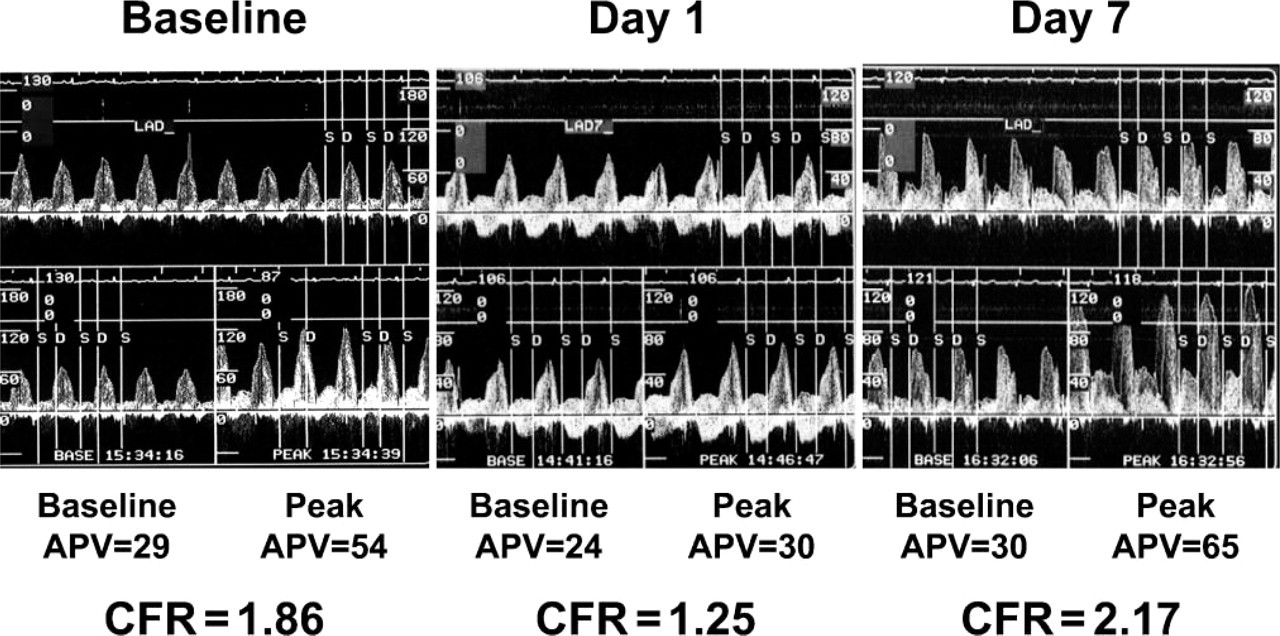
Representative tracings of Doppler flow recording over left anterior descending (LAD) artery in an animal at baseline, at day 1 (D1), and day 7 (D7) after coronary microembolization (CME). Coronary flow reserve (CFR) is calculated as the quotient of hyperemic to baseline average peak velocity (APV). CFR decreased at D1 after CME but restored to baseline level at D7.
Transmission Electron Microscopy
Ultrastructural alternation of MCs was assessed by transmission electron microscopy. Fresh tissue samples were immediately immersed in 2.5% glutaraldehyde and 1% osmium tetroxide, buffered with 3% sodium cacodylate (pH 7.4) at 4C for fixation. Glutaraldehyde-fixed specimens were embedded in resin, and left ventricular sections were viewed and photographed using a Philips CM120 electron microscope (Philips; Eindhoven, The Netherlands) at 60 kV.
Apoptosis Analysis
Myocardial apoptosis was detected using the terminal deoxynucleotidyl transferase-mediated dUTP nick end-labeling (TUNEL) staining using a commercially available kit, according to manufacturer's instructions (Sino-American Biotechnology Co; Beijing, China) (Liu et al. 1995). In each specimen, TUNEL-positive cardiomyocyte nuclei were counted in 40 random HPFs (X400), and the percentage ratio of TUNEL-positive cell nuclei to the total number of cell nuclei was calculated.
Total Collagen Volume Fraction
Five-μm-thick paraffin sections were stained with van Gieson stain for visualization of collagen fiber within the myocardium and examined by light microscopy. Stained sections were analyzed by a Leica DFC 320 digital camera (Leica Microsystems Imaging Solutions Ltd; Cambridge, UK), and CVF was calculated by determining the percentage area of stained tissue within a given field (Dean et al. 2005). A total of 20 random fields were analyzed per sample from the myocardium.
Statistical Analysis
Data are reported as mean ± SD. Serial changes in CFR, serum levels of IL-6 and IL-8, and number of apoptotic cardiomyocytes and MCs were compared by one-way ANOVA followed by Bonferroni t-tests for individual comparisons. Comparisons of the number of apoptotic cardiomyocytes and MCs between the anterior and posterior myocardium were analyzed by Student's t-test. Statistical analysis was performed using SPSS 12.0 (SPSS Inc; Chicago, IL). A p value <0.05 was considered statistically significant.
Results
Coronary Flow Reserve
As determined by Doppler flow wire, CFR decreased from 2.36 ± 0.62 at baseline to 1.72 ± 0.32 at D1 after CME (p=0.03). However, CFR at D7 (2.80 ± 0.68) and D30 (2.27 ± 0.56) increased significantly as compared with D1 (p<0.05) and returned to a level similar to baseline (p>0.05).
Coronary Sinus Levels of IL-6, IL-8, and TNF-α
As shown in Figure 3, the coronary sinus levels of IL-6, IL-8, and TNF-α increased significantly at D1 and D7 after CME as compared with baseline (p<0.01). At D30, both the serum levels of IL-6 and IL-8 returned to baseline level (Figures 4A and 4B, p>0.05). However, the serum level of TNF-α remained significantly elevated at D30 as compared with baseline (Figure 4C, p<0.05).
Mast Cell Analysis
As shown in Figure 4A, the numbers of MCs per HPF over the anterior embolized myocardium progressively increased at D1 (7.8 ± 1.9), D7 (11.5 ± 2.2), and D30 (13.8 ± 2.1) after CME (ANOVA, p<0.01) and were significantly higher than control (3.2 ± 0.4, p<0.01). Furthermore, the numbers of MCs per HPF over the anterior embolized myocardium were also significantly higher than those observed at D1 (3.6 ± 0.6), D7 (3.3 ± 0.6), and D30 (3.3 ± 0.5) over the posterior control myocardium (p<0.01).
As shown in Figure 4B, the numbers of degranulated MCs per HPF over the anterior embolized myocardium progressively increased at D1 (2.6 ± 0.7), D7 (4.7 ± 0.9), and D30 (5.8 ± 1.3) after CME (ANOVA, p<0.001) and were significantly higher than control (0.1 ± 0.02, p<0.001). Furthermore, the numbers of MCs per HPF over the anterior embolized myocardium were also significantly higher than those observed at D1 (0.1 ± 0.03), D7 (0.1 ± 0.02), and D30 (0.1 ± 0.03) over the posterior control myocardium (p<0.001).
Transmission Electron Microscopy
Electron microscopy was used to confirm the presence of MCs as detected by light microscopy and to study their ultrastructure. MCs were frequently found close to vascular structure and at sites with fibroblast and collagen accumulation (Figure 5A). They have a non-segmented nucleus rich in heterochromatin, and their cytoplasm was filled with different secretory granules containing a range of heterogeneous osmiophilic materials (Figure 5B).
Apoptosis Analysis
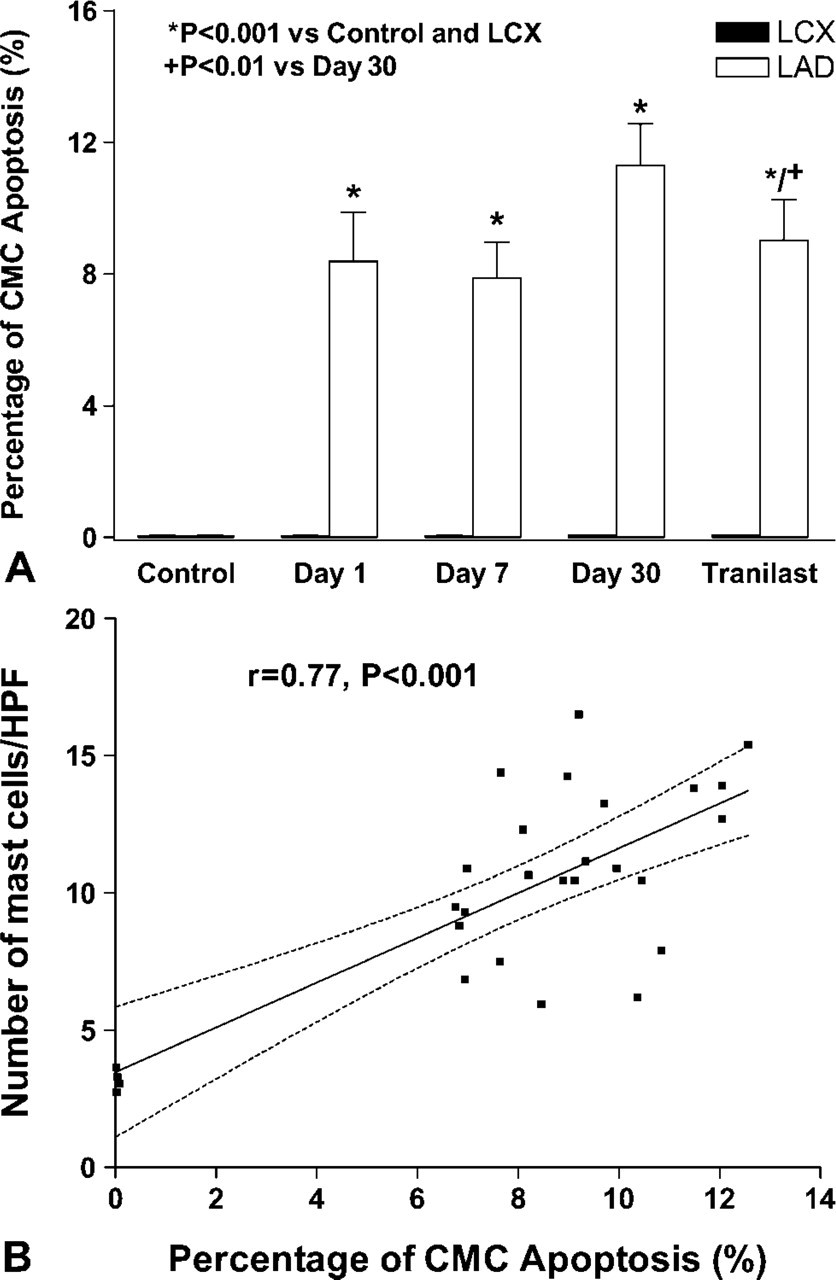
As shown in Figure 6A, TUNEL assay showed that the percentage of apoptotic cardiomyocytes over the anterior embolized myocardium at D1 (8.38 ± 1.49%), D7 (7.87 ± 1.09%), and D30 (11.3 ± 1.25%) after CME were significantly higher than controls (0.09 ± 0.05%, p<0.01). Furthermore, the percentage of apoptotic cardiomyocytes over the anterior embolized myocardium were also significantly higher than those observed at D1 (0.05 ± 0.02%), D7 (0.04 ± 0.03%), and D30 (0.05 ± 0.02%) over the posterior control myocardium (p<0.01).
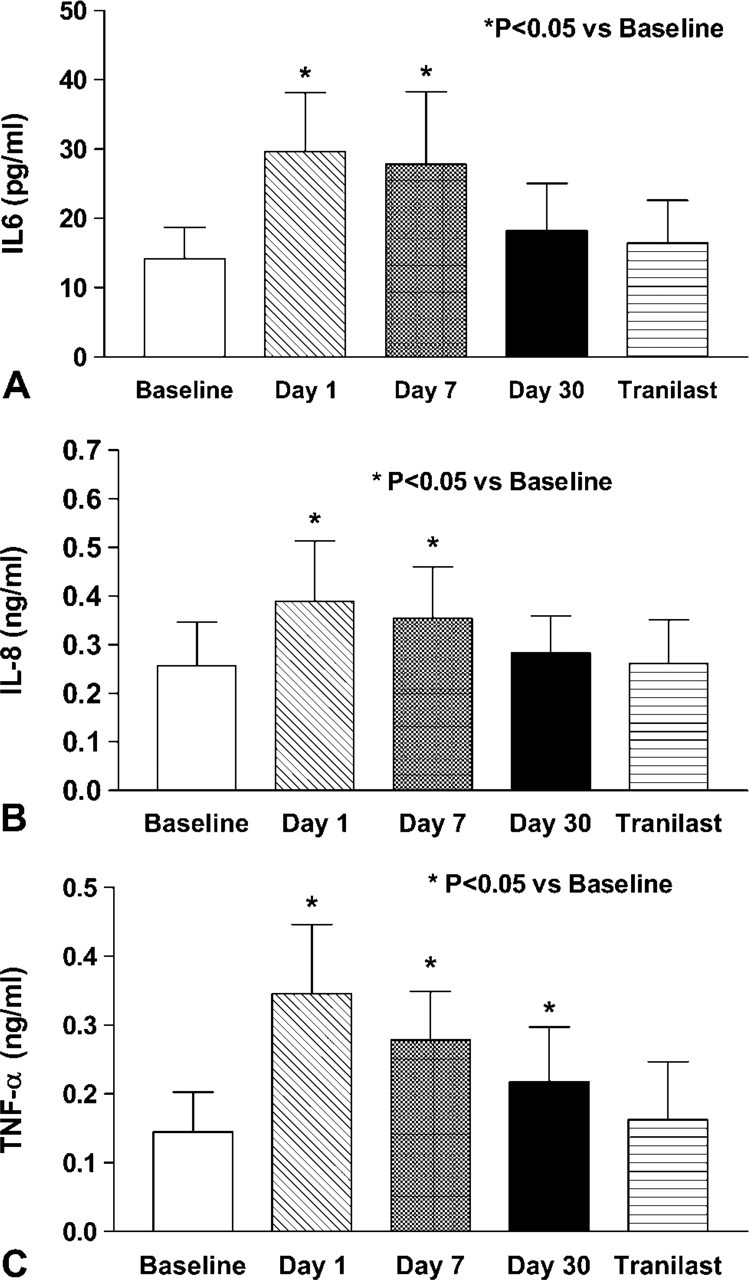
Serial changes in the coronary sinus serum level of (
There was a significant positive correlation between the numbers of MCs and the number of apoptotic cardiomyocytes over the myocardium (r = 0.77, p<0.001, Figure 6B).
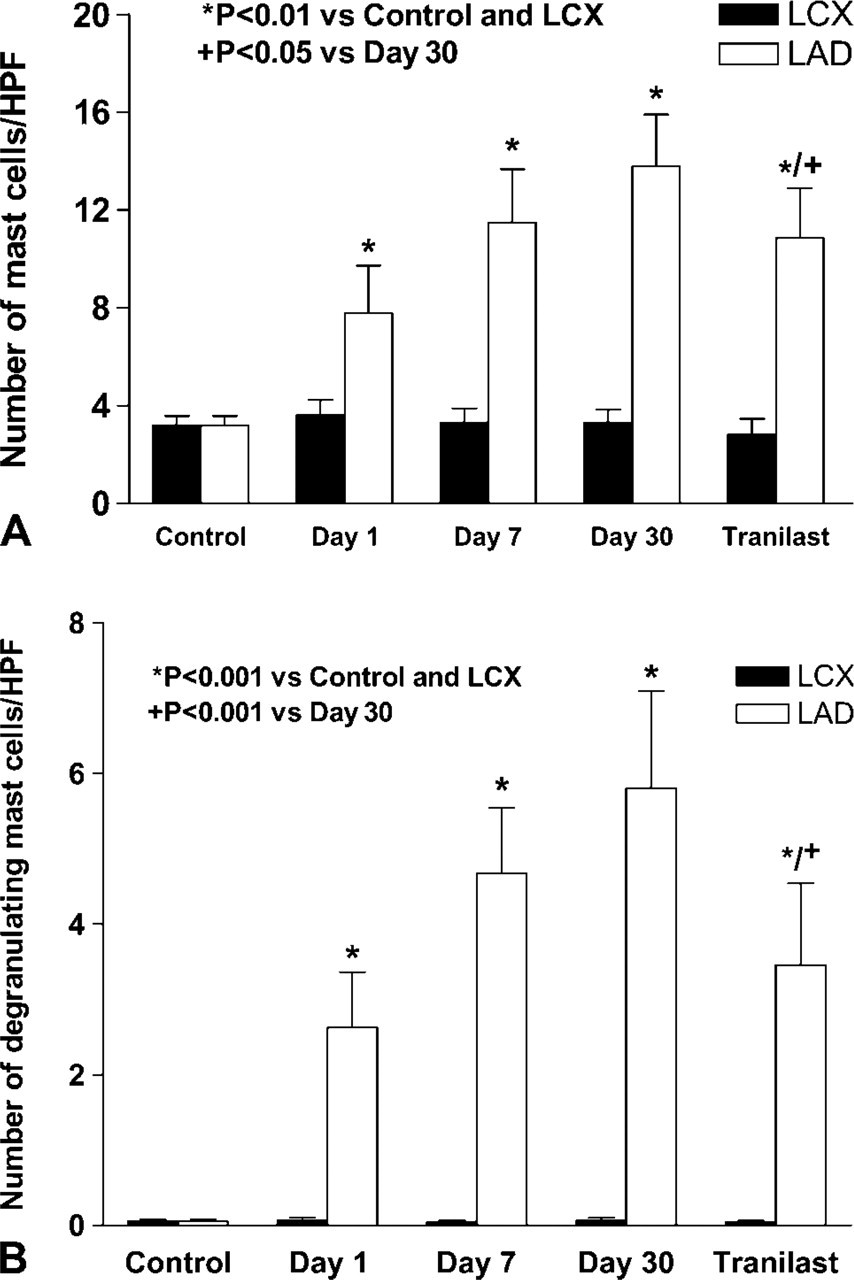
Serial changes in the numbers of (
Collagen Volume Fraction
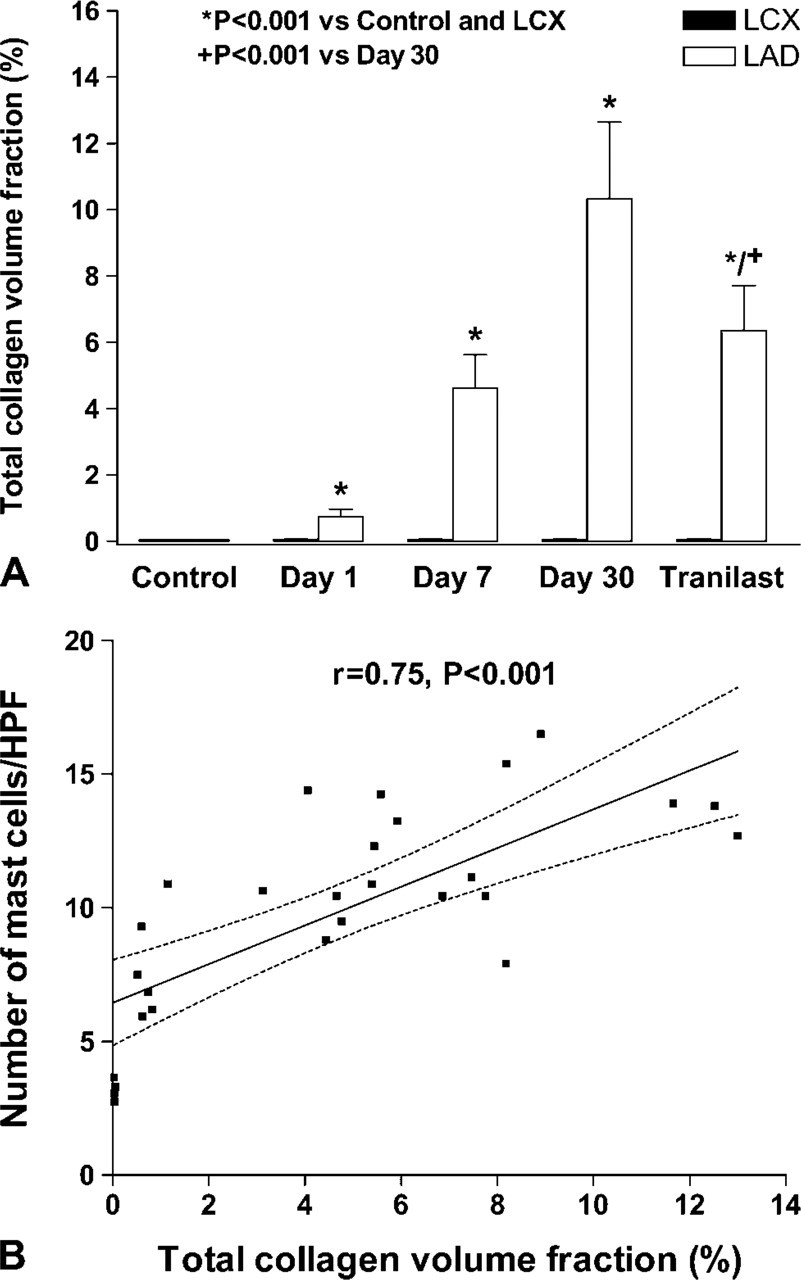
As shown in Figure 7A, the total CVF over the anterior embolized myocardium at D1 (0.8 ± 0.2%), D7 (4.6 ± 1.0%), and D30 (10.3 ± 2.3%) after CME were significantly higher than controls (0.04 ± 0.01%, p<0.001). Furthermore, total CVF over the anterior embolized myocardium was also significantly higher than that observed at D1 (0.1 ± 0.02%), D7 (0.1 ± 0.01%), and D30 (0.1 ± 0.02%) over the posterior control myocardium (p<0.001).
There was a significant positive correlation between the numbers of MCs and the total CVF over the myocardium (r = 0.75, p<0.001, Figure 7B).
Effects of Tranilast
At D30 after CME, there was no significant difference in the CFR (2.26 ± 0.53 vs 2.27 ± 0.56, p=0.8) and coronary sinus levels of IL-6 (Figure 4A, p>0.05) and IL-8 (Figure 4B, p>0.05) between tranilast-treated or untreated animals. However, treatment with tranilast reduced the elevation of coronary sinus level of TNF-α (Figure 4C) and decreased the number of total (10.9 ± 2.0 vs 13.8 ± 2.1, Figure 5A, p<0.05) and degranulated MCs (3.5 ± 1.1 vs 5.8 ± 1.3, Figure 5B, p<0.001) over the anterior embolized myocardium, as compared with those without treatment at D30 after CME. Furthermore, percentage of apoptotic cardiomyocytes (9.0 ± 1.2% vs 11.3 ± 1.3%, Figure 6A, p<0.01) and total CVF (6.3 ± 1.4% vs 10.3 ± 2.3%, Figure 7A, p<0.001) over the anterior embolized myocardium was also significantly reduced at D30 after treatment with tranilast than in untreated animals.
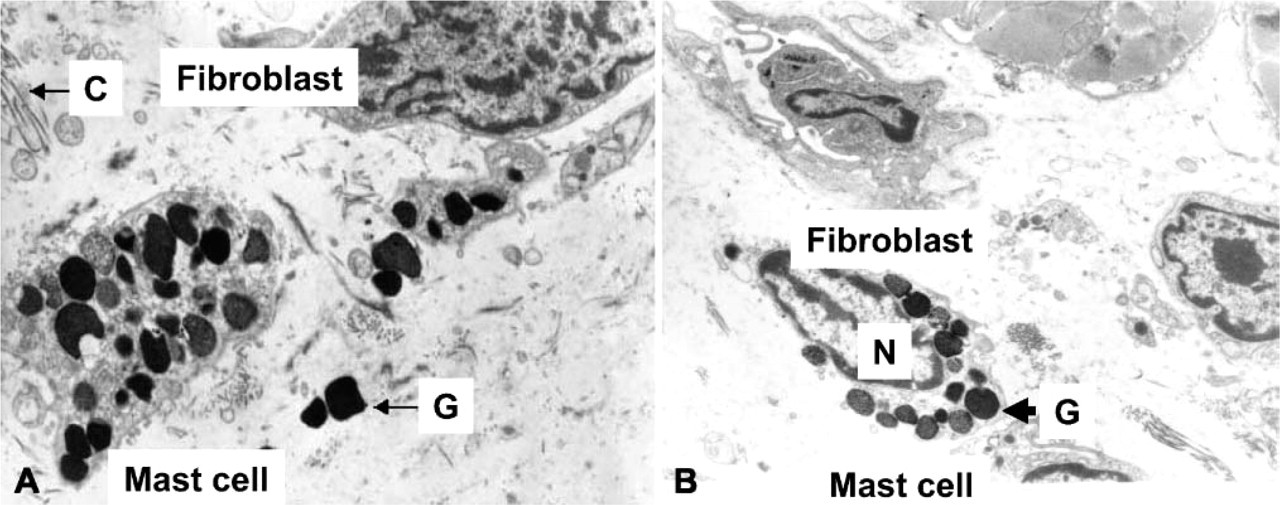
Electron microscopy of the embolized anterior myocardium to show (
Discussion
Using an experimental model of CME, this study provides evidence suggesting that MCs contribute to cardiomyocyte apoptosis in the embolized myocardium after CME. In concordance with previous studies (Dorge et al. 2002; Thielmann et al. 2002; Dispersyn et al. 2002), the present study has demonstrated that progressive cardiomyocyte apoptosis was observed despite early restoration of coronary blood flow. As determined by CFR, coronary blood flow restored to baseline level within 7 days after CME. However, progressive increasing cardiomyocyte apoptosis was observed at embolized myocardium up to 30 days. Early after CME, myocardial levels of cytokines, including IL-6, IL-8, and TNF-α, were elevated. In chronic phase, both the levels of IL-6 and IL-8 returned to baseline values. In contrast, the level of TNF-α was persistently elevated in chronic phase as compared with baseline, but tended to be lower than the acute phase as observed previously (Nossuli et al. 2000). Furthermore, a progressive increasing number of MCs with evidence of degranulation as shown by histological examination in the embolized myocardium was observed in both acute and chronic phase. This accumulation of MCs at the embolized myocardium after CME was significantly correlated with the numbers of cardiomyocyte apoptosis and the amount of collagen deposition. More importantly, treatment with a MC stabilization agent—tranilast—reduced TNF-α levels, decreased the number of total and degranulating MCs, and prevented cardiomyocyte apoptosis and collagen deposition after CME. These findings provide evidence to suggest that MCs directly or indirectly contribute to cardiomyocyte apoptosis and collagen deposition after CME.
Recently, the clinical importance of CME in patients with acute coronary syndromes or those receiving percutaneous coronary intervention has been increasingly appreciated. It has been identified as a potential cause of malignant arrhythmia, contractile dysfunction, and myocardial infarction (Folts et al. 1999; Erbel et al. 2000; Topol et al. 2000). Prior experimental studies have shown that CME induced myocardial contractile dysfunction and is associated with leukocyte infiltration, increased TNF-α expression, and myocardial apoptosis (Dorge et al. 2000,2002; Jiang et al. 2003). Furthermore, TNF-α and sphingosine play a causal role in the development of myocardial contractile dysfunction after CME (Dorge et al. 2002; Thielmann et al. 2002). After ischemic injury, inflammatory cytokines such as IL6, IL-8, and TNF-α may play an important role in the initial inflammatory injury as well as regulating cardiomyocyte apoptosis and cardiac repair (Nian et al. 2004). After ischemic injury, TNF-α induces gene expression of IL-6 and IL-8, suggesting that TNF-α plays a major role as an upstream cytokine inducer (Gwechenberger et al. 1999; Yoshida et al. 2004). As shown in this study, myocardial levels of IL-6, IL-8, and TNF-α increased at D1 and D7 after CME. However, only TNF-α level was persistently elevated at D30. Recent studies (Zhao et al. 2005) suggested that proteases secreted from the activated MCs can degrade the endogenous cytokines, in which IL-6 was more susceptible than TNF-α. This may provide an explanation for the normal level of downstream cytokine IL-6 and IL-8 detected, even though in the chronic phase the upstream TNF-α was persistently elevated, but with a lower level of TNF-α. Furthermore, this can also lead to underestimation of the local production of these cytokines by MCs in this study as only their serum levels were measured.
Human MCs have been identified in the myocardium even under normal physiological conditions, with their distribution along the coronary arterioles (Rakusan et al. 1990). Many MC mediators such as IL-1, IL-6, IL-8, TNF-α, and vascular endothelial growth factor are preformed and stored in large amounts in secretory granules for immediate release after myocardial injury (Marone et al. 2000). During ischemia-reperfusion injury, MCs may play a role in acute tissue damage and cardiac dysfunction by releasing TNF-α (Frangogiannis et al. 1998; Gilles et al. 2003). Furthermore, MC density is increased in the hearts of patients with ischemic and idiopathic dilated cardiomyopathy (Patella et al. 1998) and may contribute to the disease process through the release of mediators (Yokoyama et al. 1993) and cause apoptosis of cardiomyocytes (Hara et al. 1999).
The present study has demonstrated that MCs may also play an important role in the pathogenesis of cardiomyocyte apoptosis after CME. As shown by histological and electron microscopy studies, MCs accumulated in the embolized myocardium after CME. The number of MCs observed in the embolized myocardium correlated with the severity of cardiomyocyte apoptosis and collagen deposition. By releasing the cytokines from their secretory granules, MCs have the capacity to coordinate trafficking of leukocytes into the embolized myocardium. Furthermore, secretion of TNF-α from MCs can also directly lead to cardiomyocyte apoptosis. Accordingly, a selective therapeutic agent to prevent MC degranulation was further studied. Indeed, treatment with tranilast reduced accumulation and degranulation of MCs, decreased the level of TNF-α, and prevented cardiomyocyte apoptosis and collagen deposition. However, whether this type of treatment can provide a similar clinical benefit after CME in humans deserves further investigation.
Limitations
Although light microscopy and transmission electron microscopy were used to detect the presence of total and degranulated MCs in the embolized myocardium, no detailed characterization of the content of their granules was performed in this study. Furthermore, measurement of the serum levels of IL-6, IL-8, and TNF-α rather than their tissue levels was performed. This may lead to underestimation of the amount of cytokines secreted from MCs as discussed previously, and the cellular source of these cytokines remains unknown. However, findings from this study did demonstrate that MCs are a source of TNF-α as suppression of degranulation of MCs by tranilast and reduced serum levels of TNF-α after CME. Finally, whether accumulation of MCs in the embolized myocardium is caused by proliferation and maturation of residual immature MCs or migration of MCs from other sites is not clear.