
Abstract
This study shows that artificial super antiapoptotic FNK protein fused with a protein transduction domain (PTD-FNK) maintains the quality of osteochondral transplant by preventing chondrocyte death. Cylindrical osteochondral grafts were obtained from enhanced green fluorescent protein (EGFP)-expressing transgenic rats, in which living chondrocytes express green fluorescence, and submerged into medium containing PTD-FNK, followed by transplantation into cartilage defects of wild-type rats by impact insertion simulating autologous transplantation. The tissues were histologically evaluated by hematoxylineosin and Safranin-O staining. At 1 week, chondrocyte alignment was normal in the PTD-FNK treatment group, whereas all grafts without PTD-FNK treatment showed mixed cluster cell distribution. At 4 weeks, all grafts with PTD-FNK treatment showed almost normal matrix, whereas two grafts without PTD-FNK treatment showed fibrocartilage. Notably, all grafts with PTD-FNK retained high intensity of Safranin-O staining, but all grafts without PTD-FNK largely lost Safranin-O staining. PTD-FNK significantly suppressed a decrease in the survival rate and the density of EGFP-positive cells at 1 and 2 weeks, and this tendency continued at 4 weeks. The results of terminal deoxynucleotidyl transferase (TdT)-mediated deoxyuridine triphosphate (dUTP)-nick end-labeling staining showed that PTD-FNK inhibited cell death, indicating that PTD-FNK protects chondrocyte death and suppresses graft degeneration.
Keywords
O
Several studies suggest that mechanical stress during graft preparation causes cell death, including apoptosis, at an early stage after transplantation, obstructing the regeneration of hyaline cartilage. When articular cartilage was experimentally wounded, cell death was induced in a more extensive region than the lesion edge (Tew et al. 2000). Evaluation of early cell death at the edges of osteochondral grafts suggests that mosaicplasty is associated with an extensive margin of cell death that is likely to compromise lateral integration and articular reconstruction (Huntley et al. 2005). In addition, impact insertion of osteochondral grafts generates damaging loads that cause necrotic and apoptotic death of chondrocytes (Huntley et al. 2005; Borazjani et al. 2006); the apoptotic events after impact loading of osteochondral grafts have also been shown using human fresh cadavers (D'Lima et al. 2001; Patil et al. 2008) and animal models (Chen et al. 2001; Whiteside et al. 2005). Incomplete healing of the hyaline cartilage of osteochondral grafts has been shown in animal models in vivo, although the degree of degeneration varied among experiments (Makino et al. 2001; Oshima et al. 2002; Hui et al. 2004; Nam et al. 2004; Tibesku et al. 2004; Harman et al. 2006; Kleemann et al. 2007). Persistent interface between the transplant and the surrounding host cartilage in 2 years of clinical trials has also been shown, although their hyaline character was retained to some degree (Horas et al. 2003). The regeneration of hyaline cartilage would begin after the cylindrical osteochondral autograft transplantation even when any other strategies were combined. Therefore, preventing cell death is critical in the therapeutic strategy after osteochondral transplantation.
Visual histological assessment of cartilage repair
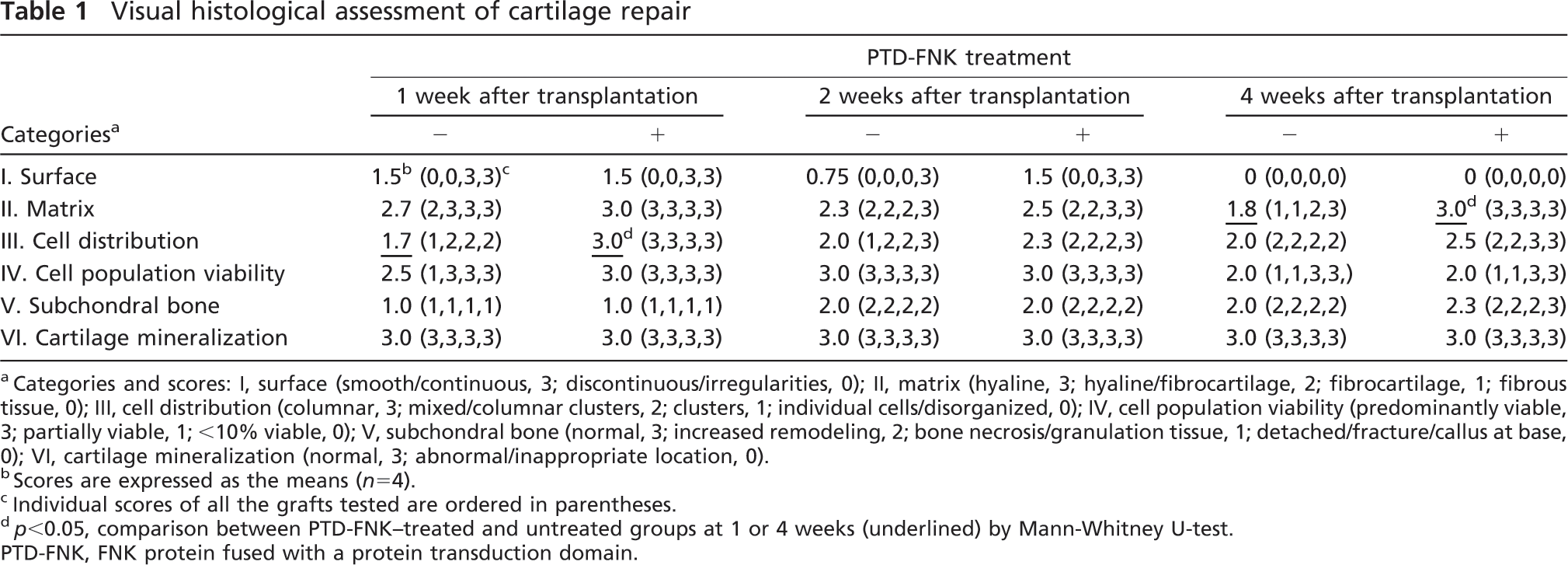
Categories and scores: I, surface (smooth/continuous, 3; discontinuous/irregularities, 0); II, matrix (hyaline, 3; hyaline/fibrocartilage, 2; fibrocartilage, 1; fibrous tissue, 0); III, cell distribution (columnar, 3; mixed/columnar clusters, 2; clusters, 1; individual cells/disorganized, 0); IV, cell population viability (predominantly viable, 3; partially viable, 1; <10% viable, 0); V, subchondral bone (normal, 3; increased remodeling, 2; bone necrosis/granulation tissue, 1; detached/fracture/callus at base, 0); VI, cartilage mineralization (normal, 3; abnormal/inappropriate location, 0).
Scores are expressed as the means (n = 4).
Individual scores of all the grafts tested are ordered in parentheses.
p<0.05, comparison between PTD-FNK-treated and untreated groups at 1 or 4 weeks (underlined) by Mann-Whitney U-test.
PTD-FNK, FNK protein fused with a protein transduction domain.
We engineered the antiapoptotic bcl-x gene to generate the super antiapoptotic factor, FNK, by substituting three amino acid residues, Tyr-22 to Phe(F), Gln-26 to Asn(N), and Arg-165 to Lys(K), in which three hydrogen bonds stabilizing the central α5-α6 helices are abolished. This novel protein exhibits stronger cyto-protective activity than Bcl-xL against various death stimuli, including oxidative stress, calcium ionophore, serum withdrawal, and anti-Fas (Asoh et al. 2000). FNK was fused with the protein transduction domain (PTD) of the HIV/Tat protein to rapidly enter the cytoplasm through cell membrane. We have shown that PTD-FNK successfully protected cells from cell death induced by a number of pathological conditions, using experimental pathological models of ischemic injury to the brain (Asoh et al. 2002; Katsura et al. 2008), heart (Arakawa et al. 2007), and liver (Nagai et al. 2007), carbon tetrachloride-induced liver injury (Asoh et al. 2005), lipopolysaccharide-induced acute lung injury (Chen et al. 2007), aminoglycoside ototoxicity (Kashio et al. 2007), amyotrophic lateral sclerosis (Ohta et al. 2008), chemotherapy-induced alopecia (Nakashima-Kamimura et al. 2007), and in bone marrow grafts (Tara et al. 2007). Our previous study using sliced cartilage showed that PTD-FNK penetrates the cartilage to enter chondrocytes and protect the cells from anti-Fas and nitrogen oxide-induced cell death (Ozaki et al. 2004) and from freezing/thawing-induced death (Sudo et al. 2005). In this study, we hypothesized that PTD-FNK protein would suppress the degeneration of cylindrical osteochondral autograft by inhibiting cell death occurring at an early stage after transplantation. We used a transplantation model between enhanced green fluorescent protein (EGFP)-expressing transgenic rats and wild-type rats to simulate autologous transplantation. Osteochondral grafts, which were harvested from EGFP rats and submerged in medium containing PTD-FNK, were transplanted into cartilage defects of wild-type rats. The objective of this study was to investigate whether PTD-FNK protein maintains the quality of osteochondral transplant by protecting graft cells from cell death.
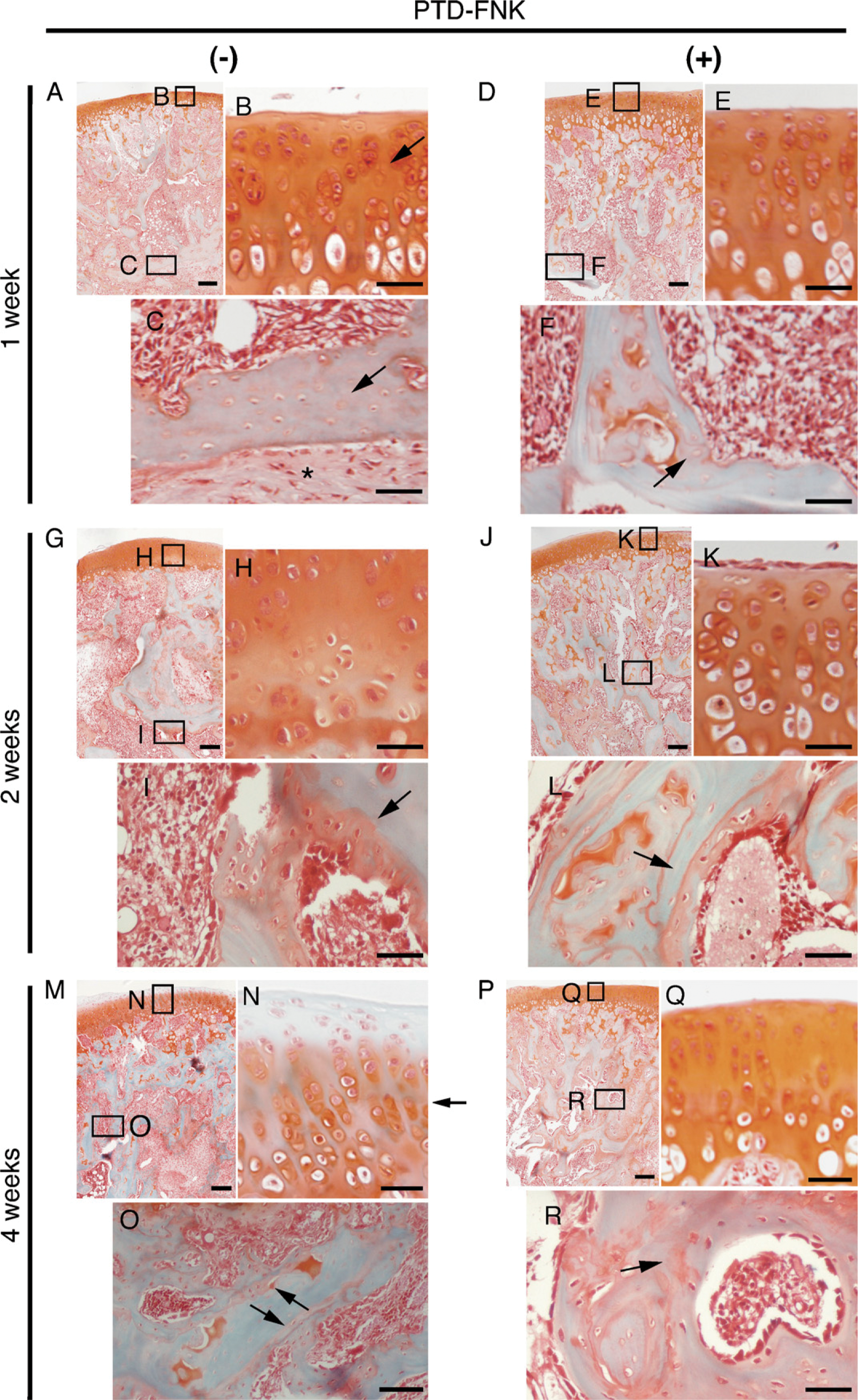
Sections of osteochondral graft stained with Safranin O/Fast Green without FNK protein fused with a protein transduction domain (PTD-FNK) treatment at 1 (
Materials and Methods
Preparation of PTD-FNK
The PTD-FNK gene encodes met-gly-PTD (consisting of 11 amino acids: YGRKKRRQRRR)-gly-FNK, as described previously (Asoh et al. 2002). PTD-FNK protein was prepared as described previously (Asoh et al. 2002; Ozaki et al. 2004). The PTD-FNK-expressing plasmid was introduced into Escherichia coli cells, and PTD-FNK protein was overproduced by treatment with 1 mM of isopropyl 1-thio-β-D-galactoside (IPTG) for 5 hr with vigorous shaking at 37C. Transformants were harvested by centrifugation, suspended with Buffer A (50 mM Tris-HCl, pH 8.0, 150 mM NaCl, 1 mM EDTA, and 1 mM DTT), and sonicated to disrupt the cells. After centrifugation at 12,000 X g for 30 min, the pellet, including inclusion bodies, was resuspended in Buffer A, sonicated again, and added to 1% Triton X-100. After centrifugation to precipitate inclusion bodies, the pellet was dissolved in Buffer B (50 mM Tris-HCl, pH 6.8, 2% SDS, 7 M urea, and 1 mM DTT). After centrifugation at 12,000 × g for 30 min, the supernatant contained the majority of PTD-FNK protein. The supernatant was subjected to SDS/PAGE to remove endotoxin and contaminated proteins. The gel was briefly immersed in 1 M K Cl, which makes an insoluble complex with free SDS, and a band corresponding to PTD-FNK (transparent because of reduced free SDS) was cut out. PTD-FNK was electrophoretically extracted from the gel slice in extraction buffer (25 mM Tris/0.2 M glycine/0.1% SDS) and was used for experiments. The extraction buffer was used as a control (vehicle). The concentration of extracted PTD-FNK ranged from 1 to 2 mg/ml. Protein concentration was determined by Coomassie brilliant blue staining after SDS/PAGE, followed by comparison with BSA standard.
PTD-FNK Treatment of Osteochondral Grafts and Transplantation
Animals were anesthetized with Nembutal (Dainippon Sumitomo Pharma; Osaka, Japan) during surgery. Male Sprague-Dawley-Tg (CAG-EGFP) rats (8 weeks old; Japan SLC, Hamamatsu, Shizuoka, Japan) were used as graft donors. An anterior midline incision was made through the skin of the knee joint, and the articular surface of the femur was exposed using a medial parapatellar retinacular approach. Cylindrical osteochondral grafts were harvested using a cylindrical chisel (Mosaic Plasty DP System, 2.7 mm in diameter; Smith and Nephew, Grand Island, MA) from the medial femoral condyle of the rats. The grafts were immersed for 3 hr in DMEM/F-12 medium (Invitrogen; Andover, NY) lacking FCS in the presence or absence (vehicle, 1:1000 dilution) of PTD-FNK (33 nM, 1:1000 dilution). Meanwhile, a cylindrical defect (2.7 mm in diameter) as a recipient site was prepared in the medial femoral condyle of wild-type male Sprague-Dawley rats (8 weeks old, n = 4 each experimental group; Japan SLC). The grafts were transplanted to the recipient site and inserted using a tamp to make their cartilage flush with that of the surrounding host cartilage. During the procedure, only a medial collateral ligament was cut. After the medial retinaculum was sutured, the host rats were returned to their cages under a 12-hr light-dark cycle, with ad libitum access to food and water. No infections or complications were observed during the study. Animal protocols were approved by the Animal Care and Use Committee of Nippon Medical School.
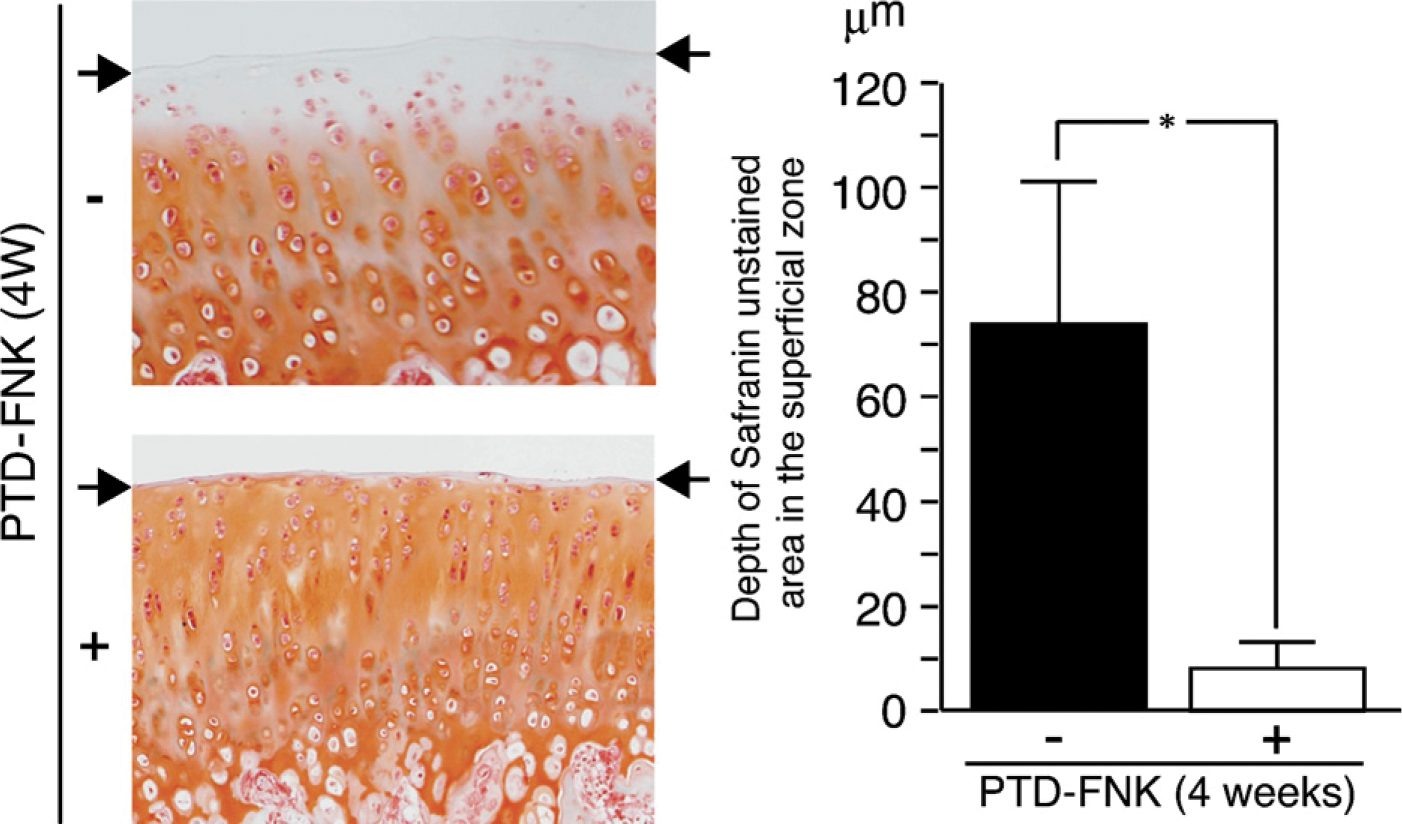
Cartilage layer of the graft without PTD-FNK treatment lost Safranin staining in the superficial zone at 4 weeks (top left). Matrix of the graft with PTD-FNK treatment was maintained (bottom left). Analysis with NIH Image Software showed that the superficial zone losing staining in the PTD-FNK untreated group was ∼10 times thicker than that in the PTD-FNK treatment group (right). ∗ p<0.005 vs PTD-FNK non-treatment groups at 4 weeks by Student's t-test. Arrow, cartilage surface.
Preparation of Paraffin Sections and Histochemical Staining
Rats were sacrificed 1, 2, or 4 weeks after transplantation. The graft-received femoral condyle, including tight bone, was removed and fixed in 4% paraformal-dehyde in 0.1 M PBS (pH 7.4) at 4C for 48 hr, followed by decalcifying with EDTA (0.5 M, pH 8.0) for 3 weeks. Tissue samples were sagittally cut and embedded in paraffin (with 24-hr processing). Sections (5 μm thickness) were made for histochemical staining [hematoxylin-eosin (HE) staining or Safranin-O/Fast Green staining] and terminal deoxynucleotidyl transferase (TdT)-mediated deoxyuridine triphosphate (dUTP)-nick end-labeling (TUNEL) staining. For Safranin-O/Fast Green staining, sections were stained with 0.1% Safranin O (Sigma Life Science; Tokyo, Japan), followed by counterstaining with Fast Green (Sigma Life Science). To evaluate cell death, TUNEL staining was performed according to the manufacturer's protocol using an ApopTag Kit (Chemicon International; Temecula, CA) coupled with the diaminobenzidine reaction. Controls for the specificity of the signal included omission of TdT reagent.
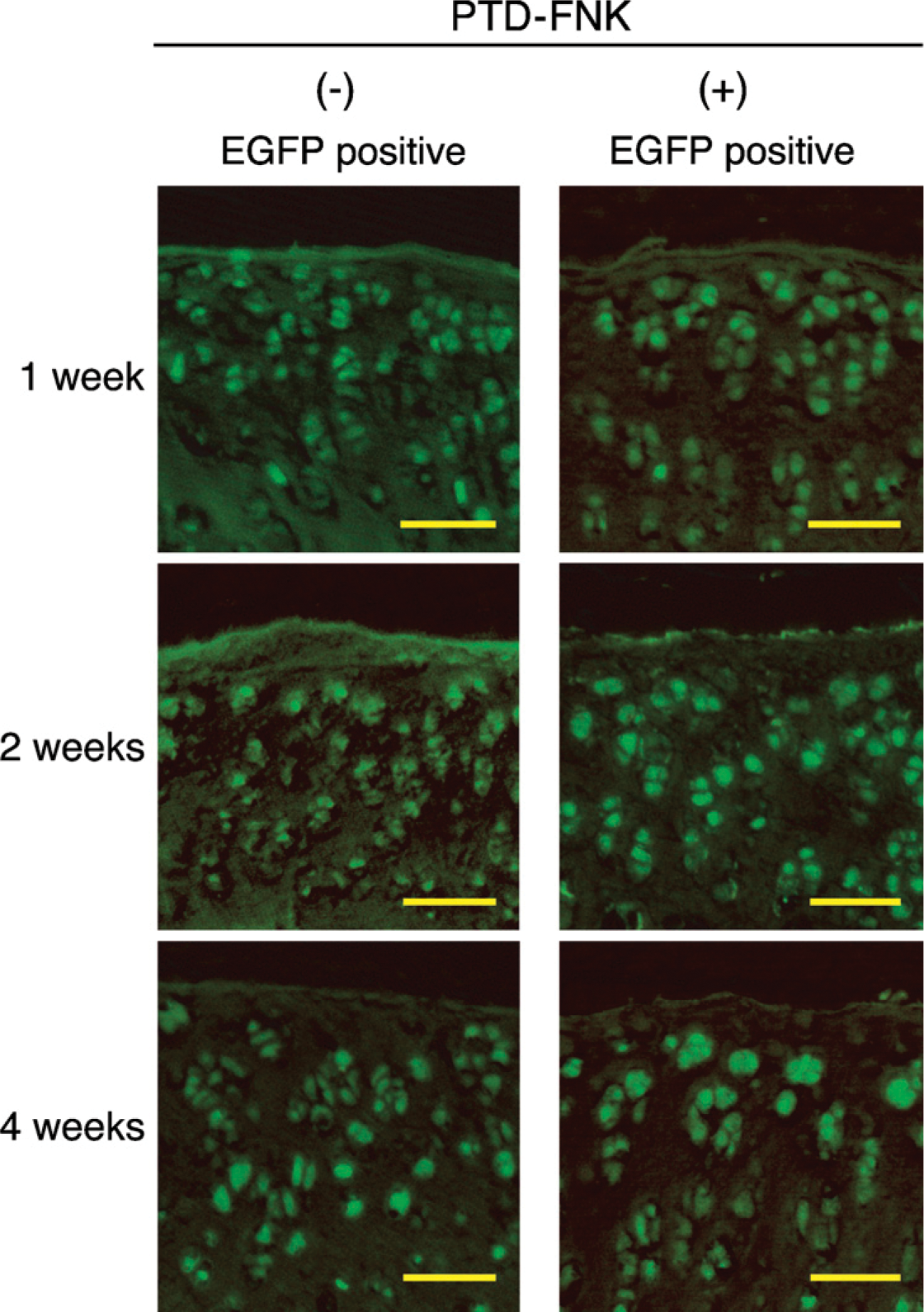
Enhanced green fluorescent protein (EGFP)-positive surviving cells in the cartilage layer of graft were counted. Surviving chondrocytes expressed EGFP during the study period. Bar = 50 μm.
Histological Assessment of Cartilage Repair
According to the International Cartilage Repair Society (ICRS) (Mainil-Varlet et al. 2003), microscopic findings were evaluated by two examiners in a blind manner, using HE- and Safranin-O-stained sections. ICRS proposed six categories with individual scores, which are described in the legend of Table 1.
Statistical Analysis
All analyses were performed using Student's t-test or the Mann-Whitney U-test, as indicated in the figure and table legends (StatView J-5.0; SAS Institute, Cary, NC). Data are presented as the means ± SE. Differences were considered significant when p<0.05.
Results
Microscopic Evaluation of Cartilage Repair
We transplanted osteochondral grafts obtained from EGFP-expressing rats into the cartilage of wild-type rats. At 1, 2, or 4 weeks after transplantation, no apparent macroscopic difference was observed between PTD-FNK treatment and non-treatment groups; however, HE and Safranin-O/Fast Green staining showed microscopic differences between them, as mentioned below.
At 1 week, a significant difference appeared in cell distribution (Table 1). All graft cartilage without PTD-FNK treatment showed abnormal cell distribution, that is, a mixed pattern of columnar arrangement and cluster of chondrocytes (Figures 1A and 1B; Table 1). On the other hand, chondrocytes were arranged in a columnar pattern in the PTD-FNK treatment group (Figures 1D and 1E; Table 1). In both groups, we observed slightly irregular surfaces (Figures 1A and 1D; Table 1) and necrosis in the subchondral bone to the same extent (Figures 1C and 1F; Table 1). The other features were almost normal, although one graft without PTD-FNK treatment showed low cell population viability (Figure 1B; Table 1) and low-level Safranin-O staining (matrix) (Table 1).
At 2 weeks, grafts with PTD-FNK treatment seemed to be slightly better than grafts without PTD-FNK treatment with regard to cartilage surface and cell distribution (Figures 1G and 1H; Table 1). It is noted that one graft without PTD-FNK treatment formed chondrocyte clusters (Figure 1H; Table 1). We also observed increased remodeling of subchondral bone in both groups (Figures 1I and 1L; Table 1).
At 4 weeks, cartilage surfaces of both groups were slightly irregular; however, there was another significant difference in the matrix between the two groups (Table 1). All graft cartilage with PTD-FNK treatment showed almost normal matrix (Figure 1Q), whereas the cartilage of two grafts (50%) without PTD-FNK treatment was found to be fibrocartilage, which developed just above the tidemark (Figure 1N). In addition, PTD-FNK treatment seemed to suppress deterioration of cell distribution but not to increase cell population viability (Table 1). There was no difference in the subchondral bone and cartilage mineralization of either group (Figures 1O and 1R; Table 1).
Microscopic assessment strongly suggested that PTD-FNK suppresses a matrix deterioration and disruption of columnar chondrocyte distribution during the study period.
Safranin-O/Fast Green Staining
Safranin-O stoichiometrically binds to tissue glycosaminoglycan, such as chondroitin sulfate and keratan sulfate (Rosenberg 1971), and is widely used to evaluate the amount of proteoglycan present in cartilage (Mainil-Varlet et al. 2003). Safranin-O/Fast Green staining allowed us to be aware of another important finding. Grafted cartilage exhibited high-level Safranin-O staining at 1 and 2 weeks in both groups (Figures 1B, 1E, and 1K). At 4 weeks, no great difference in the intensity of Safranin-O staining was observed between the graft and host cartilages; however, all cartilage layers of grafts with PTD-FNK treatment remained Safranin-O staining positive through almost the entire thickness (Figure 2). In contrast, the cartilage layers of grafts without PTD-FNK treatment showed a significant reduction of Safranin-O staining in the superficial zone, indicating that some chondrocytes, but not all, lost their activity to synthesize glycosaminoglycan. Analysis with NIH Image Soft ware showed that the superficial zone losing Safranin-O staining in the PTD-FNK untreated group was ∼10 times thicker than that in the PTD-FNK treatment group (Figure 2). PTD-FNK clearly suppressed the loss of Safranin-O staining for 4 weeks, indicating that PTD-FNK preserves chondrocytes from losing cellular activity to maintain normal proteoglycan for at least for 4 weeks.
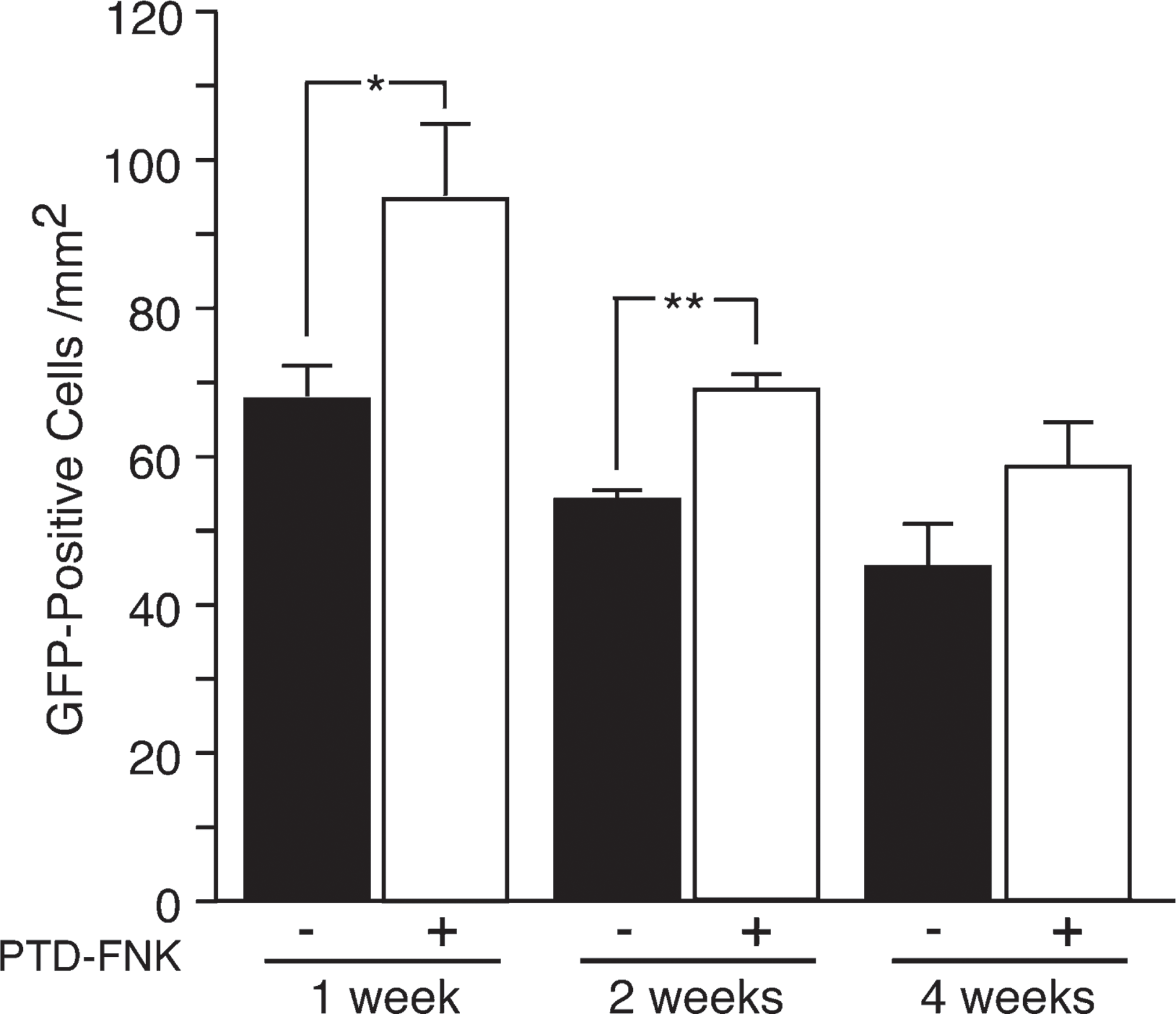
A number of EGFP-positive cells were normalized against the area of the cartilage layer (surviving cell density). PTD-FNK significantly suppressed a decrease in EGFP-positive cells at 1 and 2 weeks, and the tendency seemed to be continuing at 4 weeks. ∗ p<0.05 and ∗∗p<0.001 vs the PTD-FNK non-treatment group at 1 or 2 weeks by Student's t-test.
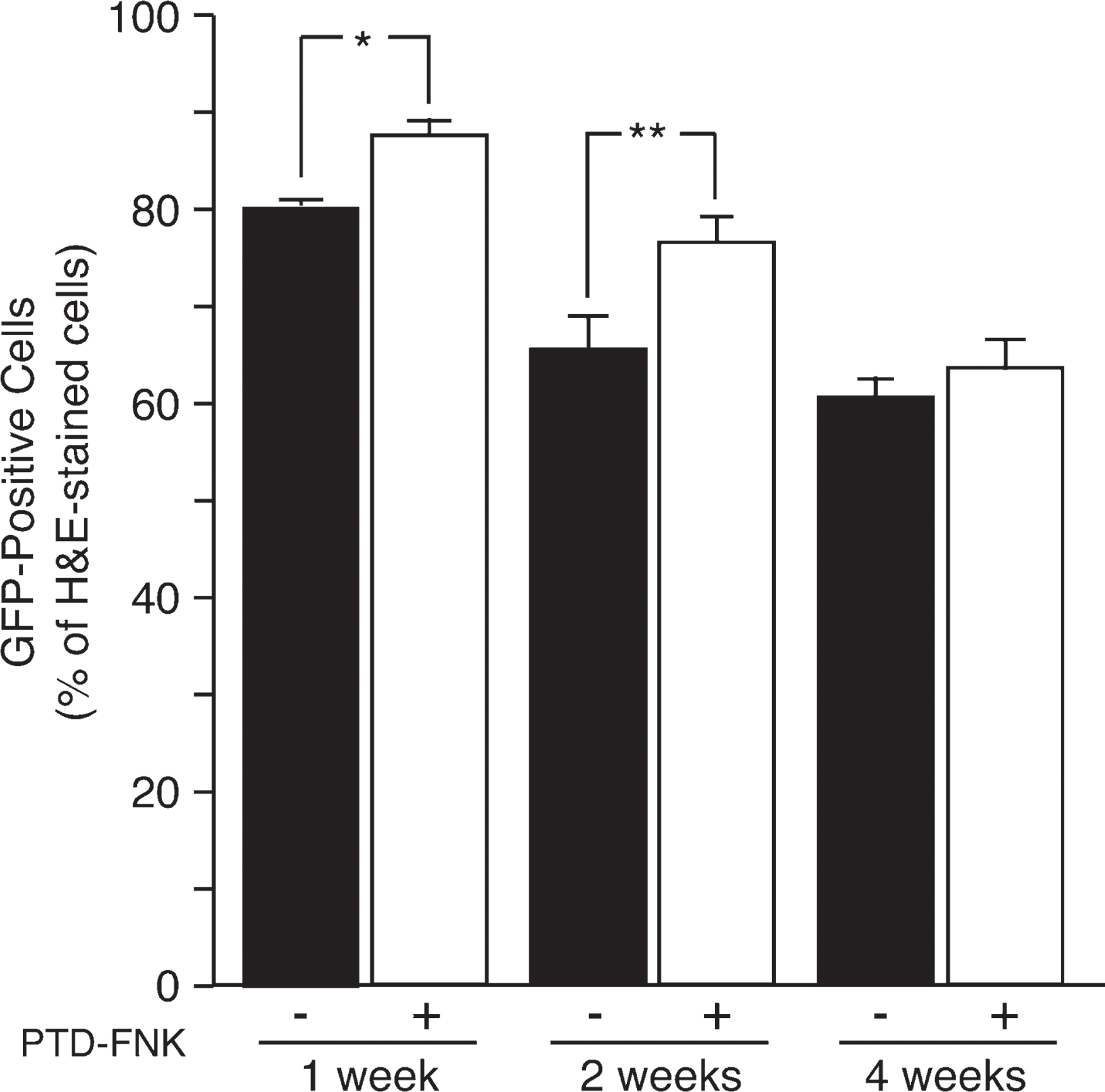
The number of EGFP-positive cells normalized against a number of hematoxylin-eosin-stained cells (survival rate) showed that PTD-FNK protected from cell death at 1 and 2 weeks, and the tendency seemed to be continuing at 4 weeks. ∗p<0.005 and ∗∗p<0.005 vs PTD-FNK non-treatment groups at 1 or 2 weeks by Student's t-test.
Chondrocyte Survival
Microscopic assessment of cartilage suggested that the PTD-FNK treatment group obtained higher scores of “cell distribution” at 1 week and “matrix” at 4 weeks, but there was no difference in the category “cell population viability” during the study period. The category “cell population viability” was roughly evaluated by the morphology of HE-stained cells and nuclei (e.g., pyknotic nuclei in a dying or dead cell) (Mainil-Varlet et al. 2003); therefore, the evaluation is not quantitative. To study the survival effect of PTD-FNK on chondrocytes in grafts, EGFP-positive cells in the cartilage layer of grafts were counted, because surviving chondrocytes of osteochondral grafts prepared from SD-Tg (CAG-EGFP) rats expressed EGFP during the study period (Figure 3).
The number of EGFP-positive cells was normalized against the area of the cartilage layer (Figure 4). PTD-FNK significantly suppressed a decrease in EGFP-positive cells at 1 and 2 weeks, and the tendency seemed to continue at 4 weeks. The number of EGFP normalized against the number of HE-stained cells also showed that PTD-FNK protected against cell death, although the difference was smaller (Figure 5). To evaluate dying or dead cells, TUNEL staining was performed. The results showed that PTD-FNK inhibited cell death (Figure 6), conforming to the above results. These results indicate that PTD-FNK protects chondrocytes from cell death caused by transplantation.
Discussions
This study showed that the degeneration of cylindrical osteochondral autografts, which were transplanted into the full thickness of articular cartilage defects by impact insertion, was suppressed when they were submerged in anti-cell death PTD-FNK protein before transplantation. Furthermore, the increased cell death and decreased survival rate and density of GFP-positive graft cells, which occurred with time in the early stage after transplantation, were also suppressed in grafts treated with PTD-FNK.
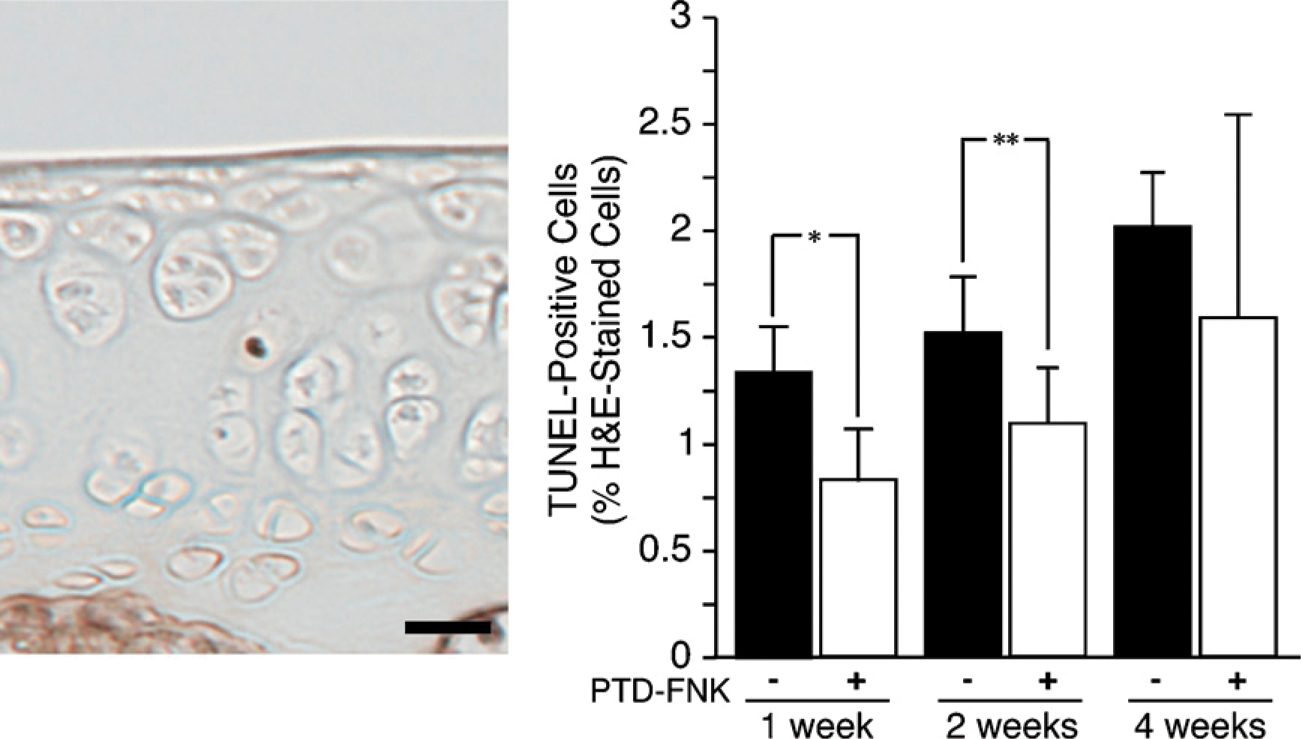
PTD-FNK inhibited cell death. Representative section of terminal deoxynucleotidyl transferase (TdT)-mediated deoxyuridine triphosphate (dUTP)-nick end-labeling staining (left). PTD-FNK significantly inhibited cell death at 1 and 2 weeks, and a similar tendency was found at 4 weeks (right). ∗p<0.05 and ∗∗p<0.005 vs PTD-FNK non-treatment groups at 1 or 2 weeks by Student's t-test.
PTD-FNK has been shown to inhibit cell death pathologically caused in various tissues, including the brain and liver, and caused by bone marrow transplantation and freezing/thawing, as mentioned above (Asoh and Ohta 2008). This study showed that the density and survival rate of the GFP-positive cells of PTD-FNK-treated grafts were significantly higher than those of PTD-FNK-untreated grafts but decreased with time during the study period. In the previous study, PTD-FNK was shown to be introduced into the chondrocytes from the superficial layer to a depth of 200 μm after 6 hr, when the cartilage slice was submerged in a solution containing PTD-FNK in vitro (Ozaki et al. 2004). The microenvironment of a cylindrical osteochondral graft, for example, blood supply to the subchondral bone and metabolism, and nutrition of the cartilage, is not the same as that of normal articular cartilage. In particular, in the early period after transplantation, horizontal mechanical stress on grafts decreases and the biological contact of subchondral bone between graft and host is lost, which generates an abnormal mechanical environment in the grafts; therefore, some environmental changes could cause chondrocyte death in grafts, regardless of PTD-FNK treatment. However, these results suggest that more chondrocytes were protected from cell death by PTD-FNK treatment at 1 and 2 weeks, resulting in matrix with a histologically normal appearance at 4 weeks.
PTD-FNK was degraded with a half-span of ∼2 hr when introduced into a cultured cell (Asoh et al. 2002); PTD-FNK was degraded with a half-span of 3.6 or ∼2 hr when systemically delivered into the brain or liver, respectively (Asoh et al. 2005; Katsura et al. 2008). Despite the short half-span of PTD-FNK in a cell, the cytoprotective effect of PTD-FNK obviously continued for at least 2 weeks when introduced into chondrocytes in cartilage. It is unlikely that PTD-FNK is very slowly degraded in chondrocytes. Meanwhile, chondrocytes are embedded in the cartilage matrix, which is rich in chondroitin sulfate containing high levels of sulfate with a negative charge. It is expected that chondroitin sulfate electrostatically interacts with PTD-FNK, because the PTD is rich in positively charged amino acid residues. It is possible that the matrix functions as a reservoir to store and supply PTD-FNK in the long term. PTD-FNK may gradually be dissociated from matrix components and introduced into chondrocytes. Otherwise, PTD-FNK exhibits cytoprotective activity only on the first day or for the first several days after transplantation, which may simply result in better survival of the cells at 1 and 2 weeks. Further effort is necessary to improve the survival of chondrocytes and the properties of cylindrical osteochondral grafts for hyaline cartilage. Strategies are also sought to enhance the transduction of PTD-FNK to the subchondral bone because there was no histological difference in this area between PTD-FNK-treated and untreated grafts.
It remains unknown how PTD-FNK protects chondrocytes from mechanical stress during preparation and impact insertion of the graft. Recently, we showed that PTD-FNK inhibits an increase in the cytosolic calcium concentration induced by glutamate, thapsigargin, and an immunosuppressant, FK506, and protected primary cultured neocortical neurons and neuroblastoma cells from cell death (Asoh et al. 2002; Katsura et al. 2008). It is widely accepted that disruption of the regulation of intracellular calcium concentration leads to cell death (Giorgi et al. 2008). How do chondrocytes in cartilage respond to mechanical stress? Several studies showed that mechanical stress transiently induces an increase in intracellular calcium concentration in primary cultured chondrocytes (Guilak et al. 1999; D'Andrea et al. 2000; Kono et al. 2006). Mechanical stress also induced ATP release from chondrocytes to the extracellular matrix (Hatori et al. 1995), and direct ATP application to rat cartilage slices induced transient elevation of intracellular calcium concentration (Kumahashi et al. 2004). Recently, Huser and colleagues (2006, 2007) reported that a single impact load induces a release of calcium from the endoplasmic reticulum, causing mitochondrial depolarization and caspase-9 activation resulting in apoptosis-like cell death of chondrocytes in cartilage within 24-48 hr. It is possible that PTD-FNK prevents the increase of intracellular calcium ions induced by mechanical stress and protects the chondrocytes from cell death. Further study remains necessary to investigate the mechanisms by which PTD-FNK protects chondrocytes from cell death associated with cylindrical osteochondral graft transplantation.
In conclusion, we present the efficacy of PTD-FNK to protect from cell death and suppress the degeneration of cylindrical osteochondral grafts. The histological score was well maintained, and the survival rate and density of GFP-positive cells were predominant in PTD-FNK-treated grafts; therefore, the potential of antiapoptotic protein PTD-FNK to suppress the degeneration of cylindrical osteochondral autograft was shown.