
Abstract
Radiotherapy is the first-line treatment for all stages of cervical cancer, whether it is used for radical or palliative therapy. However, radioresistance of cervical cancer remains a major therapeutic problem. Consequently, we explored if E-cadherin (a marker of epithelial-mesenchymal transition) and osteopontin could predict radioresistance in patients with locally advanced cervical squamous cell carcinoma (LACSCC). Patients were retrospectively reviewed and 111 patients divided into two groups (radiation-resistant and radiation-sensitive groups) according to progression-free survival (PFS). In pretreated paraffin-embedded tissues, we evaluated E-cadherin and osteopontin expression using immunohistochemical staining. The percentage of patients with high osteopontin but low E-cadherin expression in the radiation-resistant group was significantly higher than those in the radiation-sensitive group (p<0.001). These patients also had a lower 5-year PFS rate (p<0.001). Our research suggests that high osteopontin but low E-cadherin expression can be considered as a negative, independent prognostic factor in patients with LACSCC ([Hazard ratios (95% CI) 6.766 (2.940, 15.572)], p<0.001).
Keywords
Introduction
Cervical cancer is the third-most commonly diagnosed cancer affecting females worldwide (Ferlay et al. 2010) and data from 187 countries confirm that global cases of cervical cancer have increased at a rate of 0.6% per year from 1980 to 2010 (Forouzanfar et al. 2011). Radiotherapy is first-line treatment for all stages of cervical cancer, whether it is used for radical or palliative therapy (Kim et al. 2013; Rose 2000). However, tumor-cell resistance to radiation contributes to treatment failures (Nakano et al. 2010; Randall et al. 2010). Thus, understanding the molecular mechanisms of radiation resistance may permit the development of novel therapeutics to treat cervical cancer (Liu et al. 2010; Randall et al. 2010).
Epithelial-mesenchymal transition (EMT) is an essential, physiological process in mammalian embryonic development; but inappropriate EMT in tumors encourages tumor cell invasion and metastases. Inducing EMT in epithelial tumor cells results in a loss of cell polarity and the acquisition of mesenchymal traits that reduce tumor cell adhesion and increase their motility (Zeisberg and Neilson 2009). Currently, studies suggest that EMT is not only associated with invasion and metastasis, but also contributes to radiation resistance in tumors. Non-small cell lung cancer cells that survive radiation express significantly increased levels of EMT markers, such as Snail and vimentin (Gomez-Casal et al. 2013). Evidence (Theys et al. 2011) suggests that changes in the tumor microenvironment, such as intratumoral hypoxia, can induce radiation resistance by down-regulating E-cadherin expression and initiating EMT. Also, cells that express E-cadherin are more sensitive to radiation than those that do not. Early studies indicate that the hallmark of EMT is a loss of E-cadherin (De Craene and Berx 2013; Scanlon et al. 2013; Zeisberg and Neilson 2009) and emerging evidence suggests that osteopontin, a molecule involved in radiation resistance, may also be involved in the process of EMT (Li et al. 2013; Mi et al. 2009; Mi et al. 2011). Both of these ideas suggest that there may be a relationship between aberrant expression of E-cadherin and osteopontin, which are associated with EMT and radiation resistance.
E-cadherin, a calcium-dependent cell-cell adhesion molecule existing in non-neural epithelial cells, maintains epithelium polarity and tissue integrity. Research suggests that certain epithelial cancer cell lines and tumor tissues have decreased E-cadherin expression related to tumor invasion and metastasis. Research from Cheng and colleagues on cervical cancer indicates that E-cadherin down-regulation in tumor cells is positively related to nodal metastases, recurrence and distant metastases. Patients with high E-cadherin expression had better prognoses than patients with low or negative E-cadherin expression (Cheng et al. 2012). Furuyama and coworkers reported cells with low E-cadherin expression grew with less cell-cell attachment and showed more invasive potential than cells with high E-cadherin expression (Furuyama et al. 2000). Moreover, this phenomenon can be reversed at the transcriptional level. In addition, weak expression of E-cadherin has been shown to up-regulate epidermal growth factor receptor (EGFR) expression at the transcriptional level and activate EGFR and its downstream signaling pathways, inducing proliferation of head and neck squamous cells (Wang et al. 2011). Blocking E-cadherin expression facilitates invasion in a matrix metalloproteinase (MMP)2-dependent manner, with aberrant activation of the EGFR/mitogen-activated protein kinase kinase (MEK)/extracellular signal-regulated kinase (ERK) signaling pathway, thus promoting tumor cell invasion and metastases (Bae et al. 2013). So, E-cadherin is important not only in intercellular adhesion but also in cell signal transduction. At this time, few studies link E-cadherin with ionizing radiation outcomes.
Osteopontin, a phosphorylated protein, was first described by Senger in 1979 as a marker of epithelial cell transformation (Rittling and Chambers 2004). Osteopontin exists in various cells and tissues, including inflammatory, secretary epithelial, bone, kidney, and vascular cells, with roles in immune response, vascular remodeling, and wound repair, among other physiological processes (Anborgh et al. 2010; Ashkar et al. 2000). Osteopontin is also expressed in tumor, inflammatory, and stromal cells in many cancers (Anborgh et al. 2010), and its elevated expression is closely associated with tumor carcinogenesis and progression (Forootan et al. 2006; Rud et al. 2013; Song et al. 2009; Zhang et al. 2012). Song et al. (2009) reported that osteopontin expression in carcinoma in situ (CIS) of the cervix and invasive cervical cancer tissues was significantly higher than that found in normal cervical tissues, and the intensity of osteopontin staining was stronger in invasive cervical cancer as compared with that of CIS. These findings suggest that osteopontin expression increases with malignant formations. Studies correlating osteopontin with radiation responses indicate that elevated osteopontin expression can induce radiation resistance in breast cancer cells and osteopontin knockdown in combination with irradiation has additive effects on clonogenic survival, migration and the induction of apoptosis (Chang et al. 2012; Hahnel et al. 2010) .
The role of E-cadherin and osteopontin expression in cervical cancer patient responses to radiation has not been evaluated. To address this, we immunohistochemically analyzed E-cadherin and osteopontin expression in pretreated, paraffin-embedded tissues from patients with locally advanced cervical squamous cell carcinoma (LACSCC). Then, we evaluated the relationship between the expression of these two markers and the clinicopathological characteristics, radiotherapy sensitivity and survival of the samples.
Materials & Methods
Patients and Clinical Tissue Samples
This retrospective cohort study comprised 111 patients who had received primary radical radiotherapy in the Department of Radiation Oncology, Xiangya Hospital and Affiliated Tumor Hospital of Xiangya Medical School, Central South University, Changsha, China between January 2005 and March 2012. The inclusion criteria were as follows: (a) pathologically proven squamous cell carcinoma (SCC) of the cervix, (b) no evidence of distant metastasis at diagnosis (FIGO stage Ib-IVa), (c) the existence of tissue blocks available for our research, and (d) no other anticancer treatment before primary radiotherapy or post-radiotherapy surgery. The study was approved by the Research and Ethics committee of our institution. Follow-up was closed in May 2012. The median follow-up for survivors was 46 (range, 2 to 85.5) months. The median progression-free survival (PFS) was 49 (range, 0 to 85.5) months. The median age was 50 (range, 28 to 80) years. The 111 patients were divided into two groups: radiation-sensitive (n=85) and radiation-resistant (n=26) groups (Kim et al. 2006). The radiation-sensitive group included patients who had no local recurrence or distant metastases for at least 3 years after primary treatment (PFS ≥36 months). The radiation-resistant group included patients who had tumors that did not respond to radiotherapy at all, or who had experienced local recurrence with or without distance metastasis at a time point less than 3 years after primary treatment (PFS <36 months). PFS was defined as the period from the end of therapy to the date of the first documented evidence of recurrence or metastatic disease, as determined by clinical physical examination data, pathological biopsy, or imaging studies. Each cervical primary tumor diameter was directly measured during clinical physical examination rather than by imaging.
All patients were treated with external beam radiotherapy (EBRT) and high-dose rate (HDR) intracavitary brachytherapy after consultation with a radiation oncologist. HDR brachytherapy was initiated at 3 to 4 weeks after the commencement of EBRT. The median total dose at point A was 90 (range, 66 to 102) Gy. The median dose of EBRT at point A was 46 (range, 30 to 52) Gy. The median dose of HDR brachytherapy at point A was 42 (range, 20 to 54) Gy.
Immunohistochemistry
For immunohistochemical detection of osteopontin and E-cadherin, 4-μm tissue sections were deparaffinized in xylene followed by microwave treatment (osteopontin for 10 min, E-cadherin for 15 min at moderate heating) in 0.01 M citrate buffer (pH 6.0). After cooling for 30 min and washing in PBS, endogenous peroxidase was blocked with 3% hydrogen peroxide for 30 min, followed by incubation with PBS containing 10% normal goat serum for 30 min. Specimens were incubated overnight at 4C with anti-osteopontin (Santa Cruz Biotechnology Inc.; Dallas, TX) and anti-E-Cadherin (Cell Signaling Technology Inc.; Beverly, MA) antibodies, both at a dilution of 1:100. Immunostaining was detected using the ChemMate Kit (Dako; Glostrup, Denmark) and 3,3-diaminobenzidine as a chromogen. For negative controls, the primary antibodies were replaced by nonimmune isotypic antibodies.
Evaluation of Staining
Stained tissue slides were viewed separately by two pathologists who were blinded to the clinical or clinicopathological status of the patients. Osteopontin and E-cadherin expression for each slide was evaluated by scanning the entire tissue specimen under low-power (×40) and confirmed under high-power (×400) magnification. An immunoreactivity score (IRS) system (Xu et al. 2013) was applied as follows: (a) the number of stained cells was scored as 0 (no staining), 1 (≤1/3 positive cells), 2 (>1/3 and ≤2/3 positive cells), or 3 (>2/3 positive cells); and (b) immunostaining intensity was scored as 0 (negative), 1 (weak), 2 (moderate), or 3 (strong). The sum of the staining intensity and staining extent scores was used as the final immunoreactive score (0-6), which were then regarded as negative (score of 0–1) or positive (score of 2–6). We stained 111 blocks and, for each block, chose five random areas to obtain weighted scores according to the percentage of positive tumor cells and staining intensity at under high-power magnification. Thus, we had five weighted scores for each block, and scores may have been different for one patient. Thus, we selected the median weighted score from the five weighted scores as the typical score and these data were analyzed.
Statistical Analysis
The relationships between osteopontin and E-cadherin expression and clinicopathological factors were analyzed using the Chi-square test and Fisher’s exact test. The radiation dose used in the radiation-resistant and radiation-sensitive groups was estimated using the student’s t-test. The relationship between osteopontin and E-cadherin was analyzed using the Spearman test. Survival curves were plotted using the Kaplan-Meier method, and differences between groups were assessed using the log-rank test. Univariate and multivariate survival analyses were performed according to the Cox proportional hazards model. Osteopontin expression alone (high vs low), E-cadherin expression alone (high vs low), high osteopontin and low E-cadherin expression (yes vs no), age (≥50 years vs <50 years), FIGO stage (III + IVa vs Ib + II), histopathological grade (middle + low vs high), tumor diameter (>4 cm vs ≤4 cm) were included in the regression model. For all statistical tests, a p≤0.05 was considered statistically significant.
Results
Patient Clinical and Histopathological Characteristics
Clinical and histopathological characteristics of the patients enrolled in the study are detailed in Table 1. Of the 111 cervical squamous cell carcinomas, 26 were radiation-resistant. There were significant differences in FIGO stage and tumor diameter between the two groups (p=0.002 and p=0.001, respectively), but no significant differences in patient age, histopathological grade, combined chemotherapy (platinum-based), total dose of point A, EBRT dose of point A or brachytherapy dose of point A between the two groups.
Patient Characteristics.
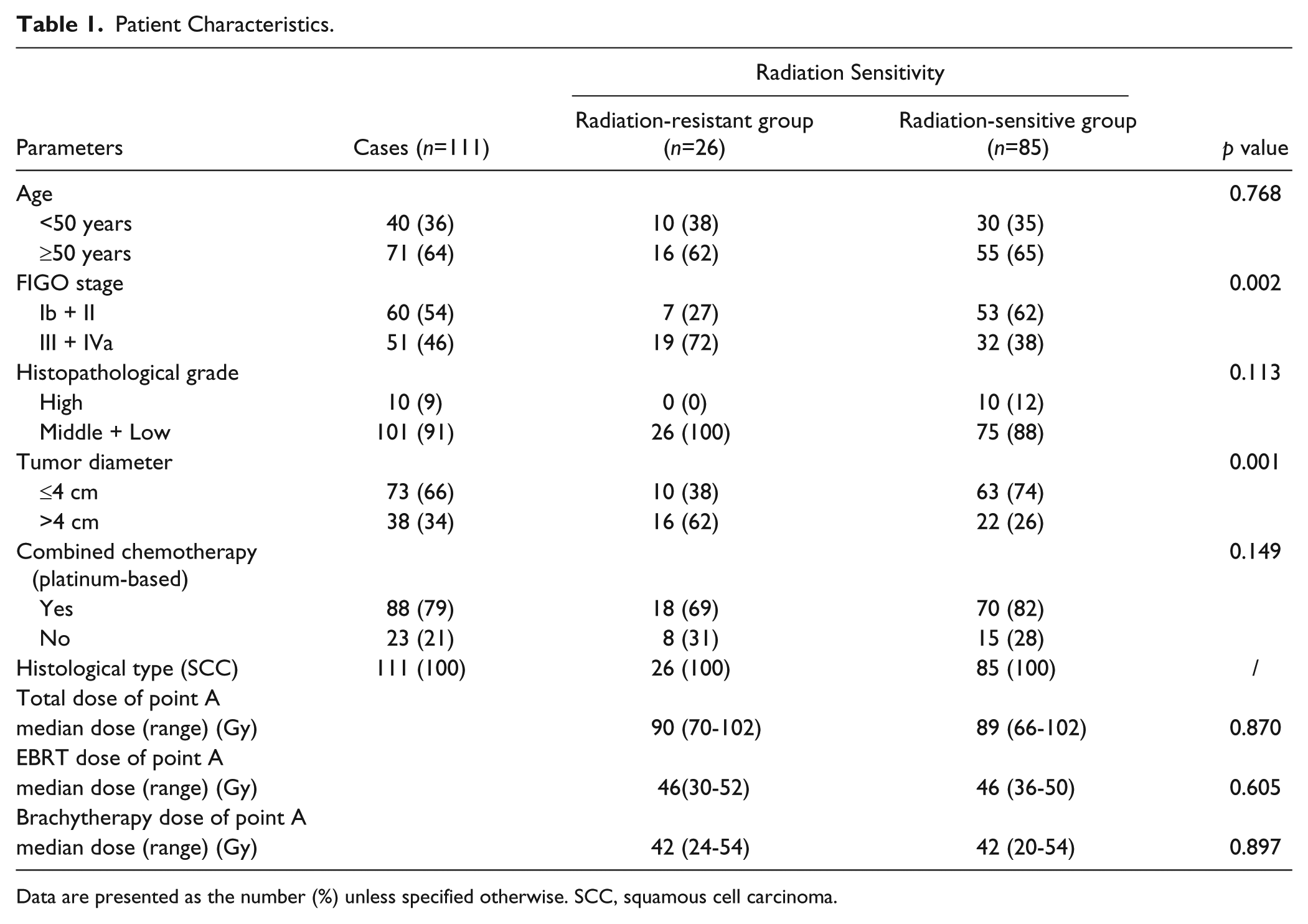
Data are presented as the number (%) unless specified otherwise. SCC, squamous cell carcinoma.
Osteopontin and E-Cadherin Expression and Clinicopathological Parameters
Osteopontin was located in the membrane and cytoplasm of cervical carcinoma cells and staining here was much stronger in radiation-resistant cases (compare Fig. 1A, 1B). Table 2 depicts the osteopontin expression data. A significant relationship was observed between osteopontin expression and FIGO stage (p<0.001) and tumor diameter (p=0.035), but no significant relationship between osteopontin expression and patient age (p=0.82) or histopathological grade (p=0.508) was observed.
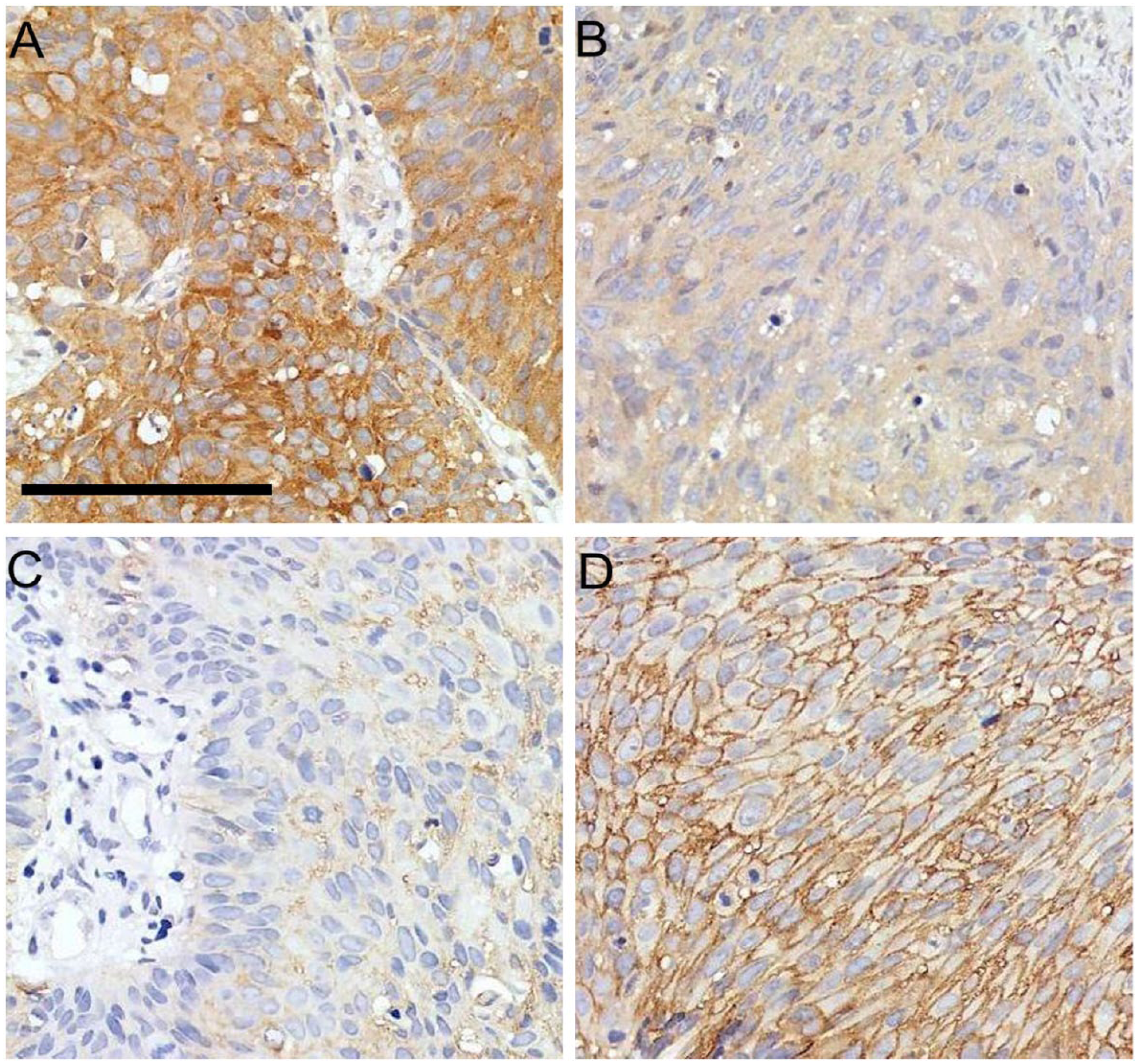
Representative examples of osteopontin and E-cadherin staining in radiation-resistant group and radiation-sensitive group (×400). (A) Strong positive staining of osteopontin in the radiation resistant group. (B) Weak positive staining of osteopontin in the radiation-sensitive group. (C) Weak positive staining of E-cadherin in radiation-resistant group. (D) Strong positive staining of E-cadherin in radiation-sensitive group. The scale size is the same for all the figures. Scale, 90 μm.
Association of Osteopontin and E-cadherin Expression with Clinicopathological Parameters of Cervical Squamous Carcinoma and Response to Radiotherapy.
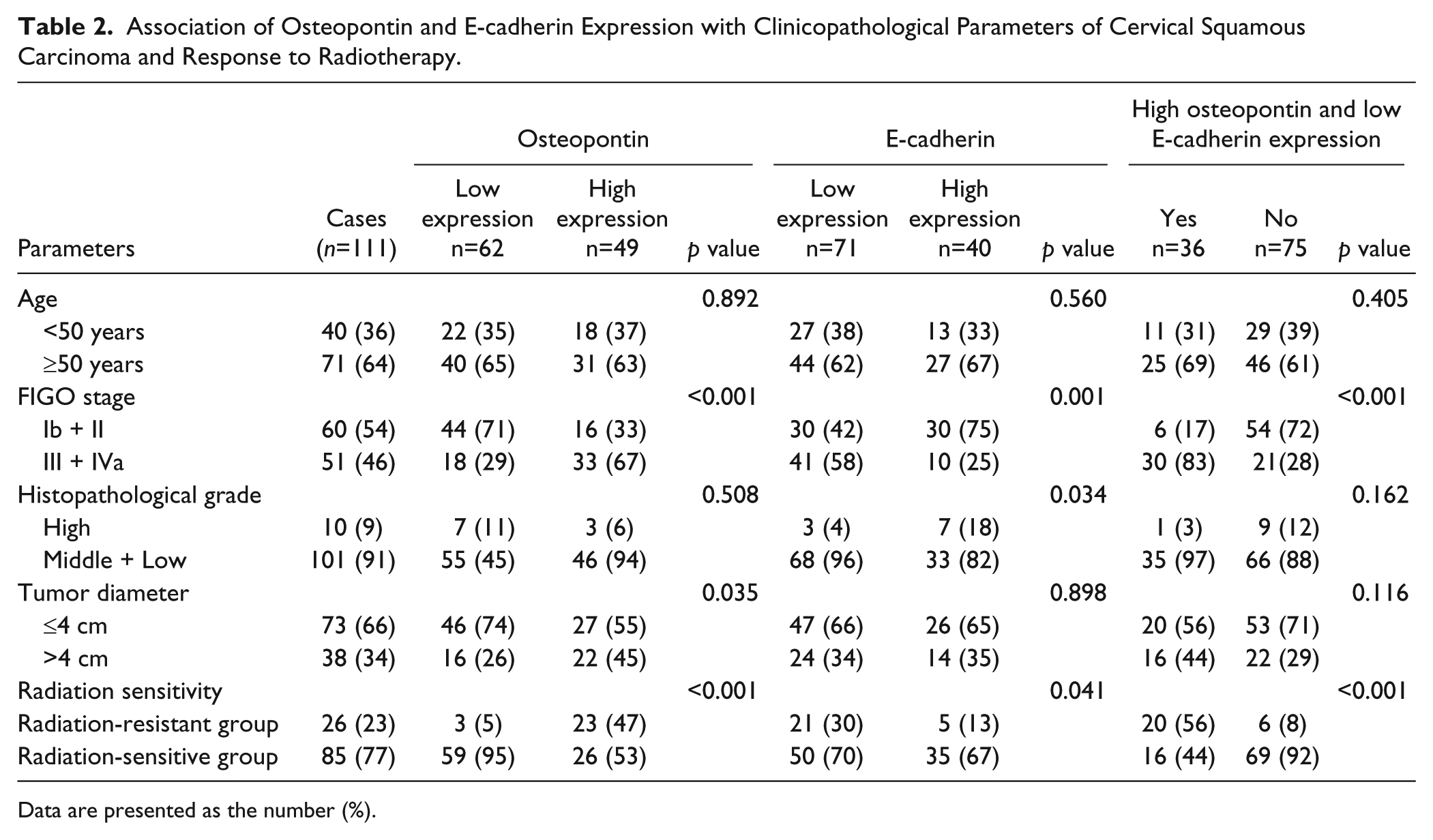
Data are presented as the number (%).
E-cadherin was located in the membrane of cervical carcinoma cells, and staining here was weaker in the radiation-resistant group (compare Fig. 1C, 1D). Table 2 shows E-cadherin data; a significant relationship was observed between E-cadherin expression and FIGO stage (p=0.001) and histopathological grade (p=0.034). However, no significant relationship was observed between E-cadherin expression and patient age (p=0.560) or tumor diameter (p=0.898).
Data for the expression of osteopontin and E-cadherin in 111 LACSCC patients are also given in Table 2. A significant relationship was observed between high osteopontin and low E-cadherin expression and FIGO stage (p<0.001), but no significant relationship was observed between high osteopontin and low E-cadherin expression and patient age (p=0.405), histopathological grade (p=0.162) or tumor diameter (p=0.116).
Relationship between Expression of Osteopontin and E-Cadherin
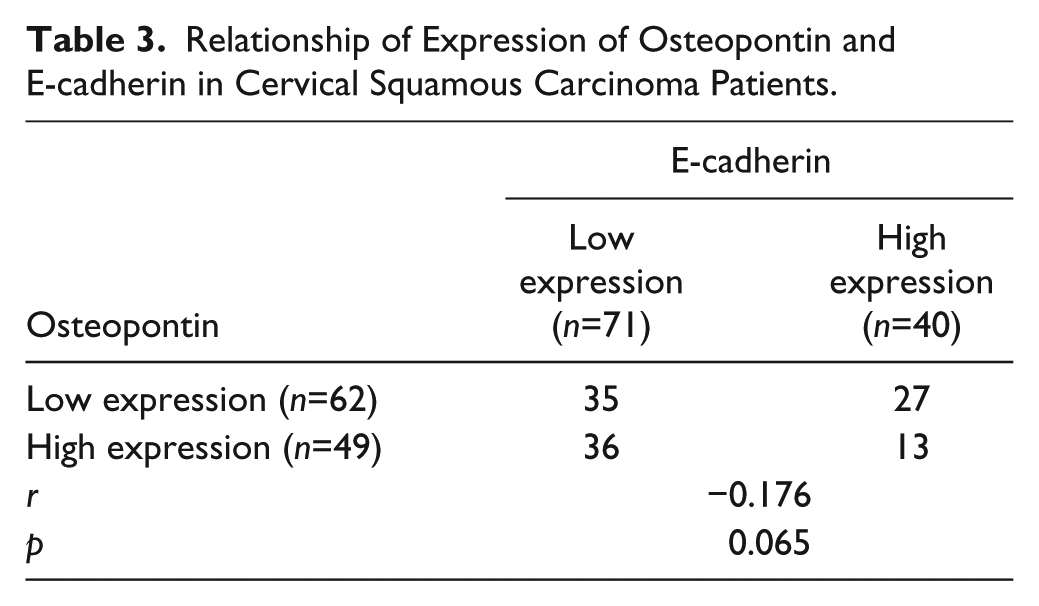
In total, 111 qualified cases were evaluated for osteopontin and E-cadherin expression using immunostaining and this was used to classify markers as low or high (Table 3). No significant relationship was observed between osteopontin and E-cadherin expression (r=-0.176, p=0.065).
Relationship of Expression of Osteopontin and E-cadherin in Cervical Squamous Carcinoma Patients.
Osteopontin and E-Cadherin Expression and Radiotherapy Response
Data from the immunohistochemical quantification of osteopontin expression in the 111 LACSCC patients are summarized in Table 2. Comparing the proportions of patients with high osteopontin expression revealed statistically significant differences between the radiation-resistant and radiation-sensitive groups (p<0.001). Data regarding E-cadherin expression in the 111 LACSCC patients are also summarized in Table 2. Comparing patients with high E-cadherin expression revealed a statistically significant difference between radiation-resistant and radiation-sensitive groups (p=0.041). Furthermore, the proportion of patients with high osteopontin but low E-cadherin expression revealed statistically significant differences between radiation-resistant and radiation-sensitive groups (p<0.001; Table 2).
Osteopontin and E-Cadherin Expression and Patient Survival
The patient cohort was stratified according to tumor osteopontin expression, and we found that the 5-year PFS rates in patients with low osteopontin expression (62 cases) and high osteopontin expression (49 cases) were 92.42% and 63.42%, respectively. A Kaplan-Meier analysis (log-rank test) revealed a significant difference between the two groups (p<0.001; Fig. 2A).
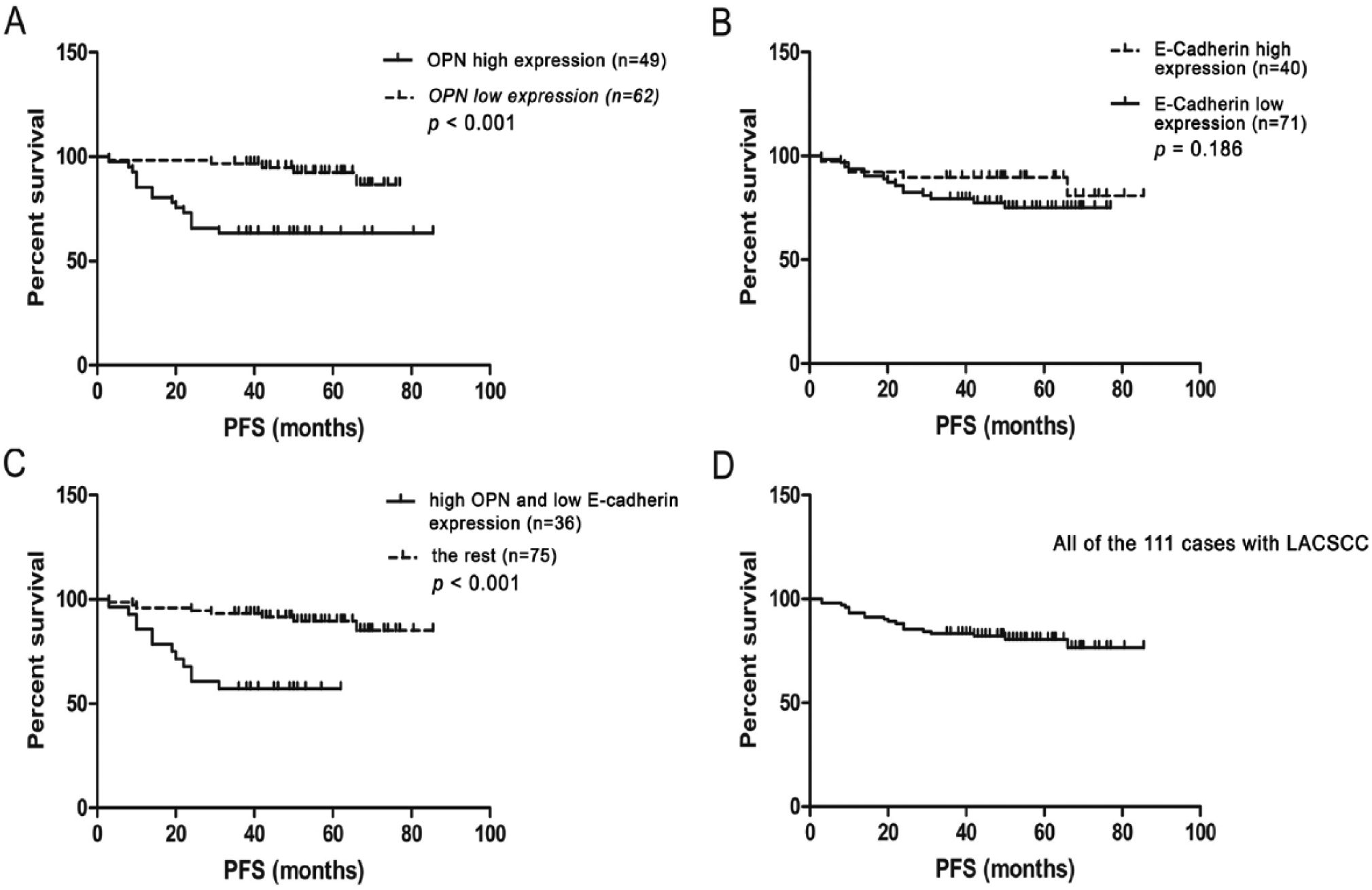
Kaplan-Meier curves of overall survival for patients with locally advanced cervical squamous cell carcinoma (LACSCC). (A) The 5-year progression-free survival (PFS) rates were 92.42% and 63.42%, respectively, in patients with low osteopontin expression (n=62) and high osteopontin expression (n=49). There was a significant difference in the overall survival rate between the two groups (p<0.001). (B) The 5-year PFS rates were 75.08% and 89.70%, respectively, in patients with low E-cadherin expression (n=71) and high E-cadherin expression (n=40); no significant difference in overall survival rate was found between the two groups (p=0.189). (C) The 5-year PFS rates were 57.14% and 89.59%, respectively, in patients that showed high osteopontin but low E-cadherin expression (n=36) and the rest of the cohort (n=75). There was a significant difference in the overall survival rate between these two groups (p<0.001). (D) The 5-year PFS rate was 80.55% in all the 111 cases with LACSCC.
With respect to E-cadherin expression, the 5-year PFS rates in patients with low E-cadherin expression (71 cases) and high E-cadherin expression (40 cases) were 75.08% and 89.70%, respectively; Kaplan-Meier analysis (log-rank test) revealed no significant difference between the two groups (p=0.189, Fig. 2B). When the patient cohort was stratified according to high osteopontin but low E-cadherin expression, the 5-year PFS rate was 57.14% in patients with high osteopontin but low E-cadherin expression (36 cases) and 89.59% for the remaining patients (75 cases). Of note, patients with tumors with high osteopontin but low E-cadherin expression had a worse prognosis than other patients (Kaplan-Meier analysis, log-rank test, p<0.001; Fig. 2C). The 5-year PFS rate for all 111 patients was 80.55% (Fig. 2D).
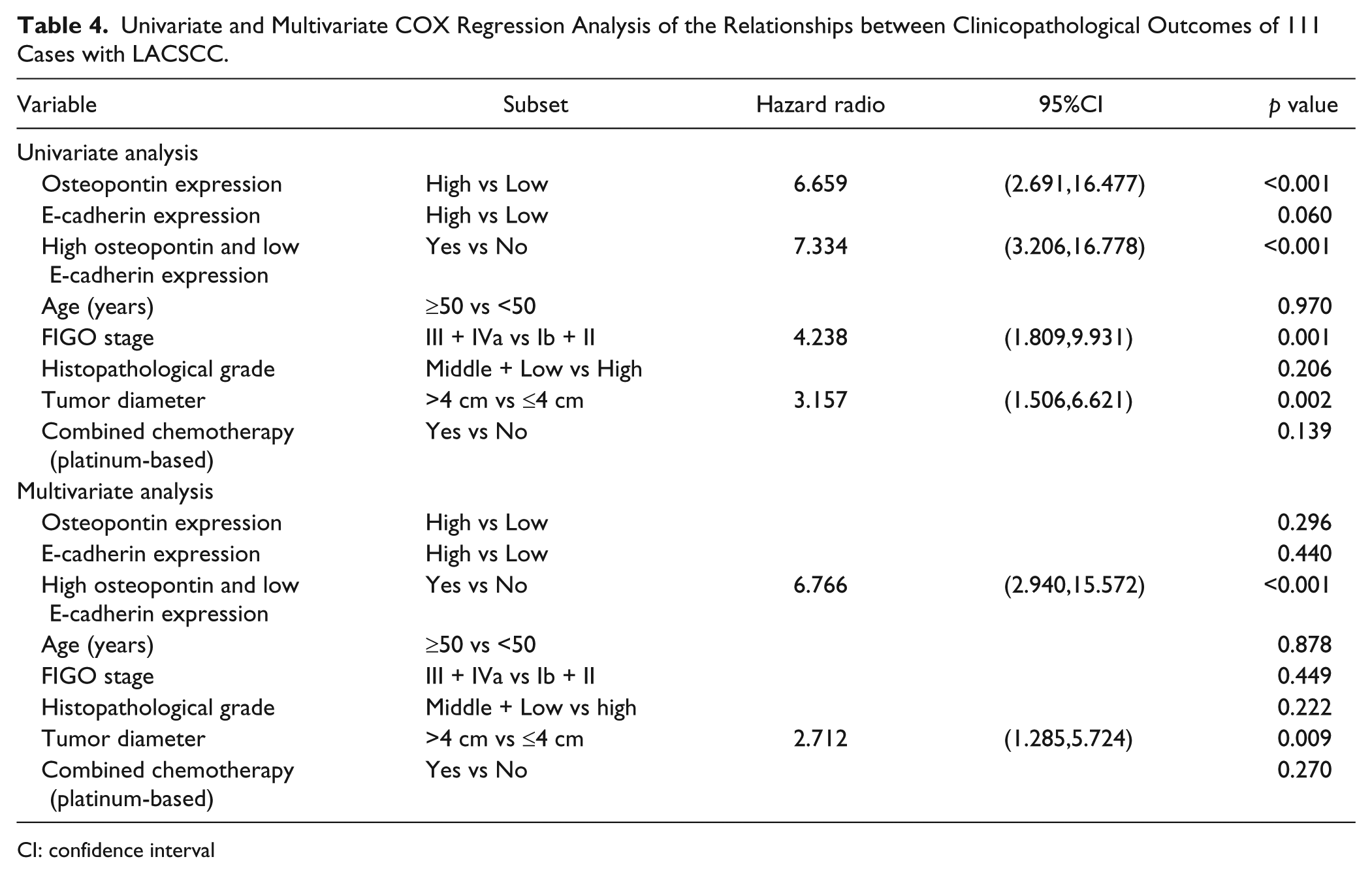
The univariate and multivariate Cox regression analysis data for hazard ratios are depicted in Table 4. The multivariate Cox regression analysis data indicated that high osteopontin and low E-cadherin expression was an informative independent prognostic factor regarding our cohort of patients with LACSCC [Hazard ratio (95% CI), 6.766 (2.940, 15.572); p<0.001]. In addition, tumor diameter was also an independent prognostic predictor.
Univariate and Multivariate COX Regression Analysis of the Relationships between Clinicopathological Outcomes of 111 Cases with LACSCC.
CI: confidence interval
Discussion
We observed that E-cadherin expression was associated with FIGO stage and histopathological grade, but not with other factors. Similarly, Cheng et al. (2012) reported strong E-cadherin expression was associated with poor histological differentiation and the nodal metastatic stages of cervical squamous cell cancer. Our data suggest that E-cadherin expression seems to be associated with 5-year PFS rates, even though the difference was not significant, and that low E-cadherin expression was not an independent predictor of survival. Furthermore, Yong’s group also considered low E-cadherin expression to be a predictor of tumor-specific poor survival. Thus, we posit that E-cadherin plays a role in resistance to radiotherapy, and that this results in poor prognosis.
In our studies of E-cadherin expression and radiation resistance, we observed that the radiation-sensitive group had more E-cadherin expression than the radiation-resistant group. Furthermore, a significant difference existed between these two groups. Emerging evidence shows that a loss of E-cadherin promotes metastasis, as E-cadherin is a vital protein for cell transforming via EMT and MET (Mareel et al. 2009; Onder et al. 2008). Our study, however, suggests a broader role for E-cadherin, beyond cellular adhesion, in radiotherapy sensitivity.
Osteopontin, a molecule involved in initiating EMT, was relevant to FIGO stage and tumor diameter in our research. In gastric cancer (Tang et al. 2008), a similar importance was found between osteopontin expression and clinical stages, nodal metastasis, and distant metastasis. Emerging data support a role for osteopontin as a potential prognostic factor in various human tumors, including non-small cell cancer (Rud et al. 2013), hepatocellular carcinoma (Zhang et al. 2012), and prostate cancer (Forootan et al. 2006). However, the correlation between osteopontin expression and survival is controversial in cervical cancer. Cho and colleagues (Cho et al. 2008) have reported that high osteopontin expression was associated with overall survival (p=0.002) and disease-free survival (p=0.033). In contrast, Song et al. (2009) reported that no significant correlation existed between osteopontin and survival. Our data indicate that patients with elevated osteopontin expression have a low 5-year disease-free survival rates but elevated osteopontin expression was not an independent predictor of survival. In our study, osteopontin expression was inversely correlated with radiation response. Previous work has shown that osteopontin knockdown improves radiobiological effects in breast cancer cells in vitro (Hahnel et al. 2010). These loss-of-function tests support our conclusion. However, how osteopontin is associated with biological radiation resistance is uncertain. As osteopontin is thought to be an indicator of endogenous tissue hypoxia response (Bache et al. 2006; Hahne et al. 2013; Le et al. 2003; Said et al. 2007; Yang et al. 2012) and tumor regrowth after radiotherapy (Solberg et al. 2008), we suggest that elevated osteopontin expression in cervical cancer is related to radiation resistance and this is partly due to hypoxia, which affects radiosensitivity- (Avanzo et al. 2010; Bouchat et al. 2010; Moeller et al. 2007) and radiotherapy-related regrowth. More importantly, osteopontin has been proven to play a role in the initiation of EMT, which is what led us to reflect on the issue of EMT and radioresistance.
Osteopontin can upregulate EMT by affecting changes in epithelial/mesenchymal markers in vitro, suggesting that osteopontin is involved in EMT (Mi et al. 2009; Mi et al. 2011). Li and colleagues (Li et al. 2013) reported that increased osteopontin-induced EMT transcription factor mRNA expression as compared with cell lines with low osteopontin expression and minimal EMT transcription factor mRNA expression. Furthermore, the use of osteopontin aptamer (APT) in cell lines with high osteopontin expression significantly decreased the expression of these EMT transcription factors, whereas treatment with exogenous osteopontin in cell lines with low osteopontin expression significantly increased EMT transcription factors. We conclude that osteopontin is critical in EMT initiation, as well as in driving and regulating EMT. Despite intensive research efforts to suggest that E-cadherin is a marker of phenotypic changes during EMT, there is little data regarding the relationship between E-cadherin and osteopontin expression and aberrant co-expression of E-cadherin and osteopontin in response to irradiation. We are the first to document a correlation between these and to conclude that osteopontin expression is negatively associated with E-cadherin expression; albeit this was not statistically significantly (r=-0.176; p=0.065). Next, we documented that high osteopontin but low E-cadherin expression was a more significant indicator than low E-cadherin expression alone for radiation resistance, suggesting that detection of both E-cadherin and osteopontin in tumor tissues may help estimate radiosensitivity. Third, patients with high osteopontin but low E-cadherin expression or high osteopontin expression alone had reduced 5-year disease-survival rates. And finally, only high osteopontin with low E-cadherin was an independent and negative prognostic factor for patient survival.
Patients with high osteopontin but low E-cadherin expression were radiation resistant. E-cadherin and osteopontin are both closely associated with EMT but how EMT-mediates such resistance is uncertain; three potential mechanisms may explain this observation. First, EMT induction in tumor cells promotes the expression of mesenchymal markers that acquire mobile traits as well as those of stem cell markers to gain stemness and self-renewal properties (Armstrong et al. 2011; Mani et al. 2008; Scheel and Weinberg 2012; Thiery et al. 2009). Such properties in tumors allow them to be referred to as cancer stem cells (CSCs) or “tumor-initiating cells” (Reya et al. 2001). Thus, we suggest that treatment failure may be due to the existence of CSCs, which are resistance to radiotherapy, in tumors. The mechanism of CSC radioresistance may be concurrent and distinct; studies investigating DNA checkpoint damage, anti-apoptotic responses, reactive oxygen species, Wnt/β-catenin and Hedgehog-Gli1 signaling have found these changes to be involved in cell survival and cell renewal after irradiation (Eyler and Rich 2008; Hittelman et al. 2010; Raimondi et al. 2010). The second potential mechanisms may be that EMT transcription factors, such as Slug and Snail, increase tumor cells invasiveness and capacity for migration as well as confer radioresistance. Slug-mutant or Slug-deficient mice were deemed radiation-sensitive; thus, Slug is also considered to contribute to tumor radioresistance (Inoue et al. 2002; Perez-Losada et al. 2003; Perez-Caro et al. 2008) . Slug mediates tumor cell survival from lethal irradiation via activation of a stem cell factor (SCF)/c-Kit signaling pathway (Perez-Losada et al. 2003), regulation of DNA damage repair (Perez-Caro et al. 2008) and inhibition of apoptosis induced by irradiation (Inoue et al. 2002). In addition, Snail is associated with apoptotic resistance (Vega et al. 2004) and affects cellular resistance to radiation-induced apoptosis (Escriva et al. 2008), resulting in radiation resistance. The last explanation may involve reversible EMT within tumor cells (Armstrong et al. 2011; Thiery 2002; Yang and Weinberg 2008; Zeisberg and Neilson 2009), which would suggest that tumor cells leave a primary tumor nodule and migrate to a new tissue site by EMT, to proliferate again and form a new tumor nodule via MET. The dynamic and reversible traits of EMT, which multiply the difficulties of investigating the relationship between EMT and radiation resistance, suggest that radiation resistance may be associated with this reversibility.
In summary, our data indicate that patients with high osteopontin expression, low E-cadherin expression or high osteopontin expression plus low E-cadherin expression are resistant to radiotherapy. Furthermore, only high osteopontin expression plus low E-cadherin expression is an independent and negative prognostic factor for patient survival. The relationship between EMT and radioresistance in cancer is a developing area and few studies have been undertaken to understand the underlying mechanisms. Thus, our data offer a new strategy for studying this mechanism at the molecular level.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by