
Abstract
Radiotherapy (RT) as a preoperative or postoperative adjuvant or primary treatment is the most common management modality for locally advanced cervical cancer. Radioresistance of tumor cells remains a major therapeutic problem. Consequently, we aimed to explore if the stem cell biomarkers SOX2 and OCT4 protein could be used to predict radioresistance in patients with locally advanced cervical squamous cell carcinoma (LACSCC). These 132 patients were divided into two groups (radiation-resistant and radiation-sensitive groups) according to progress-free survival (PFS). Using pretreatment paraffin-embedded tissues, we evaluated SOX2 and OCT4 expression using immunohistochemical staining. The percentage of overexpression of SOX2 and OCT4 in the radiation-resistant group was much higher than that in the radiation-sensitive group (p<0.001 and p <0.001, respectively). The patients with high expression of SOX2 and OCT4 showed a shorter PFS than those with low expression. Our study suggests that the expression of SOX2 and OCT4 in tumor cells indicates resistance to radiotherapy and that these two factors were important predictors of poor survival in patients with LACSCC (hazard ratio [95% CI], 2.294 [1.013, 5.195] and 2.300 [1.050, 5.037], respectively; p=0.046 and p=0.037, respectively).
Introduction
Cervical cancer is the third-most commonly diagnosed cancer and the fourth leading cause of cancer death in females worldwide (Jemal et al. 2011). Radiotherapy (RT) as preoperative or postoperative adjuvant or primary treatment can be utilized to treat all stages of cervical cancer. Although RT plays an important role in the treatment of locally advanced or inoperable cervical carcinoma, treatment outcomes remain poor when external beam RT (EBRT) and brachytherapy (BRT) are used. Tumor resistance to radiation is a major therapeutic problem (Kim et al. 2006). Since the response to RT and prognosis may differ between patients who have the same tumor diameter and FIGO stage, new markers need to be identified in order to more accurately predict the response of individual patients to RT and their prognosis.
Malignant tumors vary in their response to radiation as a consequence of resistance mechanisms at the molecular level. Radiosensitivity can be influenced by both intrinsic and extrinsic factors such as hypoxia (Rockwell et al. 2009; Dewhirst et al. 2008), the cell cycle (Shimura et al. 2010; He et al. 2011), DNA damage and repair (Bolderson et al. 2009; Beskow et al. 2009), apoptosis (Lehmann et al. 2007; Suzuki et al. 2007), growth factors and oncogenes (Mukherjee et al. 2009; Bergkvist et al. 2011), cancer stem cells (CSCs) and the epigenetic modification of genes (Baumann et al. 2008; Kawano et al. 2010). CSCs, which have been recognized as a source of local or distant cancer relapse, have the potential to dramatically affect clinical outcomes (Brunner et al. 2012). A CSC is defined as a cell within a tumor that possesses the capacity to self-renew and generate the heterogeneous lineages of cancer cells that comprise the tumor (Clarke et al. 2006). This definition directly implies that an anticancer therapy can eradicate a tumor if and only if all CSCs are killed. The radioresistance resulting from the presence of CSCs has been described in some cell lines and solid tumor types (Peitzsch et al. 2013). Essentially, these studies consist of combinations between available CSC biomarkers and radiobiological endpoints. Comprehensive lists of biomarkers used for the identification or isolation of putative CSCs in different tumor entities have been given in several recent reviews (Brunner et al. 2012).
Recently, the transcription factors SOX2 and OCT4 have been proposed as biomarkers for breast CSC-like cells in both cell lines and malignant tissues (Leis et al. 2012; Ezeh et al. 2005). Sex-determining region Y-box 2 (SOX2) is a high-mobility group (HMG) domain transcription factor and a member of the SRY-related HMG-box (SOX) family of transcription factors (Saigusa et al. 2009), and is known to bind in partnership with OCT4. OCT4 is an octamer-binding transcription factor that is a key regulator of pluripotency, differentiation and self-renewal in embryonic stem cells (ESCs) (Lengerke et al. 2011). SOX2 and OCT4, which are expressed in various tumor tissues but not in normal somatic tissues, indicate poor prognosis in some solid tumors, including prostate cancer, lung adenocarcinoma, gliomas, rectal cancer, gastric carcinoma and oral squamous cell carcinoma (Leis et al. 2012; Ezeh et al. 2005; Guo et al. 2011; Matsuoka et al. 2012; Luo et al. 2013; Saigusa et al. 2009; Wen et al. 2010; Atlasi et al. 2007; Chiou et al. 2008; Sholl et al. 2010). Knockdown of these genes can result in tumor cell apoptosis, decreased tumor sphere formation and inhibition of tumor formation in xenograft tumor models (Luo et al. 2013). Thus, accumulating evidence suggests that SOX2 and OCT4 may be strongly correlated with CSCs.
To clarify the association between the expression of stem cell markers and radioresistance in primary locally advanced cervical squamous cell carcinoma (LACSCC), we measured SOX2 and OCT4 expression before RT by means of immunohistochemistry. In primary LACSCC treated with primary RT, we evaluated the relationship between the expression of these two markers and the clinicopathological characteristics, RT sensitivity and survival of the samples.
Materials & Methods
Patients and Clinical Tissue Samples
From January 2005 to March 2012, 614 patients suffering from localized cervical squamous carcinoma (LSCC) were documented in the Radiation Oncology Department of Xiangya Hospital and Affiliated Tumor Hospital of Xiangya Medical School, Central South University, Changsha, P.R. China. Patients received no other anticancer treatment prior to primary radiotherapy (RT), or surgery after RT. Ninety-eight patients were diagnosed at other hospitals, where their tissue samples were saved, and these patients went on to receive RT in our hospitals. As these hospitals had their own management rules of tissue samples, we were unable to obtain the samples and the patients were thus excluded from our study. Among the remaining 516 patients whose follow-up period closed in May 2012, 205 patients had follow-up information but others were unreachable for various reasons (no phone, no phone number, no follow-up, among others). Seventy-three cases had clear PFS; however, they were excluded from our study because they showed no progression, the PFS was shorter than 36 months and therefore we could not assign these patients into one of the study groups. Finally, 132 cases were included in our study. The inclusion criteria were as follows: (a) pathologically proven squamous cell carcinoma (SCC) of the cervix; (b) no evidence of distant metastasis at diagnosis (FIGO stage Ib–IVa); (c) the existence of tissue blocks available for our research; (d) receipt of no other anticancer treatment prior to primary RT, or surgery after RT. The study was approved by the Research and Ethics Committee of our institution. The median follow-up time for survivors was 45 (range, 2–85.5) months. The median PFS was 43.5 (range, 0–85.5) months. The median patient age was 51 (range, 28–80) years. We divided the 132 patients into two groups: radiation-sensitive group (n=85) and radiation-resistant group (n=47) (Kim et al. 2006). The radiation-sensitive group included patients who showed no local recurrence and distant metastasis for ≥3 years after primary treatment (PFS ≥36 months). The radiation-resistant group included patients who had tumors that did not respond to RT at all, with local recurrence or distant metastasis at <3 years after the primary treatment (PFS <36 months). The radiation-resistant group was further divided into three subgroups: (1) a RT non-responsive subgroup comprising patients whose primary tumor persisted and did not shrink markedly after primary treatment until time of death; (2) a local recurrence subgroup comprising patients whose primary tumor had initially disappeared but subsequently showed local recurrence at <3 years after the primary treatment; and (3) a distant metastasis subgroup comprising patients whose primary tumor had disappeared after treatment but showed distant metastasis at <3 years after primary treatment. PFS was defined as the period from the end of therapy to the date of the first documented evidence of recurrence or metastatic disease. Evidence included clinical physical examination data, pathological biopsy or imaging studies. Each primary cervical tumor diameter was directly measured during clinical physical examination rather than by medical imaging. In our study, most patients with a shorter follow-up were classified into the resistant group. For example, one patient with FIGO stage IIIa LASCC had no cervical tumor after radiotherapy based upon the physical examination and pelvic CT scan. Two months later, however, this patient showed evidence of lung metastasis, as determined by a lung CT scan, which was used to diagnose the cause of a recurring cough. This patient chose to withdraw from treatment and we lost contact with her. Therefore, both follow-up and PFS for this patient were two months. Another patient experienced lung metastasis during RT and the cervical tumor did not respond to RT. This patient belonged not only to the RT non-responsive subgroup but also to the distant metastasis subgroup. Three patients experienced distant metastasis after RT, but their PFS was >36 months. Thus, we placed these patients in the radiation-sensitive group.
All patients were treated with EBRT and high-dose rate (HDR) intracavitary BRT after consultation with a radiation oncologist. HDR brachytherapy was initiated at 3–4 weeks after the commencement of EBRT. The median total dose at point A was 90 (range, 66–102) Gy. The median dose of EBRT at point A was 46 (range, 30–52) Gy. The median dose of HDR BRT at point A was 42 (range, 20–54) Gy.
Immunohistochemistry
For immunohistochemical detection of SOX2 and OCT4, 4-µm tissue sections were deparaffinized in xylene and subjected to microwave treatment (SOX2 for 20 min, OCT4 for 10 min at moderate intensity) in 0.01 M citrate buffer (pH 6.0). After cooling for 30 min and washing in PBS, endogenous peroxidase was blocked with 3% hydrogen peroxide for 30 min, followed by incubation with PBS containing 10% normal goat serum for 30 min. Specimens were incubated overnight at 4C with the anti-SOX2 (Santa Cruz Biotechnology Inc; Dallas, TX) (Ding et al. 2012) and anti-OCT4 (Cell Signaling Technology Inc.; Beverly, MA) (Pan and Thomson 2007) antibodies at a dilution of 1:100 and 1:200, respectively. Detection involving immunostaining was performed using the ChemMate Kit (Dako; Glostrup, Denmark) and 3,3-diaminobenzidine as the chromogen. In negative control staining, the primary antibody was replaced with nonimmune isotypic antibodies.
Evaluation of Staining
The stained tissue slides were viewed separately by two pathologists who were blinded to the clinical or clinicopathological status of the patients. The expression of SOX2 and OCT4 on the slides was evaluated by scanning the entire tissue specimen under low-power magnification (40×), and then confirmed under high-power magnification (400×). An immunoreactivity scoring system was used. The proportion of tumor cell staining was evaluated in terms of four grades: 0, no positive tumor cells; 1, <10% positive tumor cells; 2, 10−50% positive tumor cells; and 3, >50% positive tumor cells. The scoring criteria used for staining intensity were: 0, no staining; 1, weak staining; 2, modest staining; and 3, strong staining. The final score was calculated by multiplying the area of tumor staining by the intensity score (0, 1, 2, 3, 4, 6 and 9). According to this method of assessment, staining scores ≤4 and ≥6 were regarded as tumors with low and high expression, respectively (Chiou et al. 2008). We stained 132 blocks/tumors and, for each block, chose five random areas to obtain weighted scores according to the percentage of positive tumor cells and staining intensity at 400× magnification. Thus, we had five weighted scores for each block and the scores may be different for one patient. We selected the median weighted score from the five weighted scores as the typical score and these data were analyzed. Two pathologists scored all samples blindly, without knowledge of the clinical characteristics or prognosis.
Statistical Analysis
The relationships between SOX2 and OCT4 expression and the clinicopathological factors were analyzed using the Chi-square test or Fisher’s exact test. The radiation dose between the radiation-resistant and radiation-sensitive groups was estimated by the Student’s t-test. The relationships between SOX2 and OCT4 were analyzed using the Spearman-test. Survival curves were plotted using the Kaplan-Meier method, and differences between groups were assessed using the log-rank test. Univariate and multivariate survival analyses were performed according to the Cox proportional hazards model. SOX2 expression alone (high vs. low), OCT4 expression alone (high vs. low), both SOX2 and OCT4 high expression (yes vs. no), age (≥50 years vs. <50 years), FIGO stage (III + IVa vs. Ib +II), histopathological grade (middle + low vs. high), tumor diameter (>4 cm vs. ≤4 cm) and combined chemotherapy (platinum-based, no vs. yes) were included in the regression model. For all statistical tests, a p value ≤0.05 was considered statistically significant.
Results
Patient Clinical and Histopathological Characteristics
The clinical and histopathological characteristics of the patients enrolled in the study are detailed in Table 1. There were significant differences in tumor diameter, FIGO stage and histological grading between the radiation-resistant group and the radiation-sensitive group (p<0.001, p=0.004 and p<0.001, respectively). No significant differences were observed with respect to patient age, combined chemoradiotherapy (platinum-based), total dose at point A, EBRT dose at point A and BRT dose at point A between the two groups.
Patient Characteristics.
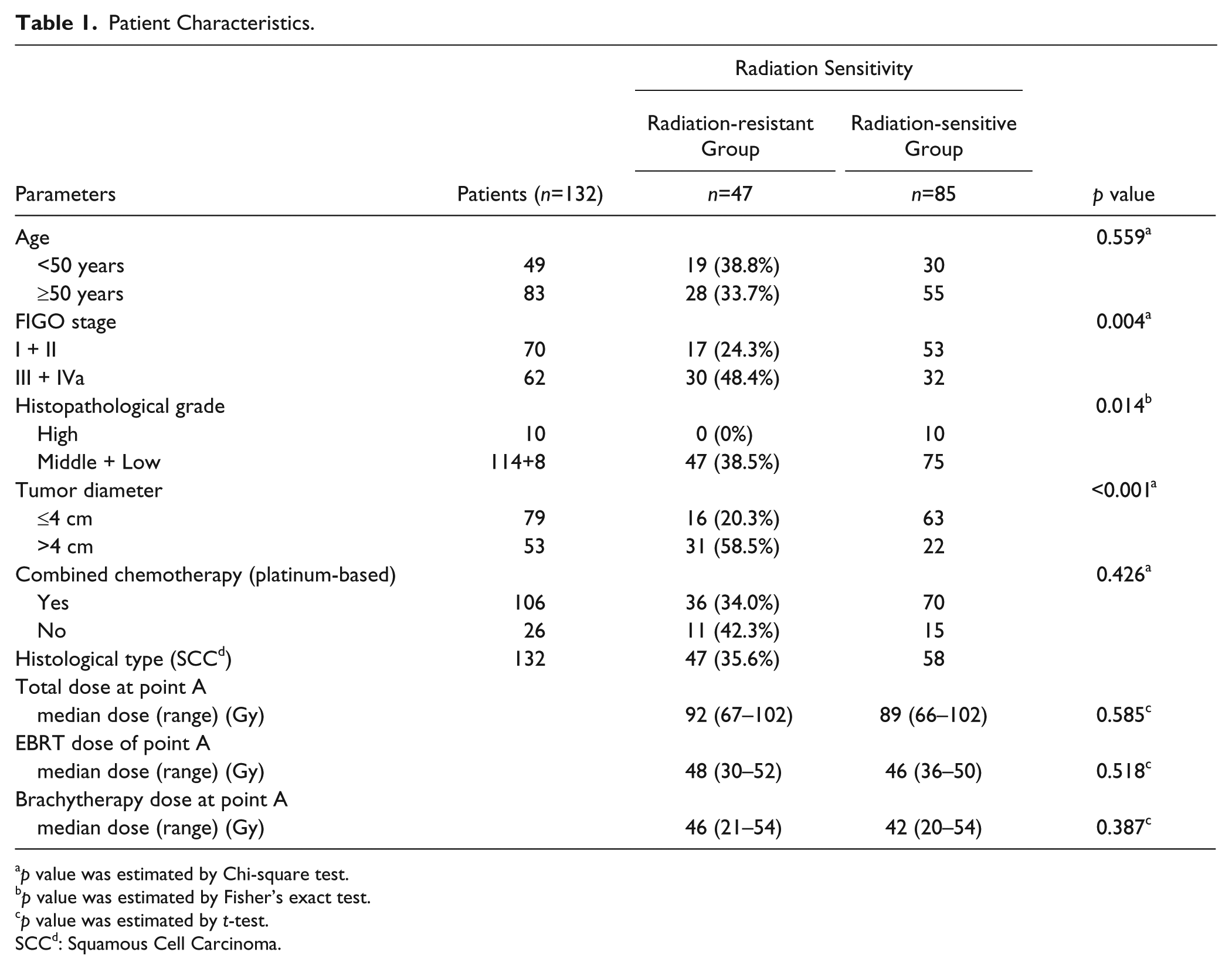
p value was estimated by Chi-square test.
p value was estimated by Fisher’s exact test.
p value was estimated by t-test.
SCCd: Squamous Cell Carcinoma.
SOX2 and OCT4 Expression and their Relationship to Clinicopathological Parameters
SOX2 was located in the nuclei of cervical carcinoma cells and staining was much stronger in the radiation-resistant group than in the radiation-sensitive group (Fig. 1A and 1C). Table 2 depicts the proportion of low and high expression of SOX2. No significant relationship was observed between SOX2 expression and patient age (p=0.944), FIGO stage (p=0.714), histopathological grade (p=0.845), or tumor diameter (p=0.177).
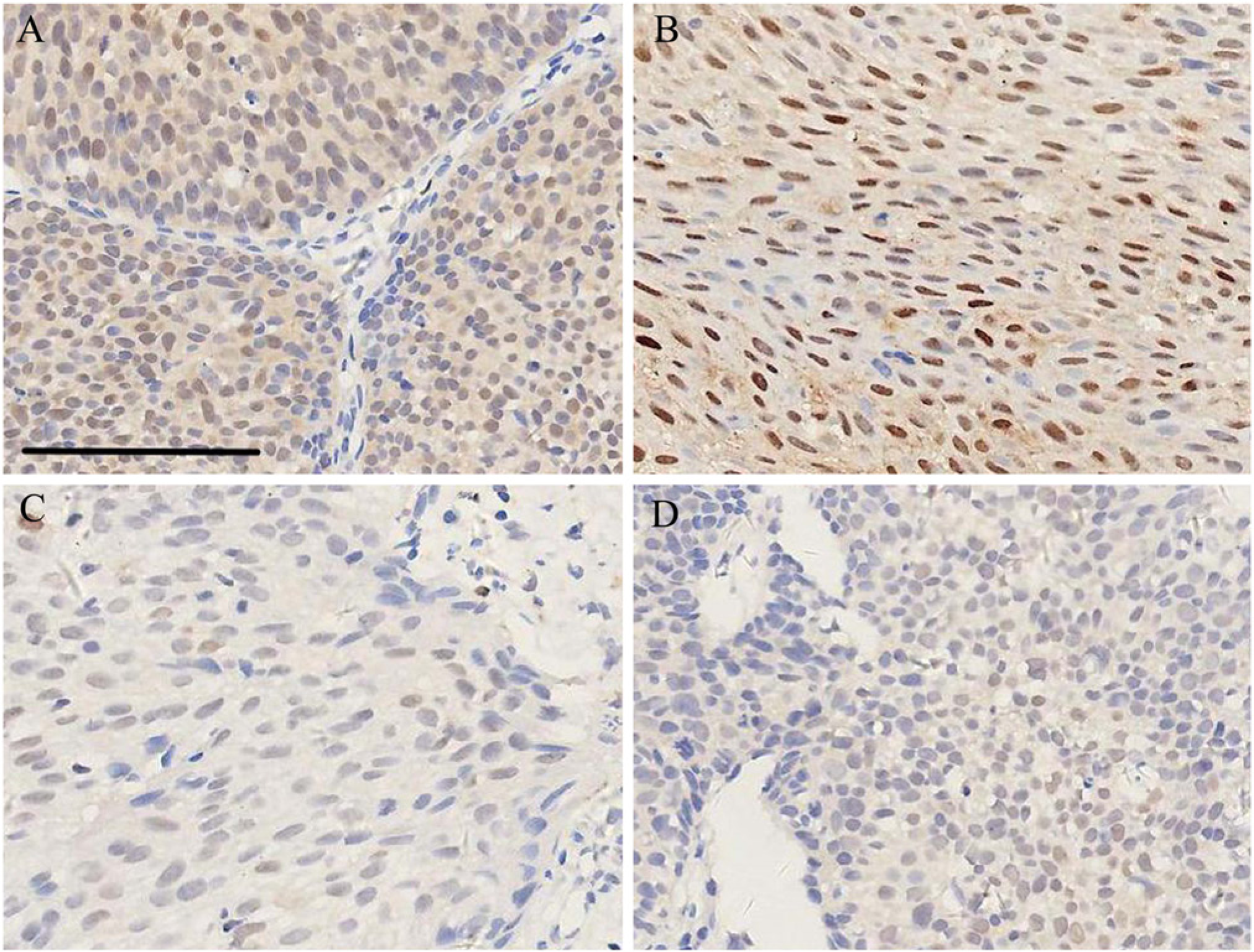
Representative examples of SOX2 and OCT4 staining of tumors in the radiation-resistant group and radiation-sensitive group (400×). (A) Strong positive staining of SOX2 in the radiation-resistant group. (B) Strong positive staining of OCT4 in the radiation-resistant group. (C) Weak positive staining of SOX2 in the radiation-sensitive group. (D) Weak positive staining of OCT4 in the radiation-sensitive group. The bar size is the same for all the figures. Scale bar, 90 µm.
Correlation between SOX2 and OCT4 Expression and Clinicopathological Parameters for Cervical Cell Squamous Carcinoma.
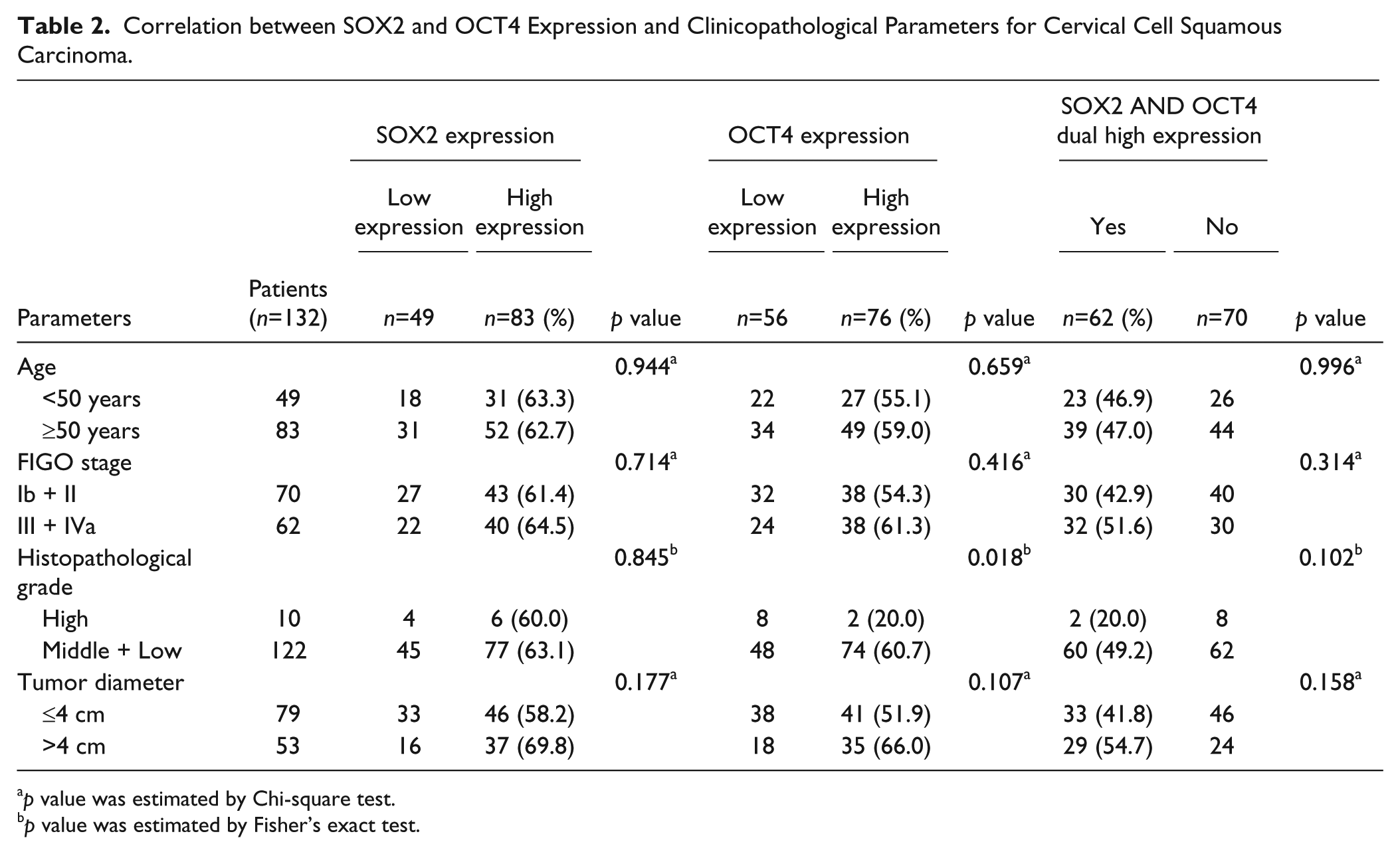
p value was estimated by Chi-square test.
p value was estimated by Fisher’s exact test.
OCT4 was also located in the nuclei of the cervical carcinoma cells, with staining much stronger in the radiation-resistant group than in the radiation-sensitive group (Fig. 1B and 1D). Table 2 depicts the proportion of patients with low and high expression of OCT4. A statistically significant relationship was observed between OCT4 expression and histopathological grade (p=0.018). However, no significant relationship was observed between OCT4 expression and patient age (p=0.659), FIGO stage (p=0.416) and tumor diameter (p=0.107).
In LACSCC patients, the proportion with low expression of SOX2 and/or OCT4 and high expression of both SOX2 and OCT4 is depicted in Table 2. No significant relationship was observed between SOX2 and OCT4 dual high expression and patient age (p=0.996), FIGO stage (p=0.314), histopathological grade (p=0.102) and tumor diameter (p=0.158).
Relationship between Expression of SOX2 and OCT4
In total, 132 qualified patients could be evaluated for SOX2 and OCT4 expression using immunostaining. Each marker was classified as low or high according to the degree of immunohistochemical staining (Table 3). A significant positive correlation was observed between SOX2 and OCT4 expression (r=0.483; p<0.001).
Expression of SOX2 and OCT4 in Cervical Squamous Cell Carcinoma Patients.
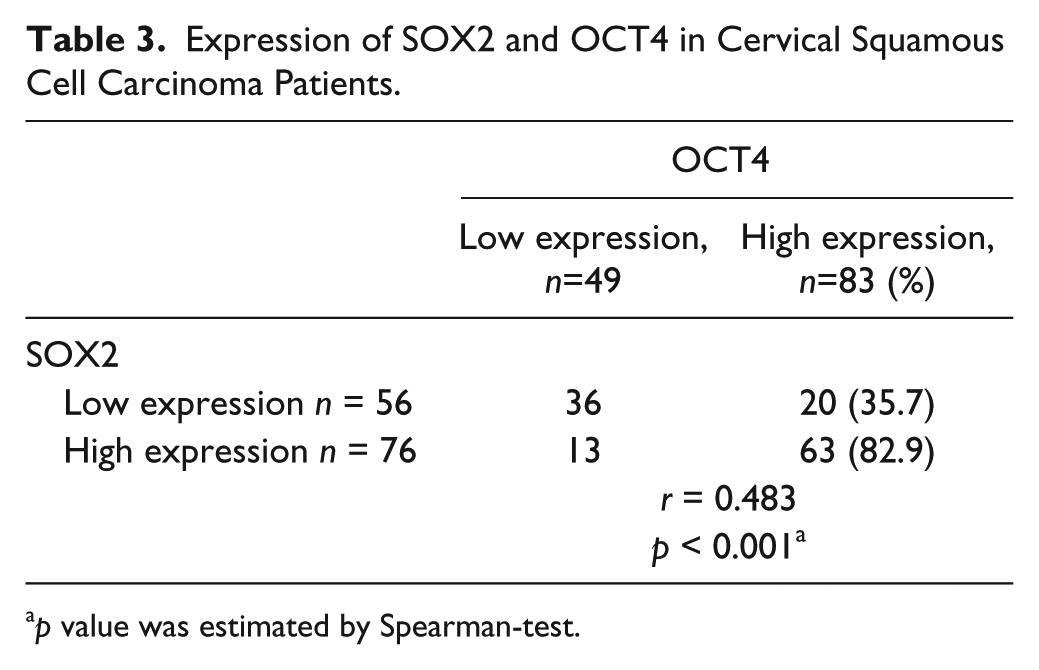
p value was estimated by Spearman-test.
SOX2 and OCT4 Expression and Response to Radiotherapy
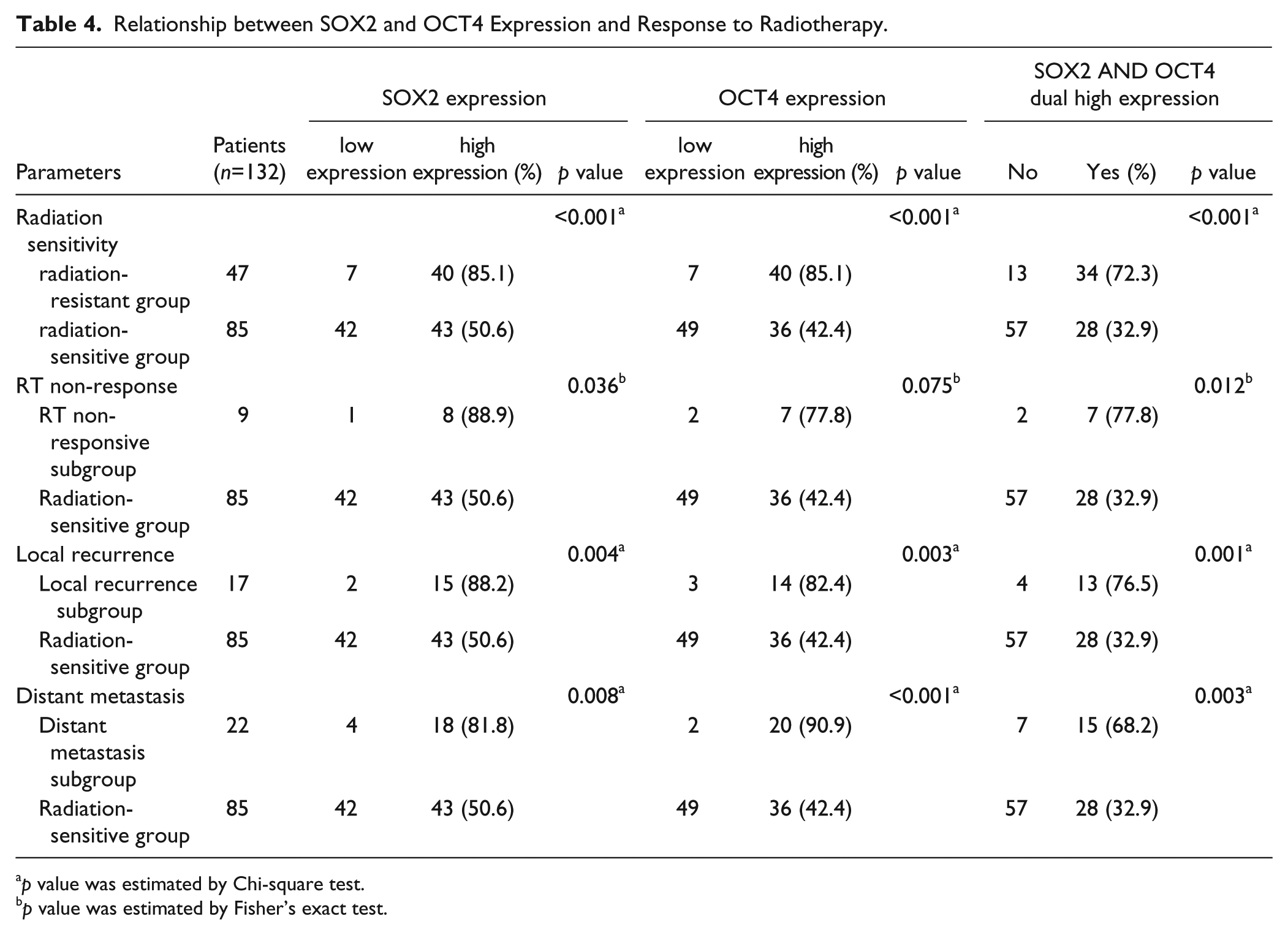
Data from SOX2 expression based upon the immunohistochemistry of 132 LACSCC patients are summarized in Table 4. Comparing the proportion of patients with high expression of SOX2 revealed statistically significant differences between the radiation-resistant and radiation-sensitive groups (p<0.001). The radiation-resistant group was further subdivided into three subgroups in accordance with the patient clinical information. A significant relationship was observed between SOX2 expression and RT non-response, local recurrence, and distant metastasis.
Relationship between SOX2 and OCT4 Expression and Response to Radiotherapy.
p value was estimated by Chi-square test.
p value was estimated by Fisher’s exact test.
Data from the immunohistochemical evaluation of OCT4 expression and SOX2 and OCT4 co-expression in LACSCC patients are also summarized in Table 4. There were also statistically significant differences among the groups.
SOX2 and OCT4 Expression and Patient Survival
As the patient cohort was stratified according to tumor expression of SOX2, the 5-year PFS rates in patients with low SOX2 expression (n=49) and high SOX2 expression (n=83) were 84.58% and 55.48 %, respectively; Kaplan-Meier analysis (log-rank test) revealed a significant difference between the two groups (p<0.001; Fig. 2A). With respect to OCT4 expression, the 5-year PFS rates in patients with low OCT4 expression (n=56) and high OCT4 expression (n=76) were 93.10% and 56.39%, respectively; Kaplan-Meier analysis (log-rank test) revealed a significant difference between the two groups (p<0.001; Fig. 2B).When the patient cohort was stratified according to the expression of both SOX2 and OCT4, the 5-year PFS rates were 80.01% and 50.91% in patients that showed low expression of SOX2 and/or OCT4 (n=70) and high expression of both SOX2 and OCT4 (n=62), respectively. It was noteworthy that patients who had tumors with high expression of both SOX2 and OCT4 had a worse prognosis than that of patients with low expression of SOX2 and/or OCT4 (Kaplan-Meier analysis; log-rank test; p<0.001; Fig. 2C). The 5-year PFS rate for all 132 patients was 66.79% (Fig. 2D).
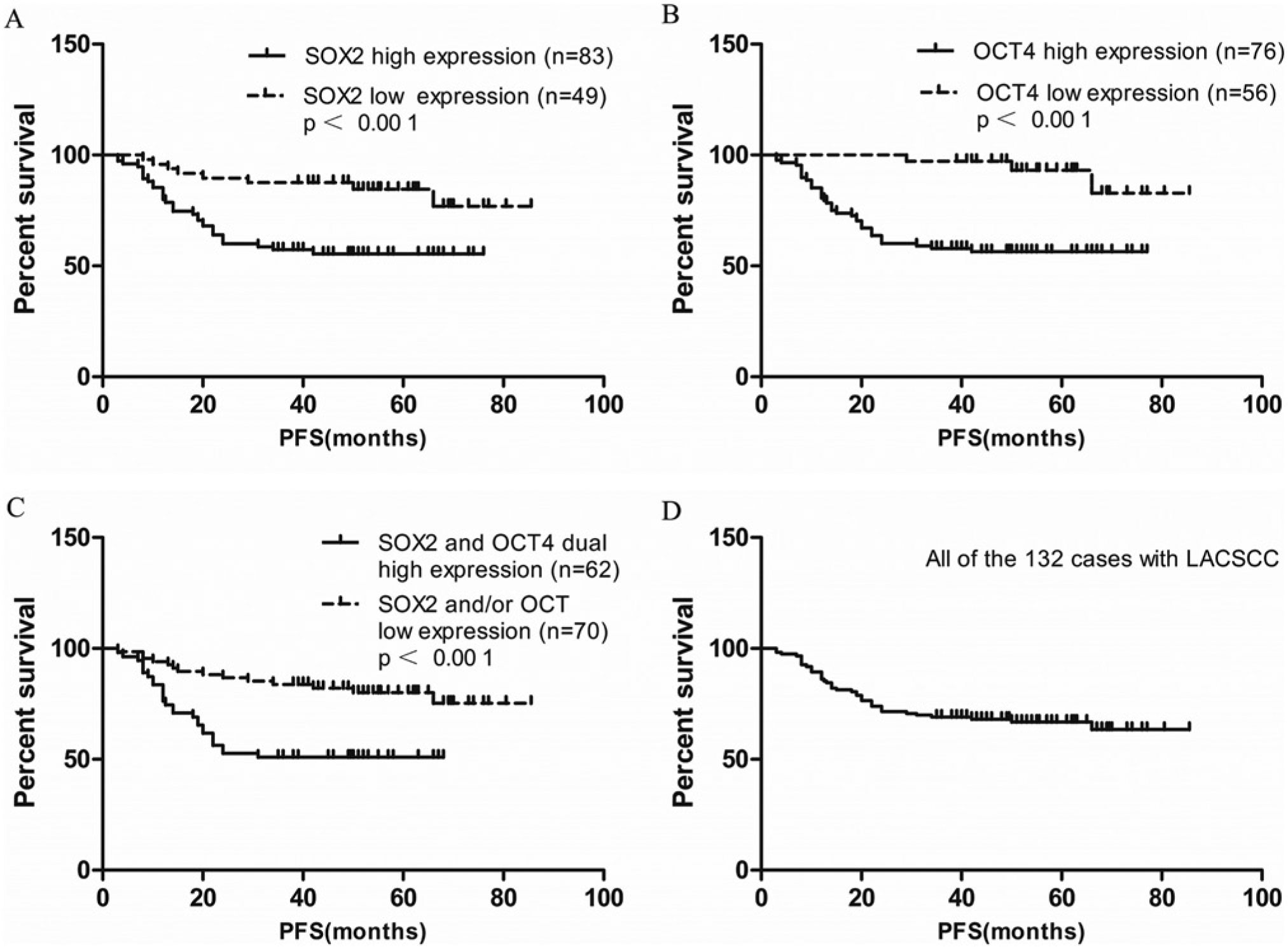
Kaplan-Meier survival curves for LACSCC patients. (A) The 5-year progression-free survival (PFS) rates were 84.58% and 55.48% in patients with low SOX2 expression (n=49) and high SOX2 expression (n=83), respectively. There was a significant difference in the overall survival rate between the two groups (p<0.001). (B) The 5-year PFS rates were 93.10% and 56.39% in patients with low OCT4 expression (n=56) and high OCT4 expression (n=76), respectively, with a significant difference in the overall survival rate between the two groups (p<0.001). (C) The 5-year PFS rates were 80.01% and 50.91% in patients that showed SOX2 and/or OCT4 low expression (n=70) and SOX2 and OCT4 dual high expression (n=62), respectively, with a significant difference in the overall survival rate between the two groups (p<0.001). (D) The 5-year PFS rate was 66.79% for all of the 132 patients with LACSCC.
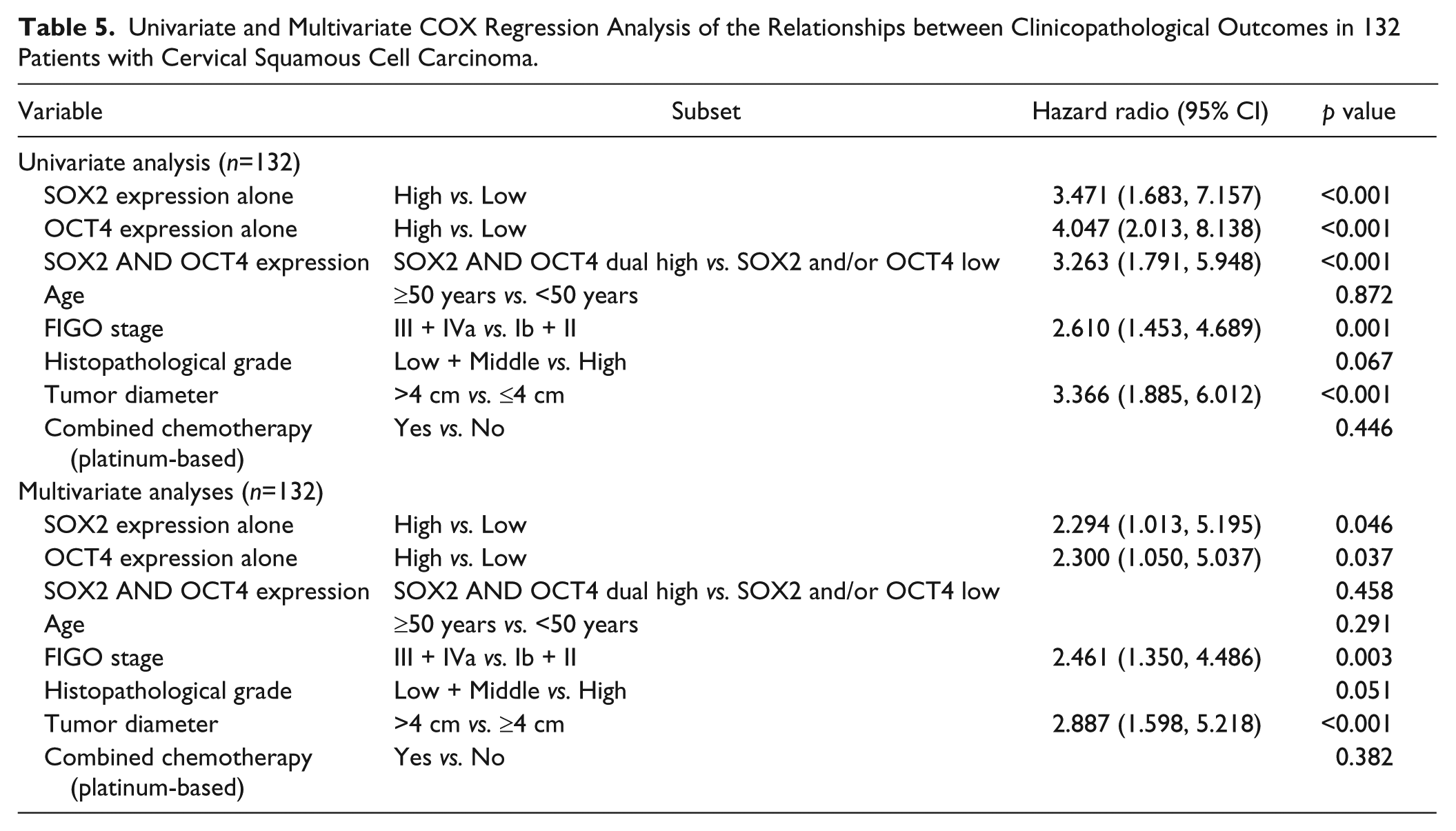
The univariate Cox regression analysis data for hazard ratios are depicted in Table 5. The multivariate Cox regression analysis data indicated that SOX2 and OCT4 co-expression was not an informative independent prognostic factor regarding our cohort of patients with LACSCC (Table 5). However, SOX2 alone and OCT4 alone had significant independent predictive value concerning PFS (Table 5). In addition, FIGO stage and tumor diameter were also independent prognostic predictors (Table 5).
Univariate and Multivariate COX Regression Analysis of the Relationships between Clinicopathological Outcomes in 132 Patients with Cervical Squamous Cell Carcinoma.
Discussion
By definition, one CSC has the potential to generate an entire tumor (Baumann et al. 2009), suggesting that all CSCs need to be inactivated for permanent local and distant tumor control after RT. RT that inactivates a high proportion of the non-CSC mass of tumor cells can lead to tumor regression and tumor growth delay without improving tumor control. However, RT that inactivates a high proportion of CSCs can improve tumor control. Increasing evidence suggests that CSCs have a higher radioresistance than non-stem cells from the same tumor (Saigusa et al. 2009). A number of mechanisms are involved in CSC-mediated tumor radioresistance (Krause et al. 2011), such as their intrinsic cellular radioresistance, especially regarding their ability to repair double-strand breaks (DSB) in DNA. Tumor radioresistance is also governed by CSC resistance to reactive oxygen species (ROS) (Diehn et al. 2009), the absolute number of CSCs before treatment (Yaromina et al. 2007), the repopulation capacity of CSCs between radiation fractions (Hessel et al. 2004) and microenvironmental factors such as hypoxia (Yaromina et al. 2010) and tumor lactate level (Sattler et al. 2010). These factors may interact and further increase tumor radioresistance mediated by CSCs.
SOX2 and OCT4 are essential transcription factors for the maintenance of pluripotent stem cells. The SOX2-OCT4 complex seems to be highly placed in the regulatory hierarchy of the pluripotent genetic network (Rodda et al. 2005). Furthermore, SOX2 and OCT4 are recognized CSC biomarkers in breast cancer. Thus, SOX2 and OCT4 play important roles in maintaining CSC biological behavior. For example, SOX2 silencing in glioblastoma tumor-initiating cells can stop proliferation and loss of tumorigenicity (Gangemi et al. 2009). Also, oncolytic adenovirus carrying OCT4 response elements in murine metastatic bladder cancer models can induce cytolysis (Wu et al. 2008).
Recent studies concerning cervical carcinomas indicate that CSCs confer a higher degree of tumor resistance to RT as compared with non-CSCs, and that SOX2 and OCT4 may be the CSC biomarkers. Lopez and coworkers (2012) showed that cancer-initiating cells derived from established cervical cell lines exhibited stem-cell markers and increased radioresistance. In another study, Feng and coworkers (2009) reported that primary cervical cancer contains a subpopulation of tumor-initiating cells with stem-like properties, and that SOX2 and OCT4 are the biomarkers for cervical carcinoma CSCs. The results from our study indicate that SOX2 and OCT4 were expressed significantly more strongly in the radioresistant group than in the radiosensitive group. Even when comparing the expression levels of SOX2 and OCT4 in the RT non-responsive subgroup, the local recurrence subgroup or the distant metastasis subgroup with those in the radiation-sensitive group, the statistical differences were also significant. Thus, we conclude that SOX2 and OCT4 play important roles with regard to LACSCC tumor radioresistance. In addition, high expression levels indicated a shorter PFS and an independent negative prognosis. Similar findings were reported in another study of rectal cancer (Saigusa et al. 2009), where SOX2 and OCT4 expression may be associated with tumor radioresistance and may predict distant recurrence and poor prognosis in rectal cancer patients treated with preoperative chemoradiotherapy.
Identification of the correlation between SOX2 and OCT4 may be an effective approach for elucidating the roles played by SOX2 and OCT4 in tumor radioresistance. In our study, a positive association between SOX2 and OCT4 was demonstrated. Although limited research has focused on the correlation between SOX2 and OCT4 in CSCs, some studies suggest that there is reciprocal transcriptional regulation of SOX2 and OCT4 via the SOX2/OCT4 complex in ESCs and that the function of SOX2 and OCT4 is dependent on this complex (Chew et al. 2005; Okumura-Nakanishi et al. 2005; Tomioka et al. 2002). Therefore, we assume that co-expression of SOX2 and OCT4 plays a more significant role than SOX2 alone or OCT4 alone. Although the co-expression of SOX2 and OCT4 was associated with a shorter PFS in our study, we found that this co-expression was not an informative independent prognostic factor regarding clinical outcomes, in contrast to the expression of SOX2 or OCT4 alone. It is possible that differences exist between the signaling pathways involved in CSCs and ESCs, or the numbers of the patients enrolled in our study were insufficient. Thus, further research is required here.
In summary, CSCs as a cause of local or distant relapse after RT are a potential therapeutic target. Treatment may be dependent on the presence of specific biomarkers because of the individualization treatment principle. SOX2 and OCT4 are suitable candidate biomarkers for patients with LACSCC, found in this study to be markers for tumor radioresistance and also independent negative prognostic factors. These findings require support from further research. First, retrospective clinical studies to evaluate SOX2 and OCT4 expression in pre-therapeutic biopsies across different centers will require sufficient samples for different cancers. Data from these studies will be important for predicting clinical outcomes and appropriate treatments. Second, in vitro studies are necessary to confirm the effect of radiotherapy in cell lines that highly express SOX2 and OCT4. SOX2 and OCT4 knockout models will also be useful here. Third, to address gaps in clinical observations and cell-based experimental data, in vivo radiobiological assays will be helpful in determining areas of tumor control after different radiation doses. These will be studied along with the frequency of tumorigenic CSCs as defined by specific phenotypic markers (SOX2 and OCT4) and functional features, including tumorigenicity, self-renewal and differentiation potential. If the biomarker profile is unfavorable, the therapeutic strategy for LACSCC may change. If favorable, we can detect inhibitors or antibodies targeted against these biomarkers, modulate the dose and frequency of fractionated radiotherapy, or even change the radioactive type (photon, proton, or carbon ion ray), according to the specific radiobiological characteristics of CSCs with high expression of these biomarkers. Certainly, we will consider the use of these markers as stratifiers in clinical trials.
Footnotes
Acknowledgements
We thank Professor Yang Lifang for advice and suggestions and Professor Yang Tubao for statistical guidance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by