
Abstract
Human leukocyte antigen-G (HLA-G) is a non-classical major histocompatibility complex class Ib molecule that acts as a specific immunosuppressor. Some studies have demonstrated that human papillomavirus (HPV) seems to be involved in lower or absent HLA-G expression, particularly in cervical cancer. In this study, we performed a cross-sectional study, systematically comparing the qualitative expression of the HLA-G5 isoform in invasive cervical carcinoma (ICC), stratifying patients according to the presence [ICC with metastasis (ICC
C
HLA-G expression may occur in normal tissues, including the placenta, where the molecule can protect the fetus against attack by the maternal immune system (Rouas-Freiss et al. 2005). On the other hand, HLA-G expression may occur in pathological states, as beneficial or deleterious depending on the condition involved. In transplantation and autoimmune disorders, HLA-G expression has been associated with a better prognosis, because the molecule may control the immune response against alloantigens or autoantigens. In contrast, HLA-G expression in virus-infected or malignant cells has been associated with tumor progression and metastasis (Carosella et al. 2003; Rouas-Freiss et al. 2005).
The expression of HLA-G in cancer was first described in melanoma cells (Paul et al. 1998), and the relationship between HLA-G expression and tumor progression has been a rapidly expanding field of cancer research, in which HLA-G expression has been observed in several tumor cells (Chen and Liao 2005; El-Chennawi et al. 2005; Adithi et al. 2006; Gros et al. 2006; Ishigami et al. 2006; Kleinberg et al. 2006; Rebmann et al. 2007; Ye et al. 2007; Yie et al. 2007) and at times used as a prognosis marker (Rouas-Freiss et al. 2007).
Overall, increased HLA-G expression in gynecological cancer cells has been associated with lesion progression, particularly in ovarian cancer (Sheu and Shih 2007) and endometrial adenocarcinoma (Barrier et al. 2006). However, the expression of the HLA non-classical molecule in premalignant and malignant cervical lesions caused by human papillomavirus (HPV) infection is increased in low-grade squamous intraepithelial lesions, later decreasing as the lesions progress to high-grade or invasive cancer (Zhou et al. 2006; Goncalves et al. 2008). In this study, we performed a cross-sectional study, systematically comparing the qualitative expression of the HLA-G5 isoform in invasive cervical carcinoma (ICC), stratifying patients according to the presence [ICC with metastasis (ICC
Materials and Methods
Specimens
The study protocol was approved by the Ethics Committee of the University Hospital, Faculty of Medicine of Ribeirão Preto, University of São Paulo (process #5507/06). This was a retrospective study (1994 to 2004) conducted on 79 human immunodeficiency virus (HIV)-1–negative patients exhibiting ICC without (ICC
The number of patients was apparently small because the archives (1994–2004) of the Faculty of Medicine of Ribeirão Preto and Campinas presented only 79 biopsies with ICC
All biopsies were reviewed and evaluated by two experienced histopathologists in a double-blind protocol. One cervical biopsy and one lymph node specimen obtained from each patient were embedded in paraffin blocks and stained with hematoxylin-eosin. Thin (5-μm) sections were cut, placed on organosilane-pretreated slides, and subjected to immunohistochemical assays (HLA-G5 isoform). Additionally, a 10-μm section was cut for DNA extraction and HPV typing.
Immunohistochemistry Assay for HLA-G5 Isoform
Sections of 5 μm were cut, placed on organosilane-pretreated slides, and subjected to immunohistochemical assay for the HLA-G5 isoform using the streptavidinbiotin system (LSAB; DAKO, Glostrup, Denmark). The cervical specimens were dewaxed in xylene, rehydrated in a graded alcohol series, and rinsed in water. For antigen retrieval, the sections were immersed in 10 mM sodium citrate buffer, pH 6.2. Endogenous peroxidase blocking was performed with three successive incubations of 15 min each in hydrogen peroxide plus absolute methanol. Nonspecific binding was performed with 3% low-fat dried milk diluted 1:100 in PBS. Slides were incubated with the primary monoclonal antibody (MAb) for the HLA-G5 isoform (5A6G7, diluted 1:50; EXBIO, Vestec, Czech Republic) in a humidified chamber at 4C overnight. Then slides were incubated with biotinylated anti-rabbit antibody and the streptavidin–peroxidase complex at 37C for 30 min. Finally, samples were incubated with 3,3-diaminobenzidine (DAB, Gibco; Gaithersburg, MD) diluted in 0.01% H2O2 for 10 min, lightly counterstained with Carrazzi's hematoxylin without acid for 60 sec, exhaustively rewashed with tap water, air dried, and mounted with Permount mounting medium (MERCK; Darmstadt, Germany). To validate the anti-HLA-G MAb and the immunohistochemical method, we systematically analyzed a paraffin-embedded section of trophoblastic tissue (positive control, Figure 1A). A negative control was prepared by omitting the primary antibody (Figure 1B). Basal HLA-G expression was evaluated in seven normal cervical biopsies from autopsies of previously healthy individuals who had died from violent trauma.
Qualitative Classification of HLA-G
All scoring and qualitative interpretation of immunohistochemical results were carried out by an experienced pathologist and classified as negative, discrete, moderate, or intense immunostaining. In the present study, we considered the expression of HLA-G to be low when no signal or discrete immunostaining was observed. HLA-G expression was classified as high when the pathologist observed moderate or intense immunostaining.
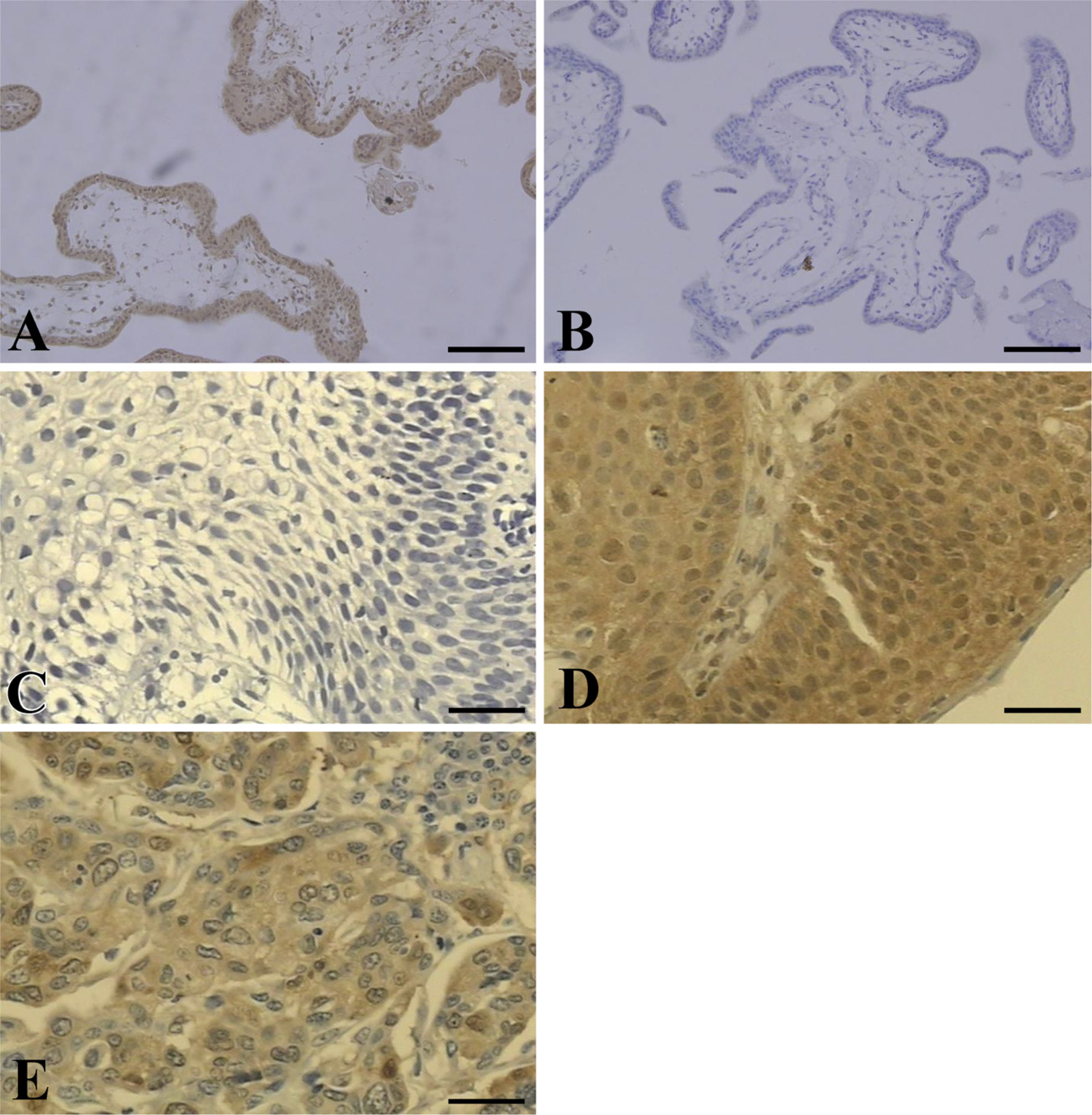
Human leukocyte antigen-G (HLA-G) expression in patients with invasive cervical carcinoma (ICC). Cervical biopsies obtained from patients according to the presence of ICC with metastasis (ICC
Quantitative Classification of HLA-G
Positive cytoplasm was automatically quantified by a computer-assisted system (Image-Pro Plus; Media Cybernetics, Inc., Bethesda, MD) consisting of a microscope, a digital camera, and a software package. A mean of ten random microscope fields were selected to analyze 1000 cytoplasm sites (HLA-G) per biopsy in all patient sections. The image acquisition of the sections of 79 patients (cervical lesion and lymph nodes with and without metastasis) was performed on an electron photomicrograph, and the image was processed and analyzed by the software. For each slide, the digitized image segmentation was controlled interactively by the red/green/blue color filter existing in the software program. The automatic cytoplasm count was established and expressed as percentage.
Qualitative classification of HLA-G expression in ICCs according to the presence or absence of lymph node metastasis

HLA-G, human leukocyte antigen-G; ICC, invasive cervical carcinoma; ICC
HPV Detection and Typing
Sections of 10 μm were cut from paraffin blocks and used for DNA extraction and HPV typing. HPV DNA obtained from paraffin blocks (Frank et al. 1996) was PCR amplified using 12.5 pmol of deoxynucleoside triphosphate, 25 pmol of each primer, 1.5 U Taq DNA polymerase (Gibco; Gaithersburg, MD), 5 μl of 10x enzyme buffer, 20 μg of genomic DNA, and distilled deionized H2O to complete a total volume of 25 μl. The mixture was processed in a thermocycler apparatus (MJ Research; Waltham, MA) under the following cycling conditions: 1 cycle at 95C for 5 min; 30 cycles at 95C for 30 sec, 55C for 30 sec, and 72C for 1 min, and finally, 1 cycle at 72C for 10 min, and then 4C indefinitely.
The primers GP5+ and GP6+ (Clifford et al. 2003), which amplify small DNA fragments (150 bp), were used for generic HPV amplification. The specific HPV-type amplification was performed with the set of primers HPV16E7.667/HPV16E7.774 for HPV-16, HPV18E7.696/HPV18E7.799 for HPV-18, HPV31E7.811/HPV31E7.890 for HPV-31, and HPV33E7.671/HPV33E7.761 for HPV-33 (Walboomers et al. 1999). All DNAs were amplified with a set of primers for a β-globin housekeeping gene (Saiki et al. 1988) as an internal control of amplification. The HPV positive control and beta-globin control were cervical biopsies that were tested for HPV DNA. For HPV-16 and HPV-18 controls, DNA was extracted from SiHa and HeLa cell lines, respectively, whereas HPV-31 and HPV-33 were from patient samples. All controls (HPV-16, −18, −31, and −33) were kindly provided by Dr. Luisa Lina Villa, Ludwig Institute for Cancer Research, São Paulo, Brazil. As a negative control, all PCR reagents were added to an Eppendorf tube containing no DNA sample. HPV-16, −18, −31, and −33 were chosen because they are most frequently associated with ICC. PCR amplicons were electrophoresed on 10% polyacrylamide gels at 200 V for 1.45 hr and stained with AgNO3 (Sanguinetti et al. 1994). It is important to note that the absence of HPV-16, −18, −31, or −33 did not exclude the presence of HPV types other than −16, −18, −31, and −33.
Statistical Analyses
Qualitative differences in HLA-G expression between groups determined according to clinical parameters were evaluated by means of the two-sided Fisher's exact test for 2 × 2 contingency tables, with the aid of the GraphPad InStat software (San Diego, CA), which was also used to estimate the odds ratio and its 95% confidence interval. Age, reported as arithmetic mean and standard deviation, was also compared between groups by means of the two-sided Student's unpaired t-test. The mean expression levels of HLA-G between ICC and metastatic cells of the draining lymph nodes were compared using the Wilcoxon matched-pair signed-rank test. Quantitative comparisons of HLA-G expression among groups were performed using the Mann-Whitney test. Correlations were calculated using the Spearman test. Statistical analyses were performed using the GraphPad Instat 3.05 software, with p values ≤0.05 considered to be significant.
Results
In the qualitative evaluation of the HLA-G5 isoform in all biopsies (n=79), HLA-G molecules were detected in only 25 patients (31.6%). In ICC
Quantitative immunoexpression of HLA-G in ICCs stratified according to presence or absence of lymph node metastasis
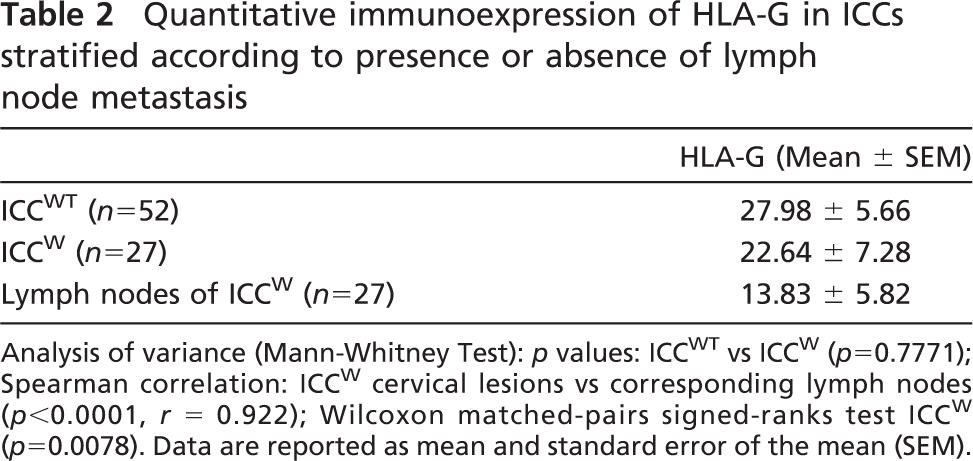
Analysis of variance (Mann-Whitney Test): p values: ICC
HPV DNA detection and typing in invasive cervical carcinomas stratified according to the presence or absence of lymph node metastasis

Normal cervical specimens obtained from healthy patients at autopsy (Figure 1C) and negative controls (Figure 1B) did not present any immunostaining in squamous cells, whereas the positive control (Figure 1A) showed specific immunostaining. In the patient sample, HLA-G expression was primarily detected in the cytoplasm of malignant cervical cells (Figure 1D) and in lymph node metastatic cells (Figure 1E).
In the quantitative analysis of the ICC
HPV Detection and Typing
HPV DNA was detected in 74 of 79 (93.7%) specimens analyzed. In the ICC
HLA-G5 Isoform Expression According to Demographic and Clinical Variables
No significant associations were observed regarding HLA-G expression in relation to age, alcohol use, and smoke exposure. However, the patients were predominantly not exposed to tobacco or alcohol (Table 4).
Discussion
Tumor cells can efficiently evade the antitumor immune response by modulating antigen expression, producing immunosuppressive cytokines, or inducing peripheral tolerance (Smyth et al. 2006). Tumor cells that have lost classical HLA molecules that are important for immune recognition tend to express the immune-tolerant HLA-G molecule on their cell surfaces (Rouas-Freiss et al. 2005). Cancers of different origin show preferential upregulation of HLA-G in advanced disease, rather than in the initial tumor lesions, supporting its tolerogenic role in the final phase of immunoediting (Urosevic and Dummer 2008).
In this study, we reported that HLA-G expression was low in cervical cancer specimens. Therefore, HLA-G expression in tumor cells may vary according to the type of cancer. A recent study stratified tumors according to the magnitude of HLA-G expression, i.e., lesions exhibiting no expression, less than 30% expression, and more than 30% expression (Carosella et al. 2008). Among some tumors affecting women, ovarian carcinoma expressed HLA-G in 61% of specimens (45/74) (Sheu and Shih 2007), endometrial adenocarcinoma in 55% (24/44) (Barrier et al. 2006), and breast cancer in 39% (14/36) (Lefebvre et al. 2002).
In the present study, concerning the immunological response, the loss of HLA class I molecules was consistently related to the occurrence of cervical lesions. We hypothesize that, similarly to other viral models, HPV infection may downregulate major histocompatibility complex class I molecules. Although definitive evidence of HPV influence on these cancers is not available, HPV infection is the hallmark in cervical cancer (Clifford et al. 2003; Fule et al. 2006), and HPV DNA was observed in patients of this series. Whether HPV is implicated in the magnitude of HLA-G expression remains to be elucidated; however, it is possible that HPV may be involved in the modulation of HLA-G surface expression, because it has been reported that high-risk HPV oncoproteins may inhibit the promotor gene of HLA class I heavy chain and may modulate latent membrane protein-2 and transporter associated with antigen processing-1 (TAP-1) proteins, responsible for processing and transporting peptides into the groove of HLA class I molecules (Georgopoulos et al. 2000). In addition, HPV E5 protein may downregulate HLA class I molecules by retaining HLA class I heavy chain in the Golgi complex (Ashrafi et al. 2002, 2005). It is also interesting to observe the behavior of HLA-G expression in HPV-associated cervical lesions. HLA-G expression appeared in atypical glandular cells of undetermined significance and progressively decreased from cervical intraepithelial neoplasia-1 (CIN1) to CIN2–3 and ICC (Goncalves et al. 2008).
Demographic and epidemiologic findings observed in HLA-G–positive patients with ICC stratified according to presence or not of lymph node metastasis
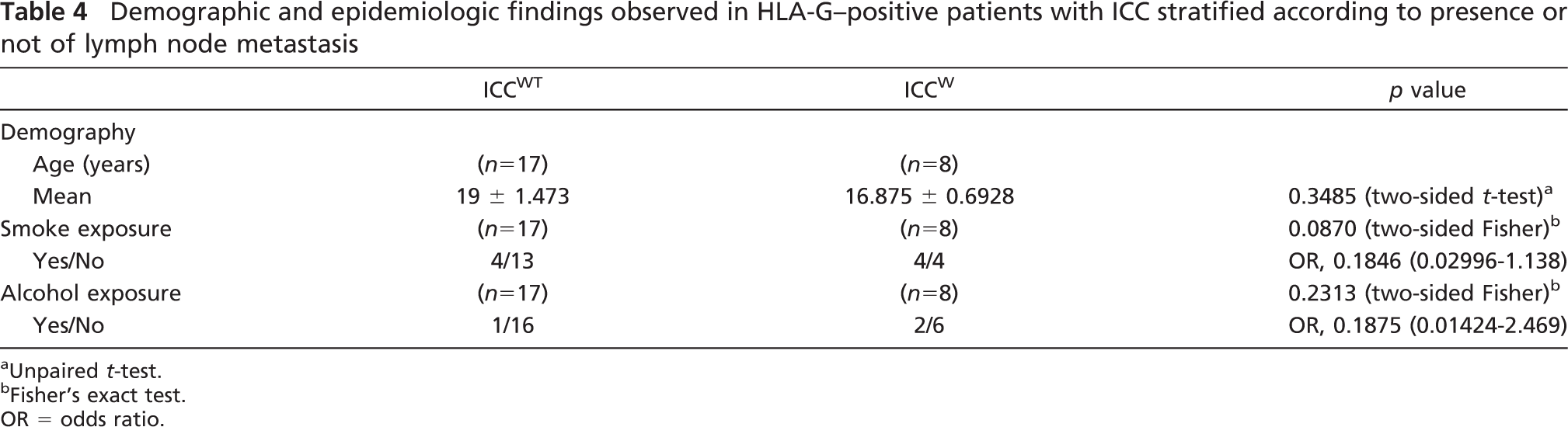
Unpaired t-test.
Fisher's exact test.
OR = odds ratio.
Several mechanisms have been proposed to explain the immunomodulatory effects of HLA-G in cancer. HLA-G may induce Th2 cytokine (IL-4, IL-5, IL-10) polarization, which is not effective on viral depletion (Nakanishi et al. 2001), permitting viral maintenance and lesion progression (Clerici et al. 1997; Nguyen et al. 2005). In our findings, low expression of HLA-G in cervical invasive lesions was observed, as demonstrated in Goncalves et al. (2008). Perhaps the genetic alterations of cervical invasive lesions could modify HLA-G expression in cancer cells in different tumor types (Carosella et al. 2008).
Particularly in cervical cancer, low expression of HLA-G could be attributed to other factors, such as genetic mutations in only one HLA allele in the 6p2.3 region (Vermeulen et al. 2005). Premalignant and malignant cervical lesions may originate from the same clonal process; therefore, the loss of HLA-G expression could be an initial event in cervical carcino-genesis (Vermeulen et al. 2005), and the loss of heterozygosis in the TAP region could cause failure of the transport of the HLA-G molecule (Vermeulen et al. 2007).
Overall, it remains to be determined why some cervical cancer patients express HLA-G, whereas others do not. These findings are important; however, additional studies are necessary to identify the influence of HPVon HLA-G5 isoform expression in invasive cervical malignancies.
In conclusion, further studies are needed to clarify the molecular aspects of the relationship between HLA-G expression and HPV infection, with potential applications for cervical cancer prediction.
Footnotes
Acknowledgements
This study was supported by grants from Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES-PROCAD # 0210/05–6) and Fundação de Apoio ao Ensino, Pesquisa e Assistencia (FAEPA) HCFMRP-USP. M.C.M.G. was supported by a doctoral fellowship from CAPES/Brazil.
We thank Ana Maria Rocha for excellent technical assistance.