
Abstract
A retrospective study of cases of a unique intramural inflammatory mass within the feline gastrointestinal tract was performed in order to describe and characterize the lesion. Twenty-five cases were identified from archival surgical and postmortem tissues. The lesion most often occurred as an ulcerated intramural mass at the pyloric sphincter (n = 12) or the ileocecocolic junction or colon (n = 9); the remaining cases were in the small intestine. Seven cases also had lymph node involvement. The lesions were characterized by eosinophilic inflammation, large reactive fibroblasts, and trabeculae of dense collagen. Intralesional bacteria were identified in 56% of the cases overall and all of the ileocecocolic junction and colon lesions. Fifty-eight percent of cats tested had peripheral eosinophilia. Cats treated with prednisone had a significantly longer survival time than those receiving other treatments. We propose that this is a unique fibroblastic response of the feline gastrointestinal tract to eosinophilic inflammation that in some cases is associated with bacteria. The lesion is often grossly and sometimes histologically mistaken for neoplasia.
There are several conditions in cats in which eosinophilic inflammation is the predominant feature, including feline indolent ulcer, eosinophilic plaque, eosinophilic granuloma, and hypereosinophilic syndrome. 2, 8 In this report we describe another feline eosinophilic lesion that appears to be limited to the gastrointestinal tract and associated lymph nodes. The typical presentation is an ulcerated intramural mass at the pyloric sphincter or ileocecocolic junction. A previous report of similar lesions in the subcutis and abdomen of cats in Japan proposed methicillin-resistant Staphylococcus as the cause. 14 In the cases reported here, the lesions are restricted to the gastrointestinal tract and associated lymph nodes, and all have a very characteristic trabecular pattern of dense collagen that resembles osteoid, sometimes leading to a mistaken diagnosis of osteosarcoma. Many cases also contain numerous mast cells, leading to the diagnosis of sclerosing mast cell tumor. The goal of this report is to further characterize this lesion, suggest a pathogenesis, and propose the term “feline gastrointestinal eosinophilic sclerosing fibroplasia” for the lesion.
Materials and Methods
Case selection
Cases were selected during 2005–2008 based on histologic appearance from the biopsy and necropsy submissions to the Department of Pathobiology at the University of Tennessee, College of Veterinary Medicine (9 cases), IDEXX Laboratories (8 cases), Marshfield Laboratories (7 cases), and Antech Diagnostics (1 case). Referring veterinarians were contacted and medical records were reviewed to collect signalment, history, clinical laboratory findings, surgical findings, and outcome information.
Cytopathology
Cytopathologic samples were obtained from 5 cats (cats 9, 11, 12, 14, and 15) by ultrasound-guided fine-needle aspirate or impression of tissue taken during surgery. All slides were stained with modified Wright's.
Histopathology
Tissue samples were fixed in 10% formalin, embedded in paraffin, and stained with HE. Selected tissue sections were also stained with Gram stain, Gomori's methenamine silver, Fite-Faraco, Toluidine blue, and/or modified Steiner's.
Immunohistochemistry
Selected slides were stained by immunohistochemistry. Antigen retrieval consisted of 25 minutes at 95°C in a pH 9.0 ethylenediaminetetraacetic acid (EDTA) buffer. A 3% hydrogen peroxide block was applied for 5 minutes, and this was followed by a 5-minute nonserum protein block. Monoclonal antibodies to smooth muscle actin (Dako, Carpinteria, CA) at a 1 : 1,000 dilution and vimentin (Dako) at a 1 : 8,000 dilution were applied and incubated for 30 minutes. A polymer-based detection kit (EnVision, Dako) and 3,3-diaminobenzidine chromagen were applied. Slides were counterstained with Mayer's hematoxylin.
Data analysis
Survival time was measured from the date of diagnosis. The Kaplan-Meier procedure (PROC LIFETEST, SAS version 8.0, SAS Institute, Cary, NC) was used to compute nonparametric estimates of the survivor function and compare survival curves in order to evaluate the association of survival time with treatment and location of the lesion. Cats were right censored if they were lost to follow-up or were alive when the study was terminated.
Results
The signalment, presenting signs, sites affected, and outcome are summarized in Table 1. The breeds included 14 domestic shorthair, 4 domestic longhair, and one each of the following: mixed breed, Siamese, Siamese cross, Maine Coon cat, Maine Coon cat cross, Himalayan, and exotic shorthaired Persian. The ages ranged from 14 weeks to 16 years, with a mean of 8.8 years ± 4.4 SD. Eighteen were neutered males (72%) and 7 were spayed females (28%). The cases were submitted by veterinarians in Tennessee, Florida, Maryland, Pennsylvania, New Jersey, Massachusetts, Wisconsin, and Minnesota.
Summary of clinical presentation, pathologic findings, and outcomes in 25 cats. ∗
FS = female spayed; MN = male neutered; DSH = domestic shorthair; DLH = domestic longhair; U = unknown; LN = lymph node; LTF = lost to follow-up.
Vomiting was the most common presenting sign (21/25, 84%), but there was wide variation in duration, from days to years. Weight loss was the second most common presenting sign (15/22, 68%). Peripheral hypereosinophilia was detected in 7 of the 12 cats (58%) on which bloodwork was performed. Three cats had biliary obstruction with hyperbilirubinemia and elevated serum enzymes suggestive of hepatocellular damage. Of the 7 cats tested for feline leukemia virus, all were negative. Of the 7 cats tested for feline immunodeficiency virus, 5 were negative and cats 13 and 16 were positive.
All cases had a palpable abdominal mass. Grossly, an intramural ulcerated mass at the pyloric sphincter was the most common lesion (n = 12, 48%), which was often considered surgically nonresectable. Other intramural sites included jejunum (n = 2), small intestine (not otherwise specified, n = 1), ileum (n = 1), ileocecocolic junction (n = 6), and colon (n = 3). Seven cats also had gross lymph node enlargement.
Cytology was performed in 5 cats (cats 9, 11, 12, 14, and 15). In cat 9, tissue imprints and fine-needle aspirates (FNAs) were taken during surgery of the pyloric sphincter mass. Large irregular to spindle-shaped cells, pink extracellular matrix, numerous eosinophils, and numerous neutrophils were present (Fig. 1). Neutrophils occasionally contained intracytoplasmic bacterial rods and cocci, and extracellular bacteria were scattered throughout the background. Also seen were occasional small to intermediate-sized lymphocytes, occasional plasma cells, and few degranulated mast cells. Ultrasound-guided FNA of the pyloric mass in cat 11 had similar findings. In cat 12, tissue imprints taken during surgery were inconclusive because of low cellularity, but the abdominal effusion in this cat was characterized as an inflammatory exudate with 20% eosinophils. In cats 14 and 15, FNA of the mass showed only increased numbers of eosinophils.
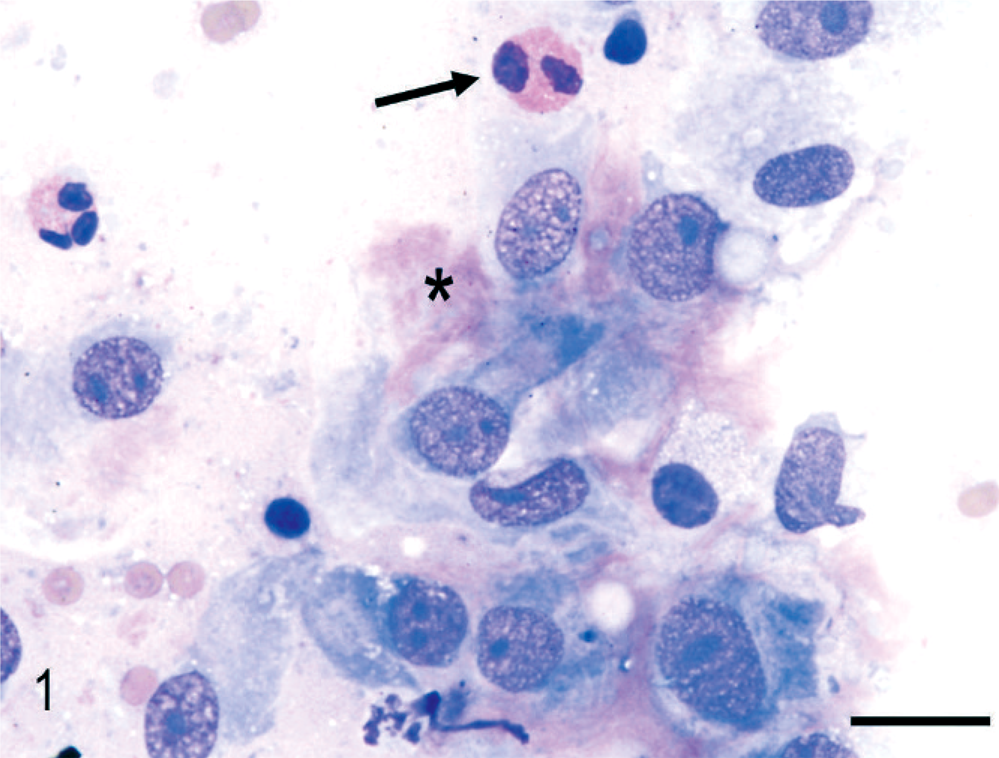
Cytology of duodenal mass; cat 9. An aspirate of the duodenal mass showing large spindle-shaped cells, pink extracellular matrix (∗), and eosinophils (arrow). Wright's. Bar = 20 µm.
The histopathologic appearance of the typical intestinal lesion was of an ulcerated mass expanding the wall at the pyloric sphincter/proximal duodenum (n = 12, Fig. 2) or ileocecocolic junction (n = 9, Fig. 3). Lymph nodes were also commonly affected (n = 7), either by the same sclerosing lesion as in the intestine (Fig. 4) or by eosinophilic lymphadenitis with more typical fibrosis. The pancreas was extensively infiltrated by eosinophils and fibroblasts in one cat (cat 12), which also had extensive infiltration of the wall of the common bile duct and a ruptured gall bladder.
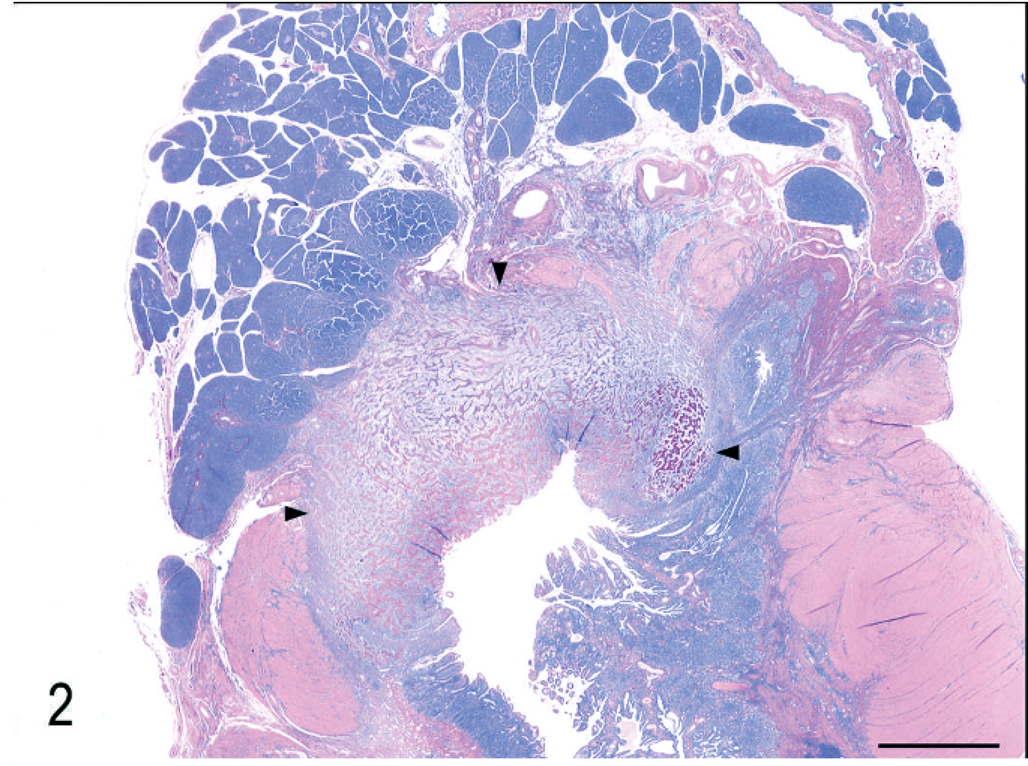
Duodenum and pancreas; cat 7. An ulcerated lesion (outlined by arrowheads) expands and replaces the intestinal wall at the junction of the pylorus and duodenum. Dense collagen trabeculae are present throughout the lesion. HE. Bar = 5 mm.
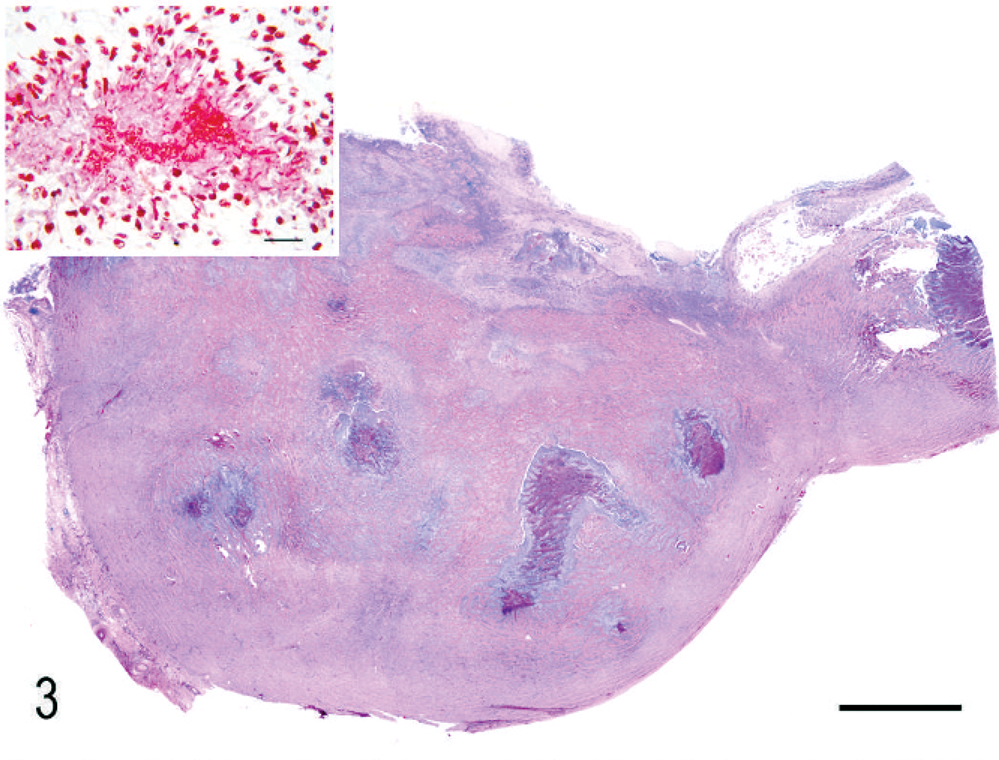
Ileocecocolic junction; cat 21. An ulcerated mass of fibroplasia with dense collagen trabeculae (sclerosing fibroplasia) expands and replaces the intestinal wall. There are multiple necrotic foci and microabscesses containing bacteria within the mass. HE. Bar = 3 mm. Inset: Gram stain of short Gram-negative rods within a microabscess. Bar = 20 µm.
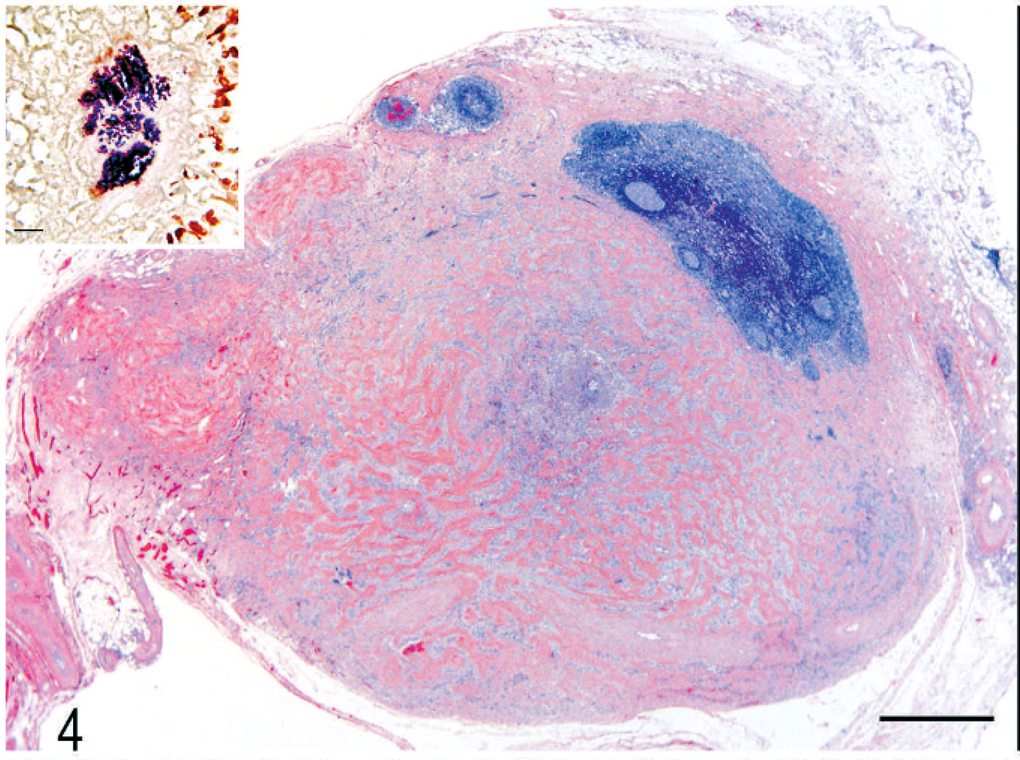
Lymph node; cat 5. Most of the lymph node is effaced by dense collagen trabeculae (sclerosing fibroplasia) surrounding a central microabscess. HE. Bar = 500 µm. Inset: Gram-positive cocci at the center of the microabscess. Gram stain. Bar = 20 µm.
All lesions consisted of branching and anastomosing trabeculae of dense collagen separated by a densely cellular population of large spindle-shaped cells. The trabecular collagen merged gradually into more typical granulation tissue at the periphery of the lesions (Fig. 5). All lesions contained variably dense infiltrates of eosinophils, mast cells, and fewer neutrophils, lymphocytes, and plasma cells within the fibroplasia (Fig. 6) as well as within the surrounding tissues. Lesions were either transmural (Fig. 3) or affected the inner layers of the gastrointestinal wall (Fig. 1). The lesions did not extend beyond the serosa, except to involve pancreas or lymph nodes. Increased numbers of eosinophils, lymphocytes, and plasma cells were noted in unaffected portions of the intestines in 3 cats (cats 14, 17, and 19). Increased numbers of globule leukocytes were noted in the adjacent mucosa in 3 cats (cats 4, 11, and 12).
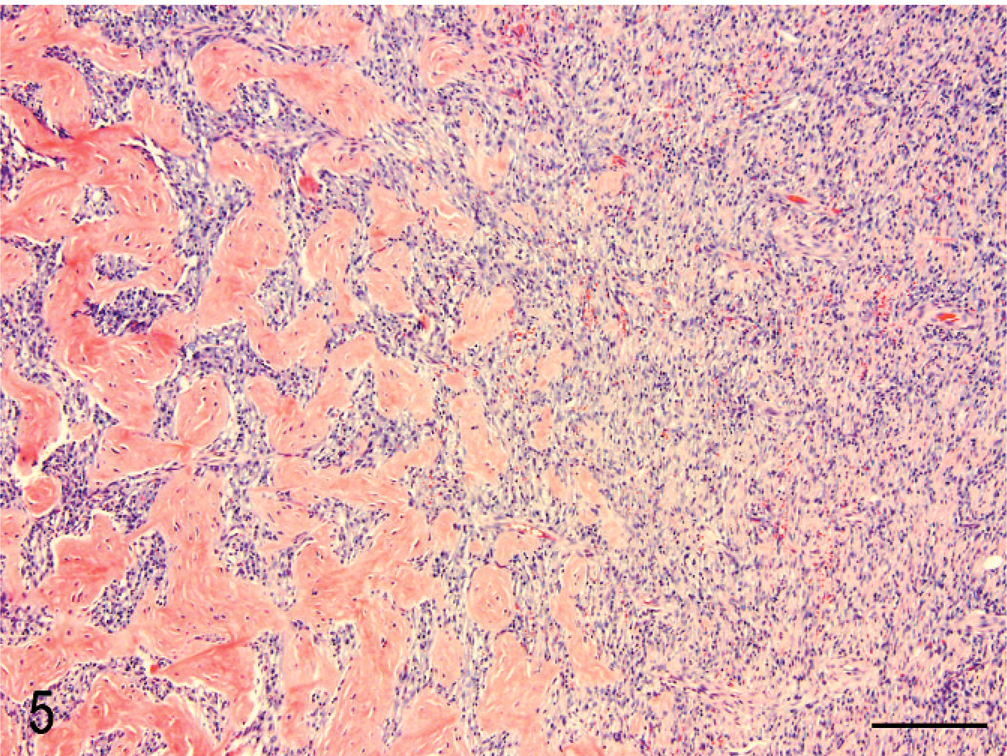
Duodenum; cat 12. Trabeculae of dense collagen separated by large spindle-shaped cells (sclerosing fibroplasia) merges into more typical granulation tissue at the periphery of the lesion. HE. Bar = 200 µm.
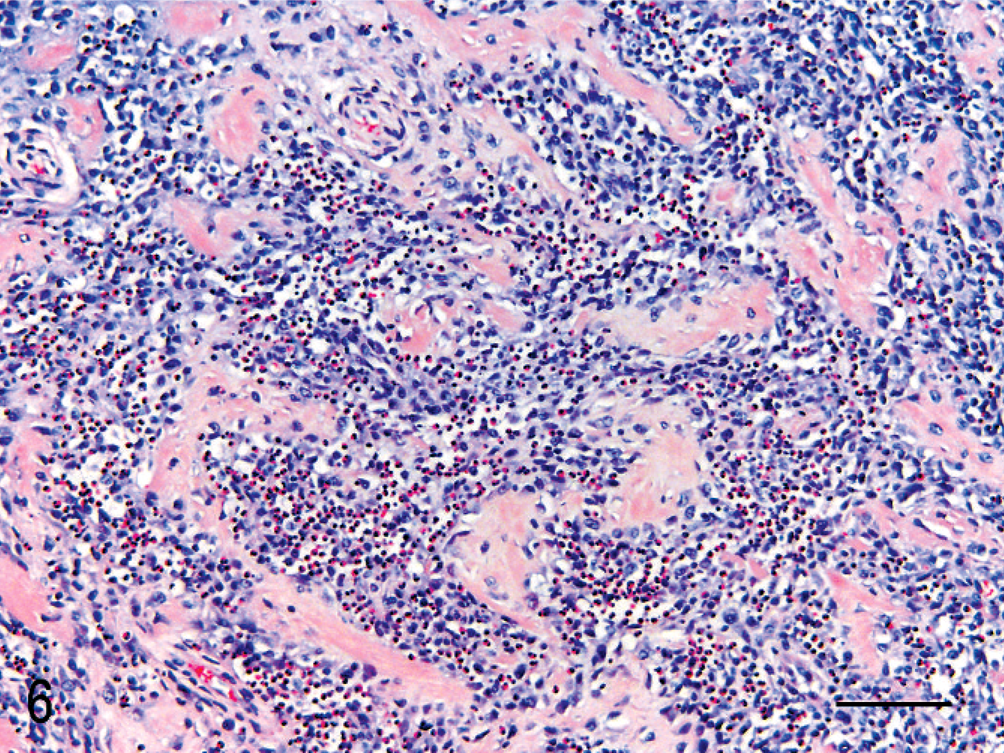
Duodenum; cat 10. Eosinophils are numerous within the fibroblastic portion of the lesion. HE. Bar = 100 µm.
In 14 cats (56%), bacterial colonies were present within microabscesses and necrotic foci within the lesion. The bacteria included Gram-negative rods, Gram-positive rods, and Gram-positive cocci (Table 1). In the cats with intralesional bacteria, the dense collagen trabeculae formed irregular radiating and concentric bands around central microabscesses containing the bacteria (Figs. 2 and 3, insets). Some cases were also stained with modified Steiner, Gomori's methenamine silver, and/or Fite-Faraco, but no spirochetes, fungi, or acid-fast bacteria were detected. Culture taken at necropsy of an affected mesenteric lymph node from cat 22 was negative. The mural mass in cat 9 was cultured during surgery and 6 colonies of Escherichia coli and 2 colonies of Clostridium perfringens were grown. Both organisms were sensitive to all antibiotics tested.
By immunohistochemistry (cat 9) the large spindle cells were uniformly positive for vimentin and smooth muscle actin (not shown) indicating myofibroblastic differentiation. The spindle-shaped cells showed variable degrees of mitotic activity and nuclear pleomorphism. Five cats were originally diagnosed with sclerosing mast cell tumors (cats 6, 18, 21, 24, and 25), two cats were originally diagnosed with osteosarcoma (cats 3 and 7), and one cat was originally diagnosed with a hematopoietic neoplasm (cat 16). The remaining 17 cats were diagnosed with eosinophilic inflammatory lesions.
Three cats (cats 4, 20, and 21) were treated by surgical biopsy only; cats with the more aborad masses (cats 20 and 21) had complete excision and longer survival than cat 4, at the pyloric sphincter. Eight cats (cats 5, 7, 8, 11, 12, 16, 22, and 23) were treated with surgical biopsy and antibiotics; 7 of those died or were euthanatized for continued clinical signs. Seven cats were treated with surgical biopsy and prednisone (cats 2, 6, 9, 14, 17, 19, and 25). Cats 6, 14, and 17 were also treated with antibiotics. Cat 9 was also treated with montelukast sodium (Singulair, Merck, Rahway, NJ) and famotidine (Pepcid, Rahway, NJ). Of the 7 cats treated with prednisone, 5 were alive at the time of this writing; 2 survived 6 weeks and 4 months after surgery, and then were lost to follow-up. The treatment was unknown in 7 cats (cats 1, 3, 10, 13, 15, 18, and 24).
Survival curves comparing treatment with surgical biopsy and prednisone (with or without antibiotics), treatment with surgical biopsy and antibiotics, and treatment with only surgical biopsy are shown in Fig. 7. Mean survival time for cats treated with antibiotics was significantly (P = .02) shorter than for cats treated with prednisone; however, the mean and standard error of the mean for cats treated with prednisone or surgical biopsy alone could not be calculated, as all but one of the cats in these groups were censored (alive or lost to follow-up).
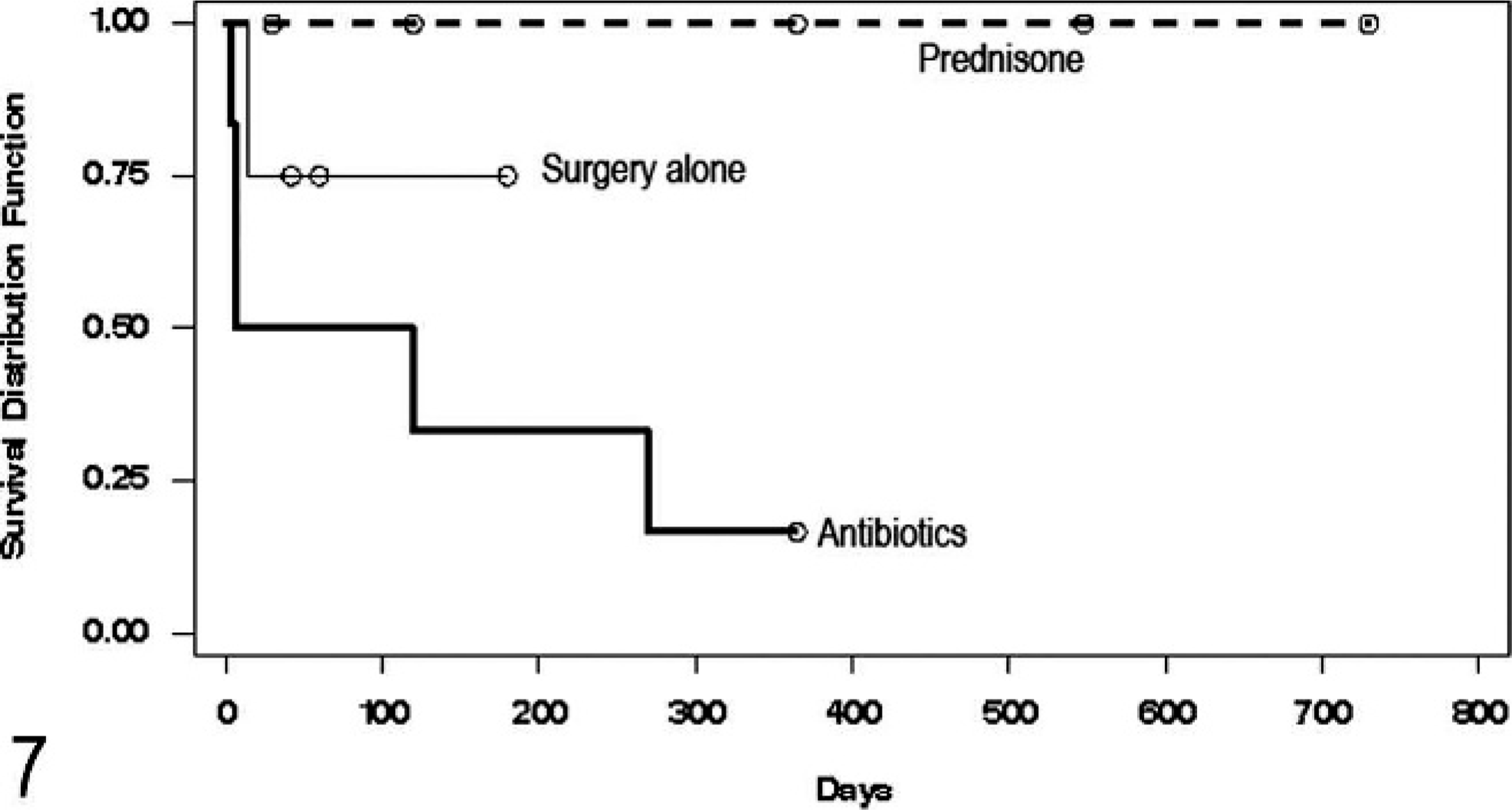
Comparison of survival between cats treated with prednisone, cats treated with surgical biopsy alone, and cats treated with antibiotics. The survival time was significantly shorter for cats treated with antibiotics (P = .02). ○ = censored data point (cat still alive or lost to followup).
Ten cats were euthanatized (40%); 6 of those were euthanatized during surgery due to the nonresectable or neoplastic appearance of the mass. The other 4 were euthanatized due to persistent vomiting and weight loss. Four cats died spontaneously. Cat 3 died of hypertrophic cardiomyopathy but had a 5-year history of vomiting. Cat 10 died of peritonitis secondary to intestinal perforation at the site of the lesion. Two cats (cats 16 and 24) died at home 1 week after surgery, but no necropsy was performed. Eight cats were alive at the termination of the study, 2 that had pyloric lesions and 6 with lesions at the ileocecocolic junction or colon. The 2 surviving cats with pyloric lesions were treated with prednisone.
Survival curves for cats with proximal (pyloric sphincter) and distal (ileocecocolic junction and colon) lesions are shown in Fig. 8. Mean survival times were not statistically different when cats with a lesion in the proximal gastrointestinal tract were compared with those whose lesion was in the distal/aborad portion.
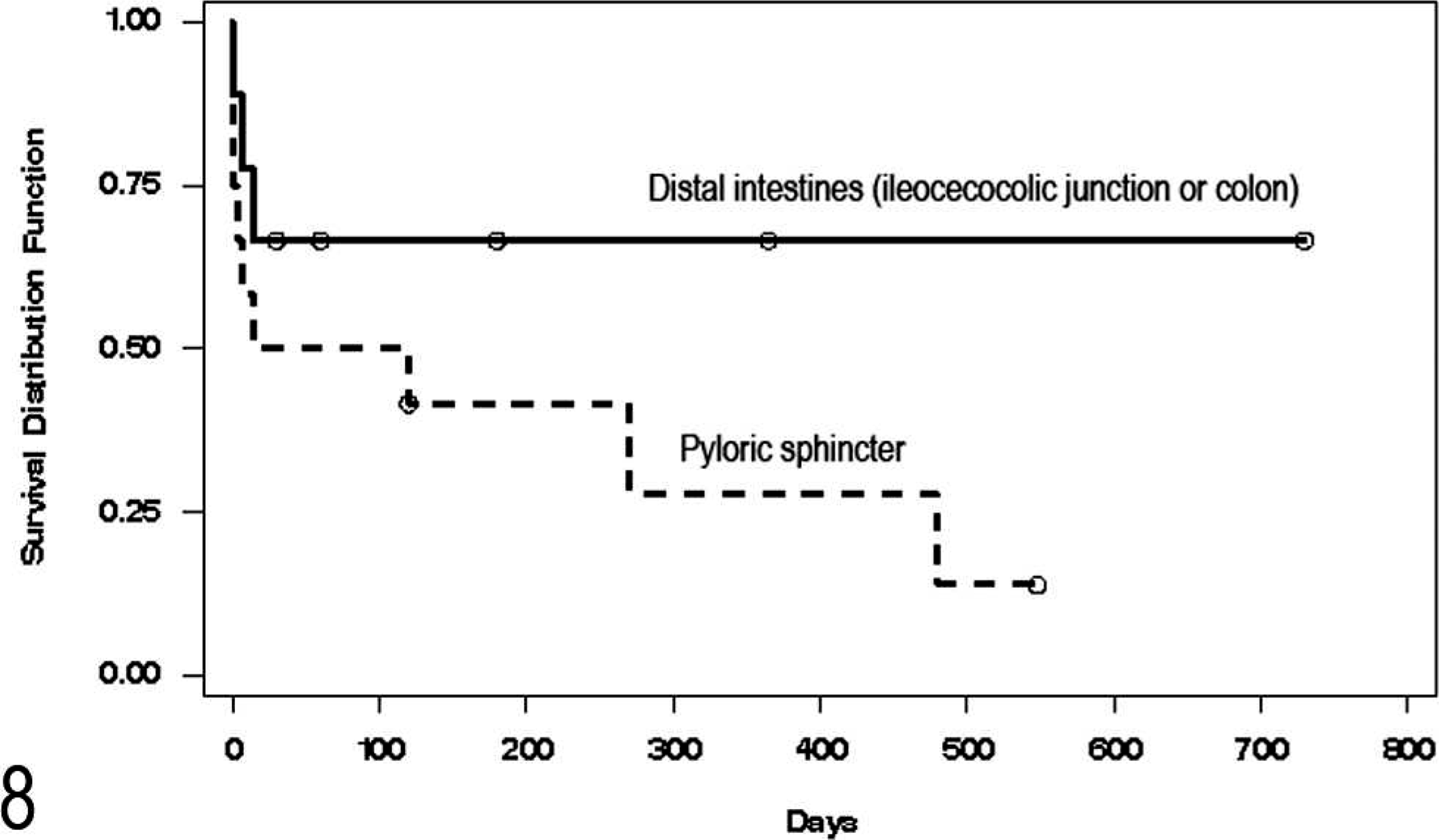
Comparison of survival between cats with lesion in the distal intestines (ileocecocolic junction or colon) with those with lesions at the pyloric sphincter. ○ = censored data point (cat still alive or lost to follow-up).
Discussion
The described cases have a very characteristic appearance consisting of dense collagen trabeculae, fibroblasts, and eosinophils. In some instances, cytology was representative of the histopathologic findings in that eosinophilic matrix, fibroblasts, and eosinophils were all present. In other cases, cytology revealed only eosinophils. Histologically, the collagen trabeculae can be very sclerotic, leading to the mistaken diagnosis of osteosarcoma in 2 cats included in this report. In addition, a previously published case of a feline duodenal osteosarcoma closely resembles this lesion. 17 The cat in the previous report was a 3-year-old neutered male that presented with vomiting, icterus, and peripheral eosinophilia. A proximal duodenal mass had been biopsied 1.5 years earlier and diagnosed as granulation tissue. At presentation there was a mass within the proximal duodenum obstructing the common bile duct. The histopathologic diagnoses on the surgically excised tissues were duodenal osteosarcoma and eosinophilic lymphadenitis. The photomicrographs more closely resemble the lesion described in the current report than osteosarcoma. That cat continued to have intermittent vomiting and died 4 months after surgery.
Although the spindle cells in this lesion can be quite large and feline myofibroblasts are known to have a tendency to undergo malignant transformation in response to ocular trauma 4 and vaccination, 5, 9 we do not believe this lesion is a neoplasm. The inflammatory context and the gradual transition of this lesion to more typical granulation tissue are not consistent with neoplasia. In addition, the lesion can occur in very young animals (14 weeks in one case). Large numbers of mast cells in some lesions strongly suggest neoplasia and 5 cats were diagnosed with sclerosing mast cell tumor. Although numerous mast cells are present within some of the lesions, these mast cells are widely dispersed and/or perivascular and are not consistent with a neoplasm. Four of the 5 cats diagnosed with mast cell tumor had bacteria within the center of the lesion. Of those 5 cats, 3 are still alive, 1 was euthanatized at surgery, and 1 (that was also feline immunodeficiency virus positive) died at home, 1 week after surgery.
In a previous study of 27 cats with similar eosinophilic sclerosing lesions, 9 had lesions in the cervical lymph nodes or subcutis. 14 However, all of the photographs were from an abdominal mass, so it is unclear whether the cervical lesions also had the distinctive collagen trabeculae described here. In that study, Gram-positive cocci (specifically, methicillin-resistant Staphylococcus aureus) were present in most of the lesions, but rods were seen in 6 of the cats, all of which were abdominal masses. 14 In our cats, bacteria were detected histologically at the center of the lesion in 14 of 25 cats. Although this is only a slight majority of the cases, the arrangement of the inflammation around the bacteria and the presence of the same bacteria and same lesion in draining lymph nodes, suggests that bacteria may play a role in the lesion. In this report the bacteria included Gram-negative rods, Gram-positive cocci, and Gram-positive rods. We hypothesize that these lesions were initiated by bacterial organisms, which are difficult to find histologically due to antibiotic therapy or the exuberant inflammatory lesion. It is unknown how the bacteria become embedded in the intestinal wall, but the predisposition for lesions to occur at the pyloric sphincter and ileocecocolic junction suggest that physical forces, such as foreign-body penetration, may play a role. Normal intestinal luminal bacteria and bacterial products have been shown to induce collagen synthesis and increase transforming growth factor (TGF)-β and interleukin (IL)-6 expression in intestinal myofibroblast cultures. 18 Although bacteria may incite the lesion, antibiotics were not clinically effective in the treatment of most cases. This may be because the bacteria are walled off by the lesion itself or because the eosinophils continue to perpetuate the lesion even after the bacteria are cleared.
The reason for the eosinophilic response is not clear, but cats can have an eosinophilic dermatologic and oral response (eosinophilic granuloma complex) to a variety of stimuli, including viruses, bacteria, and fungi. 2 Toxoplasma gondii was recently reported to cause eosinophilic fibrosing gastritis in a cat. 12 Cats that develop eosinophilic granuloma complex are thought to have an inherited eosinophil dysregulation leading to an inappropriate eosinophilic inflammatory response to a variety of stimuli. 2 Hypereosinophilia was present in 7 of the 12 cats (58%) tested in this study. We hypothesize that cats with a genetic predisposition to this lesion develop eosinophilic inflammation in response to the introduction of bacteria (or other antigens) into the intestinal wall, perhaps by a foreign body or ulceration.
Other possible causes of intestinal eosinophilic inflammation, such as fungi, oomycetes, and parasites, were not detected. However, the possibility of hypersensitivity to food or environmental antigens contributing to this lesion cannot be ruled out. Another possible association is herpesvirus infection, which causes eosinophilic inflammation in the skin of cats. 2 Although identification of herpesvirus was not attempted in this study, it would be an interesting avenue of investigation for future research on this lesion.
Eosinophils produce numerous mediators that play a role in fibrosis. 6 Eosinophil infiltration and major basic protein (MBP) deposition were present in lesions involving inflammatory fibrosis, and were absent in cases of noninflammatory fibrosis in a study of human patients. 13 Another study found elevated levels of MBP in the sera of some human patients with diffuse cutaneous systemic sclerosis. 3 Previous studies have also shown that activated eosinophils produce important fibrogenic mediators, such as TGF-β and IL-1β, which lead to fibroblast proliferation and extracellular matrix deposition. 1, 7, 11, 16 An important mediator in the initiation of TGF-β production by eosinophils is leukotriene D4. 10 Interestingly, cats with the longest survival times in this study were treated with prednisone, which inhibits the production of leukotrienes via the arachidonic acid pathway. 15
Lesions at the pyloric sphincter were more difficult to surgically excise than those in the more distal portion of the intestine. Cats with pyloric sphincter lesions (n = 12) were diagnosed by incisional biopsy or larger samples submitted after death. Two cats with lesions in this location were diagnosed at necropsy and 2 were euthanatized during surgery because of the location of the lesion. Five were euthanatized for continued clinical signs after incisional biopsy and antibiotic treatment. Of the remaining 3 cats treated with prednisone, 2 were alive at the time of this writing (4 months and 1.5 years after diagnosis) and 1 was alive 4 months after surgery when it was lost to follow-up. More of the distal (aborad) intestinal lesions (ileocecocolic junction or colon) were completely excised and 67% (6/9) of those cats are still alive.
There was no breed predisposition noted in this study; most of the cats were domestic shorthair, but this is representative of the cat population. There was a wide age distribution; range = 14 weeks to 15 years, with an average of 8.8 years. Most of the cases were male (72%), but the sex distribution of the patient population of all contributing institutions was not available, so the significance of this apparent male predominance is unknown.
In conclusion, we have described a unique inflammatory lesion of the feline gastrointestinal tract, which often contains bacteria, but does not respond to antibiotic treatment. The lesion is characterized by dense collagen trabeculae, large fibroblasts, and numerous eosinophils. The lesion is often grossly and sometimes histologically mistaken for neoplasia. Future studies will be needed to determine the prevalence, optimal therapeutic recommendations, prognosis, and pathogenesis of this unique lesion.
Footnotes
Acknowledgements
We thank Dr. Timothy Becker for follow-up clinical information on case No. 9 and Dr. Danielle Reel for contributing case No. 8. We also thank Dee Stephenson and Sharon Schlosshan for histology support, Ladonna Mrkonjich for immunohistochemistry support, and the staff of the UT Clinical Pathology Laboratory for cytology support.