
Abstract
Amanitin is a toxic cyclopeptide present in several species of poisonous mushrooms. Amanitin toxicosis was diagnosed in 2 cats from separate premises. Both cats initially had lethargy and vomiting, and they rapidly developed depression and neurological signs over 24–48 hours. Marked elevation of alanine aminotransferase was the primary finding, with subsequent serum chemistry values compatible with hepatic and renal failure. Histopathological findings consisted of submassive to massive acute hepatic necrosis, renal proximal tubular epithelial necrosis, and foci of necrosis and inflammation in the gastrointestinal tract. Amanitin exposure was confirmed postmortem by detection of α-amanitin in the kidney by liquid chromatography–mass spectrometry. A similar clinical course and pathological changes are reported in human and canine amanitin intoxication; however, gastrointestinal lesions are not typically described.
Amanitins are cyclopeptides present in several species of poisonous mushrooms in the genera Amanita, Galerina, and Lepiota and are considered to be responsible for the potent toxicity of these mushroom species. 5,10,11 Cases of natural amanitin toxicosis are reported in humans and dogs, and experimental toxicity studies have been described in a variety of species. 1,2,5,7,10 The clinical progression is classically described as multiphasic. 2,5,7,8,9 Following an initial latency period 6 to 24 hours post ingestion, gastrointestinal (GI) signs occur, including vomiting, bloody diarrhea, and abdominal pain. This can be followed by a period of seeming recovery, which may last hours to days, until the development of clinical signs of hepatic and renal failure in the final phase. Acute hepatocellular necrosis, often accompanied by renal proximal tubular epithelial necrosis, is the typical pathological finding. 2,5,7,8,9 We report the clinical and pathological changes associated with amanitin toxicosis in 2 cats. To our knowledge, this is the first report of amanitin toxicosis in cats.
Cat No. 1
In November, a 1-year-old spayed female domestic shorthair cat was presented to a veterinary practice in northern California for acute onset of vomiting, lethargy, and anorexia. Rectal temperature was 105.7°F. A complete blood count (CBC) was unremarkable. Serum chemistry abnormalities included marked elevation (too high to register) of alanine aminotransferase (ALT) and mild elevation of alkaline phosphatase (ALP) (128 IU/L; range 14–111 IU/L). Abdominal radiographs showed gas accumulation in the small intestine. An abdominal ultrasound showed a flaccid, fluid-filled stomach, hypermotile duodenum, and mild thickening of the colon wall. Treatment with ampicillin and supportive care was initiated. Fever and vomiting resolved, but anorexia continued and the patient became progressively depressed and developed ataxia and visual and proprioceptive deficits. After 48 hours, a repeat CBC was performed; the cat had thrombocytopenia (84 × 103/μl; range 175–600 × 103/μl) and severe leukopenia (1790/μl; range 5.5–19.5 × 103/μl) with neutropenia (570/μl; range 2.5–12.5 × 103/μl), and eosinopenia (30/μl; range 100–790/μl). Repeat serum chemistry demonstrated persistent elevation of ALT, marked azotemia with a blood urea nitrogen (BUN) of 100 mg/dl (range 16–36 mg/dl) and creatinine too high to register, hypoalbuminemia (1.9 g/dl; range 2.2–4 g/dl), hyperbilirubinemia (2.3 mg/dl; range 0–0.9 mg/dl), hypocholesterolemia (19 mg/dl; range 65–225 mg/dl), and hypoglycemia (23 mg/dl; range 74–159 mg/dl). On the third day following onset of clinical signs, the patient was referred to the Veterinary Medical Teaching Hospital of the University of California, Davis, where it was severely obtunded and hypothermic. The clinical diagnosis was fulminant hepatic failure with renal dysfunction. Humane euthanasia was elected.
Cat No. 2
In December, a 7-month-old neutered male Bengal cat was presented to an emergency and specialty hospital in northern California in lateral recumbency with ptyalism and a history of acute-onset lethargy and vomiting. On presentation, the cat was hypothermic (97.9°F), hypotensive (60 mm Hg systolic), and hypoglycemic (41 mg/dl). A CBC and serum chemistry had the following abnormalities: anemia (hematocrit 22.6%), leukocytosis (24.5 × 103/μl) with neutrophilia (22.2 × 103/μl) and basophilia (140/μl; range 0–100/μl), and elevated ALT (too high to register) and ALP (542 IU/L). Thoracic and abdominal radiographs were unremarkable. Supportive care was initiated with mild improvement in mentation but persistent hypotension. Repeat CBC values were within reference range. On repeat serum chemistry, there was persistent elevation of ALT (432 IU/L) and ALP (724 IU/L). Additionally, there was hypoproteinemia (4.4 g/dl; range 5.2–8.8 g/dl), azotemia with a BUN of 49 mg/dl and creatinine of 2.7 mg/dl (range 0.6–2.4 mg/dl), and hypocholesterolemia (39 mg/d). Partial thromboplastin time was prolonged beyond the reference range (60–119 seconds), and ammonia levels were within reference range. Clinical signs progressed to hyperesthesia, tremors, and oral ulceration. The patient died in hospital 18 hours following initial presentation, less than 48 hours from the onset of clinical signs.
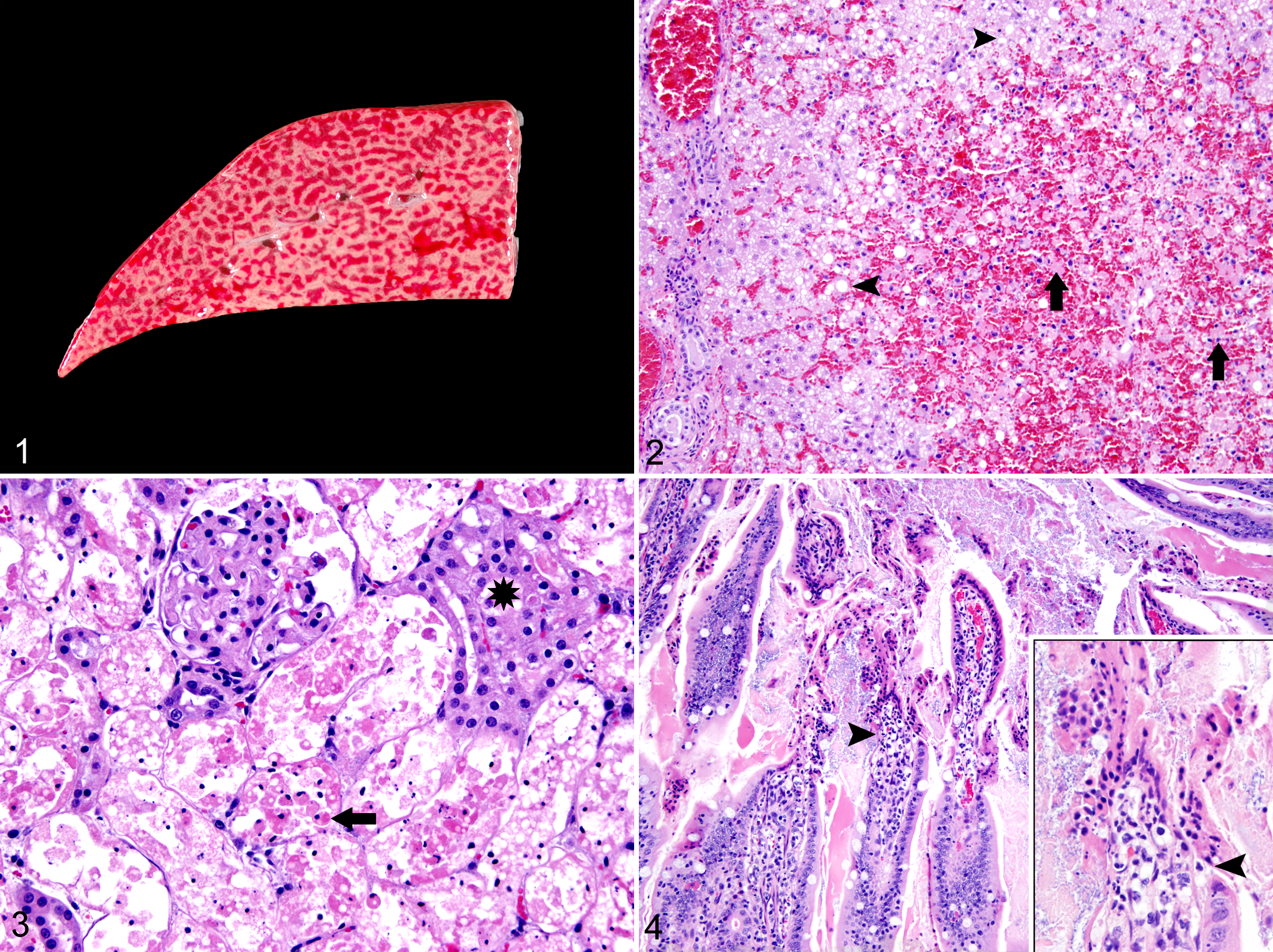
Necropsy was performed by a pathologist on cat No. 1.The liver had a prominent generalized pale tan reticular pattern with bright red central areas (Fig. 1). Multifocal mucosal hemorrhage was in the gastric fundus; the colonic mucosa was hyperemic with scattered petechiae. The necropsy of cat No. 2 was performed by the referring veterinarian; samples of liver, kidney, small intestine, and pancreas were submitted for histopathological analysis.
Due to suspicion of exposure to a hepatotoxicant, samples of fresh liver and kidney from cat No. 1 and samples of urine, serum, gastric contents, liver, and kidney from cat No. 2 were submitted to the Toxicology Section of the California Animal Health and Food Safety Laboratory System. An organic chemical screen by gas chromatography–mass spectrometry on liver from cat No. 1 was positive for pentobarbital, propofol, and phenytoin (consistent with euthanasia). Kidneys from cat Nos. 1 and 2 were positive (>2.5 ppb) for α-amanitin by liquid chromatography–mass spectrometry (LC-MS 3 ). The LC-MS 3 is detailed in online supplemental materials (for supplemental materials, please visit http://vet.sagepub.com/supplemental). Ion chromatograms and spectra for positive and negative controls and kidney samples from both cases are provided in Supplemental Figs. 1 –4. The presence of any level of α-amanitin is considered significant. Urine from cat No. 2 was also tested for α-amanitin and was negative (with a laboratory reporting limit of 2.5 ppb).
Histopathological Study
Histopathological examination of liver, lung, heart, spleen, kidney, ureter, lymph nodes, thyroid gland, pancreas, stomach, duodenum, jejunum, ileum, cecum, colon, skin, bone marrow, brain, and pituitary gland was performed in cat No. 1. Limited histopathological examination was performed in cat No. 2 and included kidney, liver, duodenum, jejunum, and pancreas. Tissues were fixed in 10% neutral buffered formalin and processed routinely. Lesions were limited to the liver, kidney, and GI tract of both cats. In the liver from cat No. 1, the central 75% of all lobules was replaced by hemorrhage, and hepatocytes in the affected areas were dissociated and necrotic with shrunken, hypereosinophilic cytoplasm and pyknotic and karyorrhectic nuclei (Fig. 2). Remnant periportal hepatocytes had highly vacuolated cytoplasm. Scattered lymphocytes and plasma cells infiltrated portal areas. The liver from cat No. 2 had panlobular hepatocellular necrosis with portal infiltration by scattered neutrophils and macrophages. In both cats, there was diffuse necrosis of the renal proximal tubular epithelial cells, characterized by granular to foamy hypereosinophilic cytoplasm and nuclear pyknosis, karyorrhexis, and karyolysis (Fig. 3). Many necrotic cells were dissociated from the basement membrane and present within the lumen of more distal tubular segments. Vessels at the corticomedullary junction were congested. In the stomach of cat No. 1, the superficial mucosa was focally necrotic and hemorrhagic. The cecum and colon from cat No. 1 had multifocal coagulative necrosis of the superficial epithelium with locally intense neutrophilic infiltration in the mucosa, extending into a submucosal lymphoid follicle. In cat No. 2, multiple segments of jejunum had acute necrosis of villous epithelial cells (Fig. 4). In summary, both cats had submassive to massive hepatocellular necrosis and renal proximal tubular epithelial necrosis. Superficial mucosal necrosis was in the stomach and colon of cat No. 1, but these tissues were not examined histologically in cat No. 2. Cat No. 2 did have focal jejunal mucosal necrosis, whereas the jejunum of cat No. 1 was unaffected.
Discussion
Based on the presence of α-amanitin in renal tissue and the pathological findings, both cats were diagnosed with amanitin toxicosis. In North America, amanitin toxicosis is typically attributed to Amanita spp, particularly Amanita phalloides, which grows in northern California from October to January, fitting the time frame for these cases. 5 The pathological findings reflect the mechanism of action of amanitin, which binds to RNA polymerase II, inhibiting transcription of mRNA and leading to diminished protein synthesis and eventual cell death. 10,11 In reported cases, hepatocytes and renal proximal tubules are consistently affected, which may reflect high rates of protein synthesis in these cells. 4,6,7 Accordingly, serum chemistry values in cases of amanitin toxicosis reflect aberrations in hepatic, and often renal, function. 5,7,9,10 In the present cases, the primary clinicopathological finding was marked elevation of ALT, indicating hepatocellular damage. Subsequent serum chemistry values, including elevated total bilirubin and low serum cholesterol, glucose, and albumin, reflected compromised hepatic function. The prolonged partial thromboplastin time in cat No. 2 may also reflect deficiency in coagulation factors secondary to hepatic failure. Additionally, both cats developed azotemia even with intravenous fluids, suggesting renal dysfunction. The neurological signs in both cats may have been the result of hepatic encephalopathy, although histological lesions, including those of hepatic encephalopathy, were not present in the brain from cat No. 1. The brain was not examined in cat No. 2; however, ammonia levels in cat No. 2 were within normal limits, making hepatic encephalopathy unlikely.
Acute hepatocellular necrosis and renal proximal tubular necrosis are the most commonly reported pathological findings in amanitin toxicosis and were the most extensive histological lesions in both cats. In addition, there were necrotizing lesions in the stomach and intestines. Although vomiting and diarrhea are common in amanitin toxicosis, GI lesions in naturally occurring cases are inconsistently reported and limited to mural and serosal hemorrhage and acute gastritis. 5,9 In one study, dogs injected with α-amanitin at a lethal dose had histological changes in the gastric and small intestinal epithelium consisting of individual to clustered epithelial cell necrosis, with the duodenum most prominently affected. 3 The pathogenesis of the GI lesions in these cats is difficult to interpret, given the variation in distribution between the 2 cases. We believe that given the chronicity and character of the lesions, amanitin is a direct cause of the gastrointestinal necrosis. Clotting abnormalities secondary to liver failure could lead to infarction, but there was no evidence of this in other tissues. Moreover, cat No. 1 was thrombocytopenic, and cat No. 2 had prolonged partial thromboplastin time. If the mucosal necrosis is a direct effect of amanitin, it is surprising that the small intestine was affected in cat No. 2 but not in cat No. 1 and that the jejunum in cat No. 2 was affected whereas the duodenum was spared. Perhaps the variation in lesion distribution reflects differences in exposure to, absorption of, or susceptibility to amanitin along the GI tract in cats. Other factors, such as hypoperfusion, could play a role; cat No. 2 remained hypotensive throughout hospitalization. The colonic lesions in cat No. 1 were associated with neutrophilic inflammation, which is possibly the result of secondary bacterial invasion.
Definitive diagnosis of amanitin toxicosis in animals is frequently confounded by a lack of exposure history. 7 The source of exposure in these cats remains unknown. Both cats were indoor/outdoor house pets so could feasibly have ingested mushrooms while unobserved. This possibility, in addition to the constellation of hepatic and renal necrosis and the time frame for the cases, influenced the decision to test these cats for amanitin. No potential for drug exposure was identified for either cat, making an idiosyncratic drug reaction unlikely. Definitive diagnosis in the present cases was facilitated by postmortem analysis of fresh kidney for amanitin by LC-MS. 3 This method can be used to identify amanitin in fresh liver and kidney, urine, and serum. 6,7 Approximately 90% of amanitin is cleared via the urine, and thus urine is the preferred sample for antemortem testing. 1,6 Kidney is considered the preferred tissue for postmortem sampling, as amanitins persist longer in kidney than in liver. 6 It is notable that in cat No. 2, α-amanitin was detect in renal tissue, but not urine, indicating that testing of both in a postmortem setting is advisable. The ability to detect amanitin in formalin-fixed or paraffinized tissues could facilitate retrospective diagnosis of amanitin exposure. Detection of amanitin in deparaffinized renal tissue has been reported. 6 However, in our case, attempts to detect amanitin in both formalin-fixed and paraffin-embedded kidney from cat No. 1 were unsuccessful.
Although both natural and experimental cases of amanitin toxicosis have been documented in dogs, 2,5,7,9 there are no published cases of feline amanitin toxicosis to our knowledge. Dogs typically have less discriminating eating habits than cats and, in some cases, may have increased access to outdoor environments, but increased susceptibility of dogs to α-amanitin cannot be ruled out as a cause for this difference. In a study on the parenteral lethal dose of α-amanitin in several animal species, dogs and guinea pigs were most susceptible. 2
In summary, the clinical and pathological findings in cats with amanitin toxicosis resemble those in humans and dogs. Amanitin toxicosis should be considered as a differential diagnosis in cats with acute hepatic failure or extensive acute hepatocellular necrosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.