
Abstract
A 2–year-old, female hedgehog presented with an 8–month history of progressive, ascending paresis/paralysis and was tentatively diagnosed with wobbly hedgehog syndrome. She died awaiting further diagnostic tests, and the owners consented to postmortem examination. Grossly, the bladder was large and flaccid and the cervical and lumbar spinal cord were regionally enlarged, light grey, and friable with multifocal hemorrhages. The thoracic spinal cord was grossly normal. Microscopically all regions of the spinal cord had similar changes, although the cervical and lumbar sections were most severely affected. These regions were completely effaced by a moderately cellular infiltration of highly pleomorphic polygonal to spindle shaped cells, mineralization, and necrosis, which were most consistent with anaplastic astrocytoma. The thoracic spinal cord white matter was similarly infiltrated by the neoplastic cells, with perivascular extension into the otherwise normal grey matter. A diagnosis of anaplastic astrocytoma was confirmed using immunohistochemical stains that were positive for glial fibrillary acidic protein and S100.
Astrocytomas in humans are a heterogenous group of malignant neoplasms with clinical, radiographic, and histologic features that typically subdivide them into several categories. 1 Astrocytomas are common in humans and have a bimodal age distribution: the brainstem is more commonly affected in childhood, whereas cerebral astrocytomas are more common in middle age. Spinal cord and cerebellum are both rarely affected. All astrocytic tumors share the common characteristic of being highly cellular with peripheral invasion into the neuroparenchyma and stain consistently immunopositive for glial fibrillary acidic protein (GFAP). 1 Neoplastic cells typically have an obvious astrocytic appearance histologically, although this can sometimes be difficult to distinguish from reactive astrocytosis, particularly in biopsy specimens taken from the periphery of an infiltrating mass.
Based on morphologic characteristics of the individual cells and prognosis, astrocytomas in humans are divided into fibrillary or “diffuse,” and pilocytic. Among the fibrillary astrocytomas, tumors can be further graded. An important feature of fibrillary astrocytomas is their tendency to undergo anaplasia, become progressively more malignant, and increase in grade over time. This characteristic makes a universal grading system for these tumors difficult. Several grading systems have been developed using various morphologic criteria. Because of their relative simplicity, the Ringertz system using words (astrocytoma, anaplastic astrocytoma, glioblastoma multiforme) and the corresponding World Health Organization (WHO) grading system (grades II–IV) were used in this case. Grading of fibrillary astrocytomas, based on these methods, is divided into well-differentiated astrocytoma (grade II), anaplastic astrocytoma (grade III), and glioblastoma (grade IV). Grade I astrocytomas are reserved for the pilocytic type as they are uniformly less aggressive and have an overall better prognosis. Frequently, different grades can be identified within the same tumor making an overall final grade difficult. 1
This article documents an anaplastic astrocytoma in a hedgehog and reviews and compares some known information about astrocytomas in humans and animals.
A 1.5-year-old, female African pygmy hedgehog (Atelerix albiventris) was examined for abdominal distention, fecal incontinence, and dragging hind legs. She had an 8-month history of lameness with progressive development of bilateral hind limb and ultimately left front limb paresis as well as urinary bladder distention. On physical examination, she had ulcerative skin wounds on her abdomen, with urine scalding, bilateral hind limb paralysis and a distended painful abdomen. Radiographs showed marked urinary bladder distention. Initial complete blood count (CBC) and serum chemistry findings were normal, and there was no response to treatment with meloxicam, antibiotics, or corticosteroids. Clinical signs gradually became more severe and the hedgehog died at home. The owners consented to a postmortem examination.
On gross exam, the hedgehog was thin and weighed 400 g. There was subcutaneous bruising on the right hind limb and subcutaneous edema in the right axillary area and flank (from subcutaneous fluid administration). There were multiple epidermal crusts on the skin in the inguinal region. There was 35 ml of yellow-amber fluid (urine) in the abdominal cavity, and the bladder was markedly enlarged and flaccid with a focal ecchymotic hemorrhage (cystocentesis site).
Tissue samples were collected, fixed in 10% neutral-buffered formalin, and routinely processed and stained with hematoxylin and eosin (HE) for microscopic evaluation. Several immunohistochemical stains on selected sections of spinal cord were performed based on a standard avidin-biotin-peroxidase method. The following antibodies were used: GFAP, neuron-specific enolase (NSE), neurofibrillar filaments (Ventana, Tuscon, AZ), and S100 (Dako, Carpinteria, CA).
Microscopic lesions were limited to the spinal cord. The lumbar and cervical spinal cord were completely effaced by a highly cellular infiltration of pleomorphic polygonal to spindle shaped cells with large oval to irregular, hypochromatic, vesicular nuclei and scant to moderate amounts of eosinophilic cytoplasm. There was marked anisocytosis and anisokaryosis, and mitoses were rare (Fig. 1). There were multifocal areas of necrosis and mineralization throughout (Fig. 2) with regions of vascular hyperplasia (Fig. 3). Numerous necrotic neurons and spheroids were also present. The thoracic spinal cord white matter was infiltrated by the same population of neoplastic cells (Fig. 4) with perivascular extension into the otherwise normal grey matter (Fig. 5).
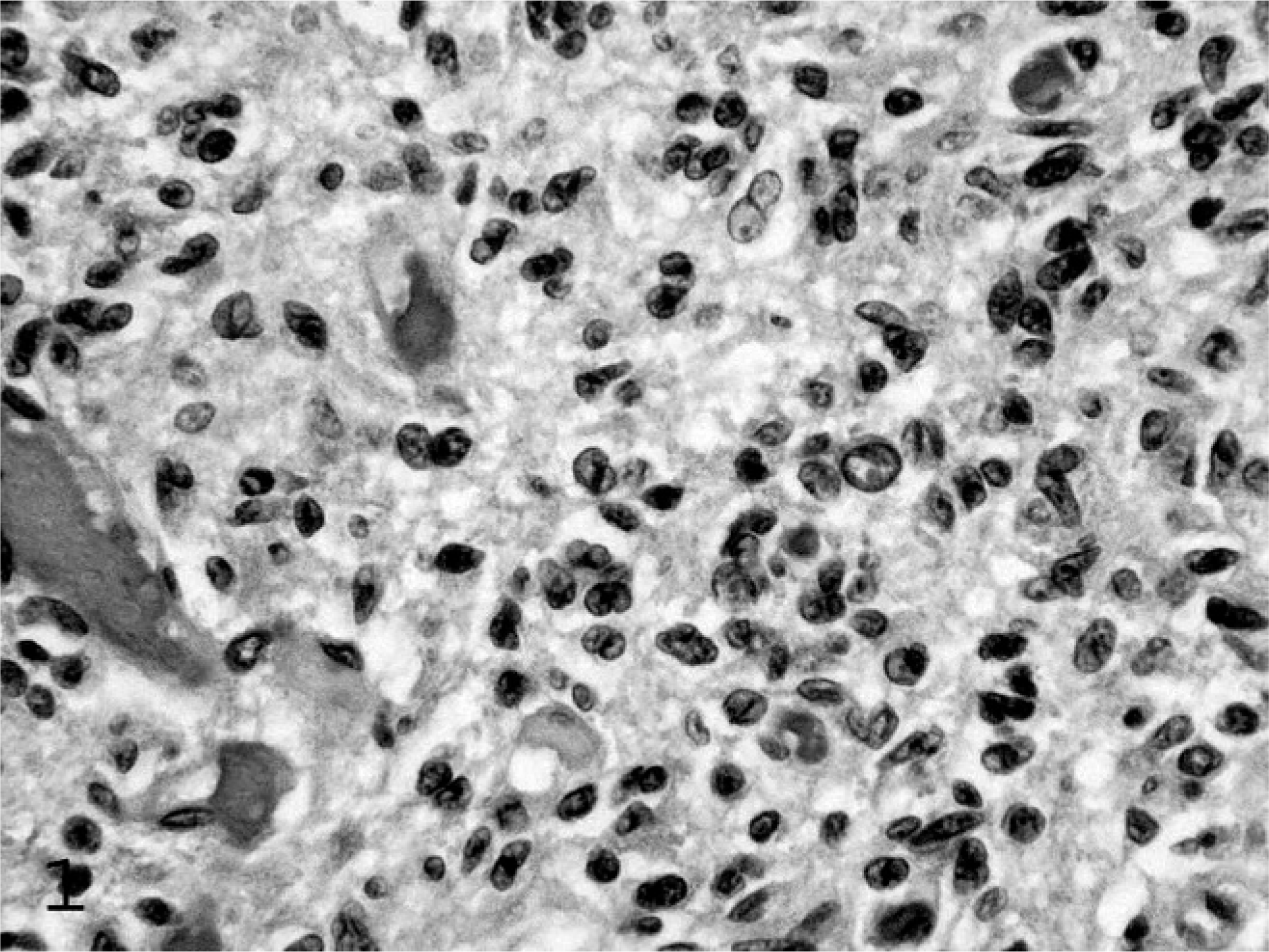
Mass, spinal cord; hedgehog. The mass is composed of a pleomorphic population of polygonal to spindle cells with irregular oval nuclei and marked anisocytosis and anisokaryosis. HE.
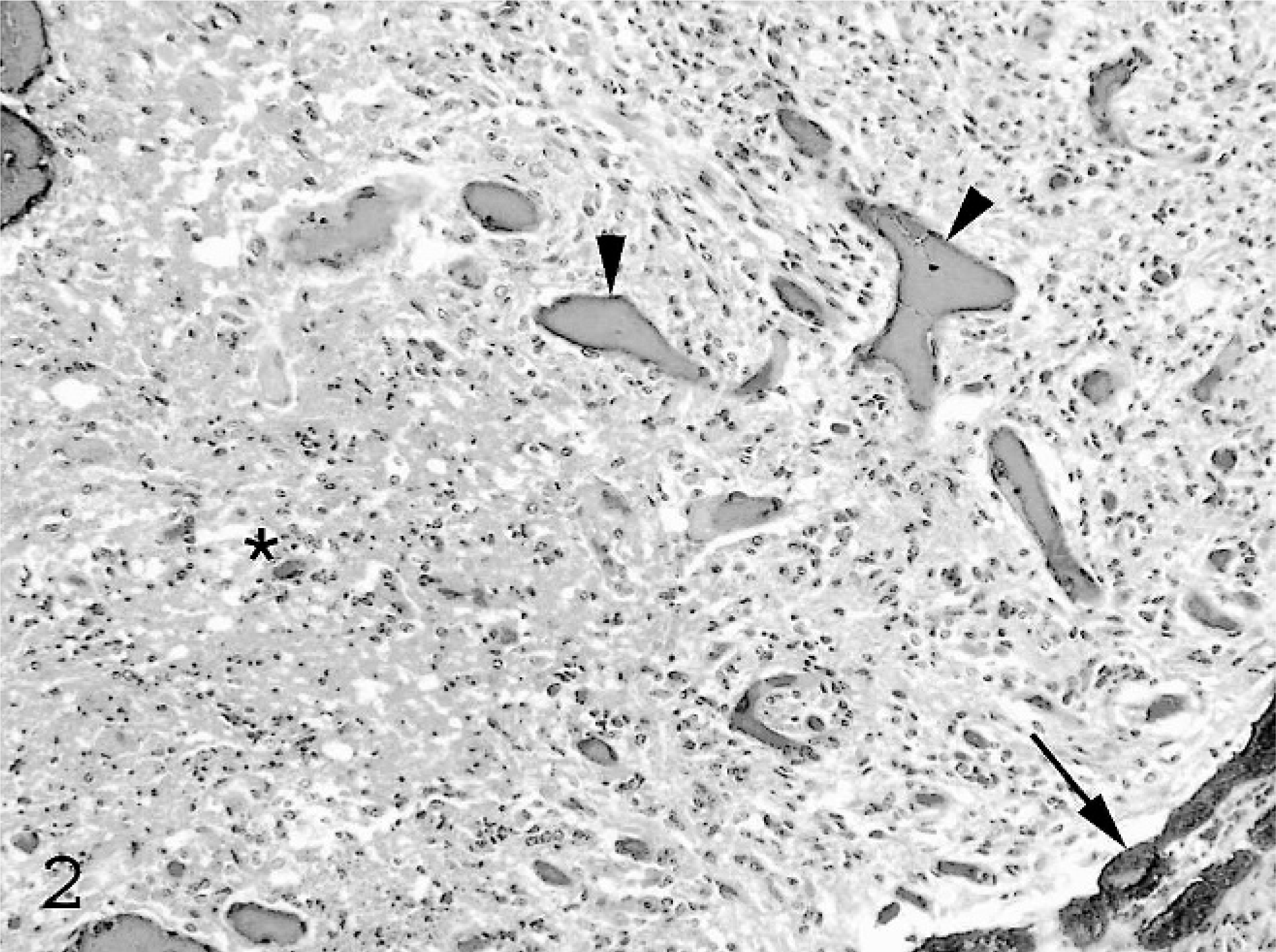
Mass, spinal cord; hedgehog. There are large regions of necrosis (∗) and mineralization (arrow). Vessels are distended with blood (arrowheads). HE.
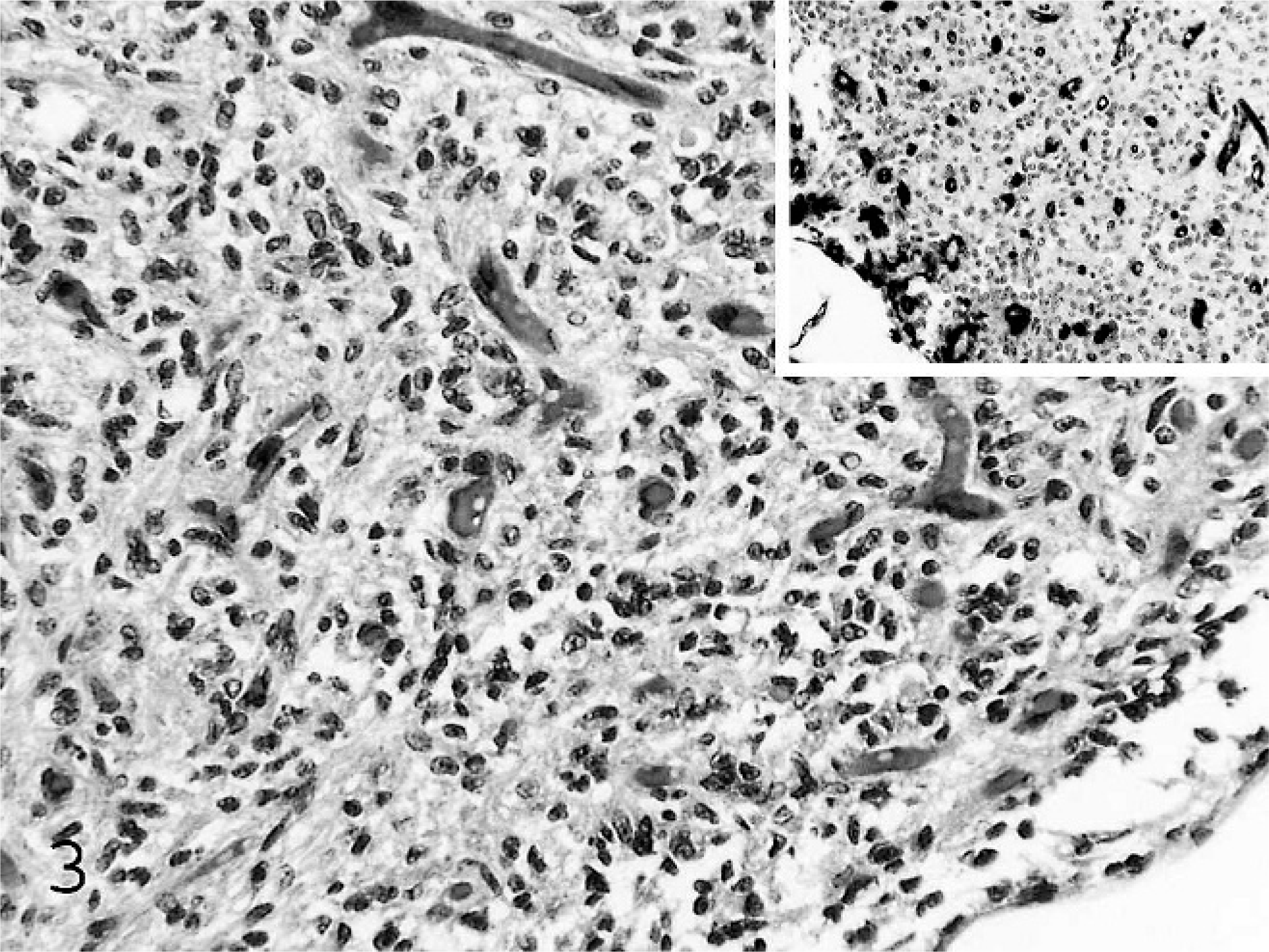
Mass, spinal cord; hedgehog. There is marked vascular hyperplasia. HE. Inset: vascular hyperplasia is highlighted by staining of endothelium for vimentin.
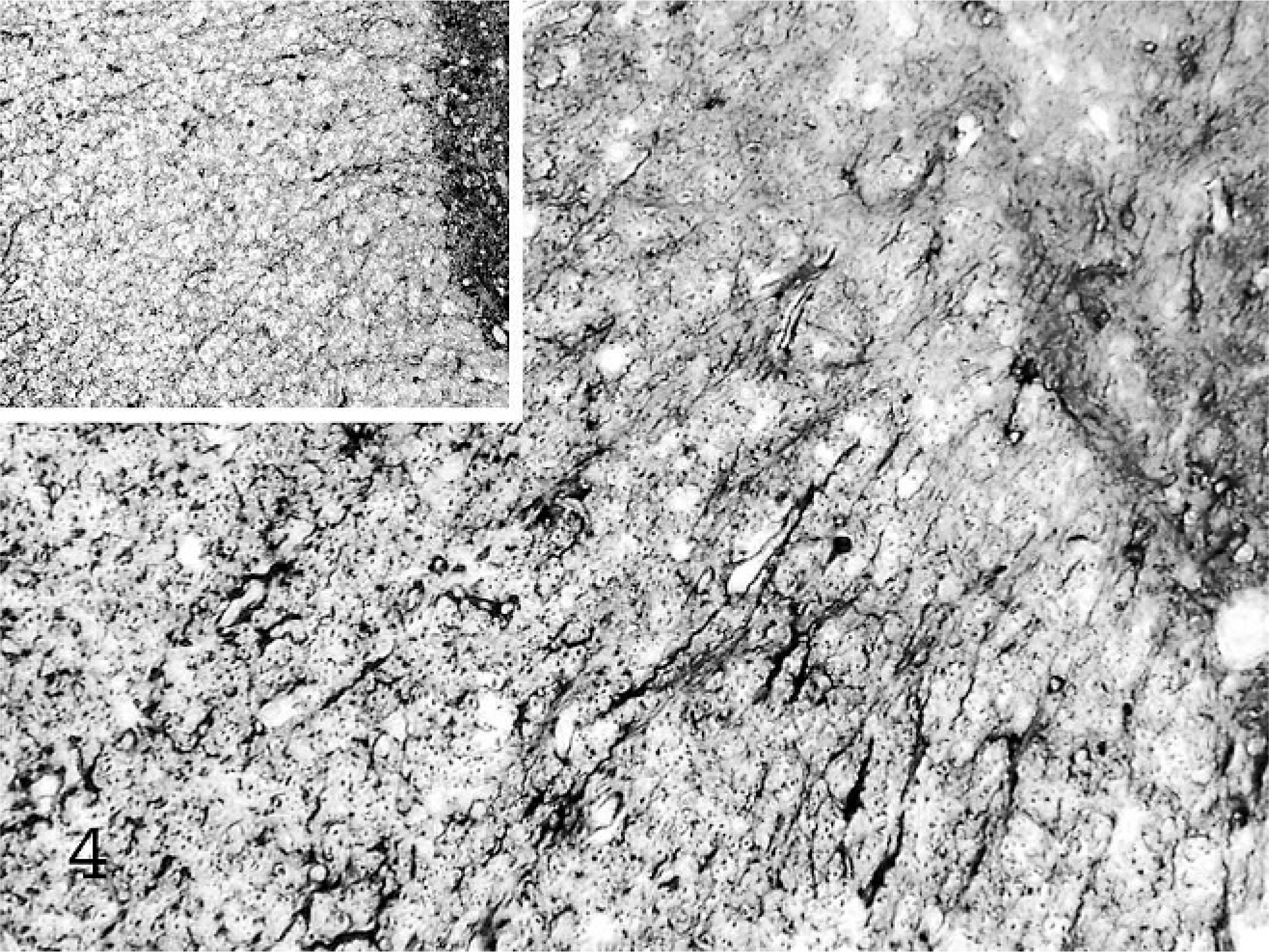
Mass, spinal cord; hedgehog. The less affected thoracic segment exhibits increased numbers of neoplastic astrocytes within the white matter. GFAP immunohistochemistry with hematoxylin counterstain. Inset: normal control, GFAP.
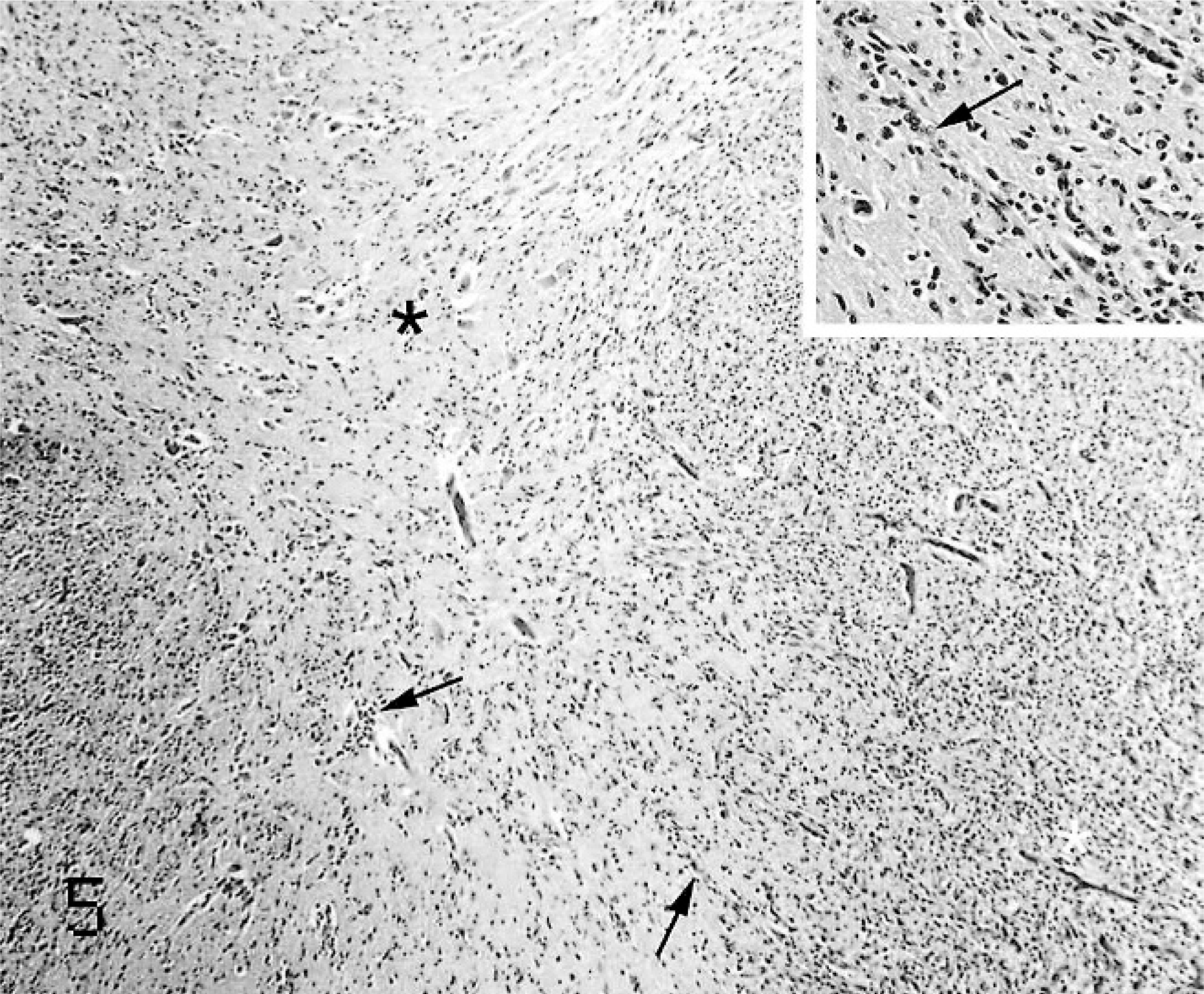
Mass, spinal cord; hedgehog. Neoplastic cells extend into the grey matter of the spinal cord (∗) from the white matter (white ∗) along vessels (arrows). HE. Inset: high power.
The tumor cells in this case demonstrated moderate cellular and nuclear pleomorphism with bilobed nuclei, and karyomegaly. Immunohistochemistry findings showed diffuse cytoplasmic positivity for GFAP, particularly of short, irregularly branched, cytoplasmic processes (Fig. 6), and diffuse strong cytoplasmic positivity for S100. The tumor had nonspecific staining for NSE, and was negative for neurofilament and vimentin. Based on the cellular and nuclear pleomorphism, invasion into the grey matter, and the presence of necrosis, a diagnosis of anaplastic astrocytoma was made.
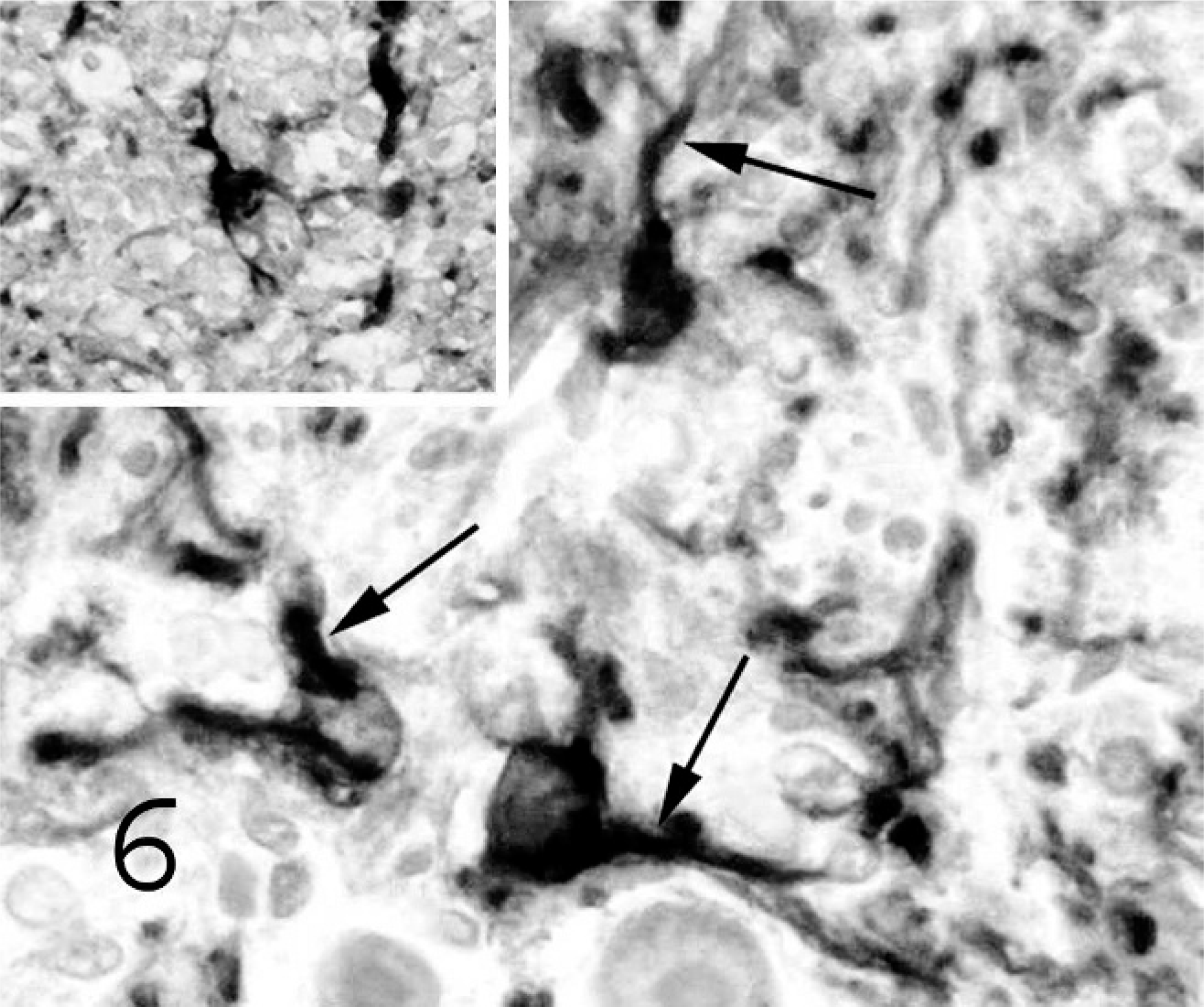
Mass, spinal cord; hedgehog. There is diffuse cytoplasmic staining and blunt cytoplasmic processes (arrows) for GFAP. GFAP immunohistochemistry with hematoxylin counterstain. Inset: normal control; notice fine cytoplasmic processes of a normal astrocyte, GFAP.
Astrocytomas (WHO grade II) are well-differentiated, diffusely infiltrative neoplasms of fibrillary astrocytes. 1 Microscopically, astrocytomas appear as ill-defined regions of hypercellularity, often subtle, within the white matter that merges with the normal neuroparenchyma. Astrocytoma cells are irregularly distributed compared with normal white matter and have enlarged, cigar-shaped, or irregular hyperchromatic nuclei. The cytoplasm can vary from scant (naked nuclei), with the classic, short cytoplasmic processes, to abundant rotund gemistocytic cytoplasm. Gemistocytic cells are often confused with reactive astrocytes, the latter of which are differentiated by uniform distribution and symmetric stellate cytoplasmic processes. Mitoses are usually absent in low-grade astrocytomas.
Most astrocytomas are GFAP, S100, and vimentin positive. Interestingly, cytokeratin and epidermal growth factor are sometimes positive as well. Differential diagnoses for these low-grade tumors include oligodendroglioma, higher-grade tumors, fibrillar ependymoma, reactive gliosis, demyelinating disease, and cerebral infarcts. However, the hypercellularity of demyelinating diseases is due to infiltrating macrophages, which appear similar to neoplastic gemistocytic astrocytes but have more distinct cytoplasmic membranes and are easily differentiated with immunohistochemistry. Pilocytic astrocytomas (WHO grade I) are less aggressive and surgery is often curative in humans, making an accurate diagnosis important. They are usually circumscribed and cystic, with a marked difference in invasiveness and malignancy, and are more common in young children and young adults. In humans these tumors are differentiated by having Rosenthal fibers, protein droplets, and granular bodies. 1 Rosenthal fibers, which are elongated eosinophilic bundles that are thought to be clumped intermediate filament proteins, are reportedly rare in pilocytic astrocytomas of dogs. 4
Anaplastic astrocytomas (WHO grade III) have increased cellularity, increased nuclear pleomorphism, increased mitotic activity, and a higher degree of proliferating cells 1 as seen in this hedgehog (Fig. 1). Some have a pronounced gemistocytic component, which is often associated with increased malignancy. 1 Typically, the extent of nuclear atypia and mitotic index indicates anaplastic transformation (Fig. 1). Immunohistochemical results are similar for all grades of astrocytomas with GFAP, S100, and vimentin being consistently positive. Interestingly, however, vimentin was negative in the hedgehog described in this case. Additional sections of this hedgehog's brain were stained with vimentin and revealed that most of the normal astrocytes were vimentin negative. The reason for this is unknown as internal controls (neurons, blood vessels, meninges) were strongly vimentin positive.
High-grade astrocytoma or glioblastoma multiforme (WHO grade IV) is a highly malignant glioma related to fibrillary astrocytoma, but sometimes such astrocytomas are so poorly differentiated that an astrocytic origin is not obvious. They can sometimes arise from oligodendrogliomas that acquire astrocytic qualities. 1 Glioblastoma is the most common glioma in humans, however, the spinal cord is an uncommon site. These tumors have a highly variable morphology but often have regions of necrosis with pseudopalisading; mitoses are common. They most commonly develop as a progression from anaplastic astrocytomas, and they often contain giant cells and so can be mistaken for metastatic sarcoma. Sometimes they have characteristics of metastatic carcinomas, with glandular structures and keratin pearls and can be difficult to distinguish if cytokeratins and epidermal growth factor are used. Another important feature of glioblastoma, in addition to necrosis, is hyperplasia of vascular cells, which differs from the vascular hypertrophy in many gliomas (Fig. 3). GFAP is usually positive but may be highly variable with less differentiated cells being negative. 1
Other less common types often confused with fibrillary astrocytomas are gliosarcoma, protoplasmic astrocytomas, granular cell astrocytomas, and gliomatosis cerebri. 1 The neoplasm in this hedgehog illustrates that multiple morphologic variants and histologic grades of neoplastic astrocytes can occur within a single tumor in hedgehogs as they do in humans. This makes it difficult to place an astrocytic neoplasm into a specific category or grade. Overall, the neoplastic cells in this hedgehog showed marked cellular and nuclear pleomorphism consistent with anaplastic astrocytoma (grade III; Fig. 1). The extent of the spinal cord involvement with effacement of cervical and lumbar regions and thoracic segment white matter was remarkable and more consistent with the higher-grade glioblastoma. Other features of glioblastoma that were seen in the neoplasm in this hedgehog included mitotic figures, foci of necrosis (Fig. 2), and vascular hyperplasia (Fig. 3); however, these features were only occasionally seen and wer not prominent enough to warrant a diagnosis of glioblastoma.
Astroglial tumors have been reported in a variety of other animal species. 10 Many of the subtypes of astroglial tumor that occur in humans have not been described in animals. 10 The typical locations and bimodal age distribution of astroglial tumors reported in humans is generally not seen in animals, and most occur in aged animals, especially dogs, with a predilection for brachycephalic breeds, but numerous dog breeds are affected. A review of intracranial primary neoplasms in the dog showed that 17% of these are astrocytomas or glioblastomas. 8 One study of 31 dogs demonstrated that 35% of the astrocytomas had genetic alterations in p 53, which is similar to that found in human astrocytomas. Also, overexpression of epithelial growth factor receptor was found in certain types of astrocytic tumors. 9 Astrocytomas are uncommon in cats, only a few individual case reports have been documented and one study of 8 cats described 4 subtypes (pilocytic, protoplasmic, gemistocytic, and fibrillary). 7 There are also reports of astrocytomas in pigs and cattle. 10 Astrocytomas are rare in common mice breeds but a 1% incidence is found in the VM strain. 10 Glioblastoma has been reported in a baboon 10 as well as deer, an elk, a goat, a llama, a rat, and a raccoon. 5 Attention is paid to these tumors because of their high incidence in humans and because they represent a good example of progressive mutations leading to increased malignancy. With the advent of gene microarrays, the specific genes responsible for each step in tumor transformation and progression can be identified, and a study in dogs showed similarity of gene expression to humans in some brain tumors. 11
Hedgehogs are becoming more popular as pets, but the incidence of many of their diseases, including tumors of the central nervous system, is largely unknown. In a study of spontaneous tumors in captive African hedgehogs there was a very high incidence of tumors (35 of 66 hedgehogs; 53%) especially in older hedgehogs (>1 year old), with integument, digestive, and endocrine systems most commonly affected and mammary gland adenocarcinoma, mast cell tumors, lymphosarcoma, and oral squamous cell carcinomas being the most common. 6 Nervous system tumors were not observed. 6 In a similar study, the prevalence of neoplasia in African hedgehogs at necropsy was found to be between 29% and 53%. 3 Up to 85% of tumors in hedgehogs are malignant. In this study, no additional cases of central nervous system tumors were found. 3
Wobbly hedgehog syndrome (WHS) was observed beginning in mid-1990s and is a progressive paralysis that occurs in approximately 10% of pet African hedgehogs in North America. 2 Signs begin with mild ataxia, progressing to severe neurologic signs (falling to one side, tremors, exophthalmos, scoliosis, seizures, muscle atrophy, self-mutilation) and ultimately leads to complete paralysis and muscle wasting. In 70% of cases reported ascending signs started in the hind legs. Onset occurs under 2 years of age and complete paralysis occurs by 15 months after onset of signs. 2 Histologic findings in WHS are predominantly limited to vacuolation of white matter tracts of cerebrum, cerebellum, brainstem, and spinal cord, and this process of progressive demyelination occurs without an inflammatory infiltrate. Various treatments have been used but are generally unsuccessful. The etiology is unknown; however, disease appears to be restricted to family lineages. In a study of WHS there was a 7% (3 of 45) incidence of astrocytomas at necropsy in hedgehogs that presented with clinical signs of WHS. 2
Little is known about diseases of hedgehogs, but more reports are being written about the very high incidence of neoplasia in these animals. Because many of these animals suffer from a debilitating central nervous system degenerative disease (WHS) the incidence of central nervous system neoplasia may be overlooked and some of these animals may benefit from early detection and treatment. In light of the findings in this case, and studies on WHS, neoplasia should be a differential in hedgehogs with clinical signs of spinal cord disease.
Footnotes
Acknowledgements
We thank Dr. Rolf Pfannl, Tufts-NEMC, Boston, for his consultation.