
Abstract
Neoplasms affecting the central and peripheral nervous systems of wild animals are extremely rare. Described are clinical signs and pathologic and immunohistochemical findings in an adult female raccoon (Procyon lotor) with an astrocytoma that involved medulla, cervical spinal cord, and roots of the cervical spinal nerves. Microscopically, the neoplastic cells revealed some pleomorphism but generally had fusiform morphology and showed moderate numbers of mitotic figures. Glial fibrillary acidic protein was demonstrated within the neoplastic cells by immunohistochemistry. This appears to be the only reported case of astrocytoma that involved multiple anatomic sites in the central nervous system of this raccoon.
Raccoons are highly adaptable and have managed to survive and increase their numbers in many urban and suburban areas. They are omnivores, and their diet may include carrion. Because raccoons share the immediate environment with human beings, they have been used as monitors of zoonotic diseases and environmental contamination. 1, 3
Neoplastic lesions have infrequently been documented in raccoons (Procyon lotor). Except for the neoplasms of thyroid and adrenal glands, only isolated case reports affecting other organs have been reported. 4, 5
History, Gross Findings, and Laboratory Results
The subject was an adult, female, free-ranging raccoon that had been provided with food by owners of a home in Lincoln City, Oregon, for a few years. At one time it was seen dragging its forelegs while walking, and soon after that the clinical signs of lameness became progressively worse. It was live-trapped and sent for examination at the College of Veterinary Medicine, Oregon State University. The raccoon was found to have marked muscle atrophy of both front legs (Fig. 1). The atrophy was more obvious in the left foreleg, and the raccoon was unable to retract this leg. No reflexes were seen in either of the forelegs. Some muscle atrophy was also seen in the hind limbs. At this point the animal was euthanatized and necropsy was conducted.

Raccoon with astrocytoma. There is marked atrophy of tissues over the shoulders (arrow) and both forelegs and hind legs.
Gross lesions were confined to the neck and forelegs. There was extensive muscle atrophy around the neck and shoulders and in both forelegs but was more marked on the left front side. Moderate muscle atrophy was also noted in both hind legs. The spinal cord at C5 to T1 and the brachial plexus appeared swollen, but otherwise appeared normal. The brain and the cervical spinal cord were fixed by immersion in 10% neutral buffered formalin. The formalin-fixed brain was cut into 2–4 mm thick coronal sections, and 4 sections of brain (cortex, hippocampus, cerebellum, medulla), 2 sections of cervical spinal cord, and 1 section of brachial plexus were processed by routine histologic procedures, embedded in paraffin wax, and sectioned at 5-µm thickness. The sections were stained with HE, and selected sections were labeled with glial fibrillary acidic protein (GFAP; DakoCytomation, DK-2600 Glostrup, Denmark) by immunohistochemistry.
Differential Diagnosis
In this case the differential diagnoses to consider would be trauma and inflammatory and neoplastic conditions. Inflammatory processes would include viral (rabies, canine distemper), parasitic (toxoplasmosis, aberrent parasitic migrations), granulomatous inflammations (bacteria, fungi), and neoplastic conditions. The viral and parasitic inflammations have frequently been described in free-ranging raccoons.
Microscopic Findings
Histopathologic lesions were confined to the medulla oblongata, cervical spinal cord, and nerves in the brachial plexus. In the medulla and the spinal cord there was extensive infiltration with neoplastic cells that had obliterated the grey matter around the central canal (Fig. 2). At both sites there was also considerable infiltration of the neoplastic cells into the dorsolateral white matter, the meninges, and the root sheaths of the spinal nerves. Within the neoplastic cell infiltration there were scattered normal-appearing neurons and some dilated axon sheaths. Morphologically, although there was some pleomorphism in the neoplastic cell population, the cells were generally fusiform and to varying degrees resembled proliferating glial cells. Moderate numbers of mitotic figures (up to 3 per ×40 objective) were seen. Some of the neoplastic cells were slightly larger, and these had a single nucleus that was more vesicular than the nucleus present in other small neoplastic cells. Most of the larger neoplastic cells and scattered smaller cells were positive on GFAP stain (Fig. 3). A similar cell population was also present in the spinal roots where the neoplasm had infiltrated.
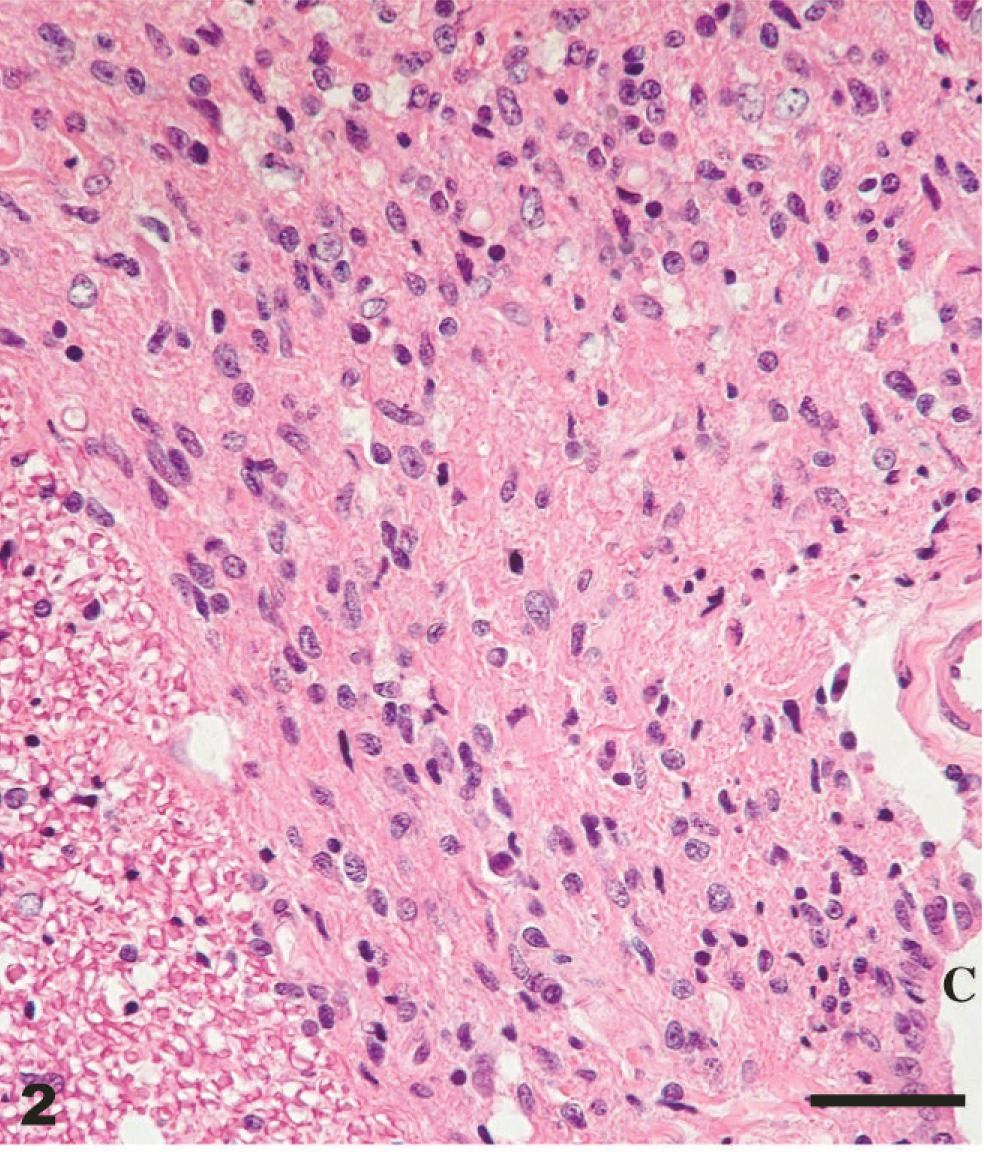
Medulla oblongata of raccoon showing extensive infiltration of neoplastic cells in the grey matter around the central canal (c). HE. Bar = 50 µm.
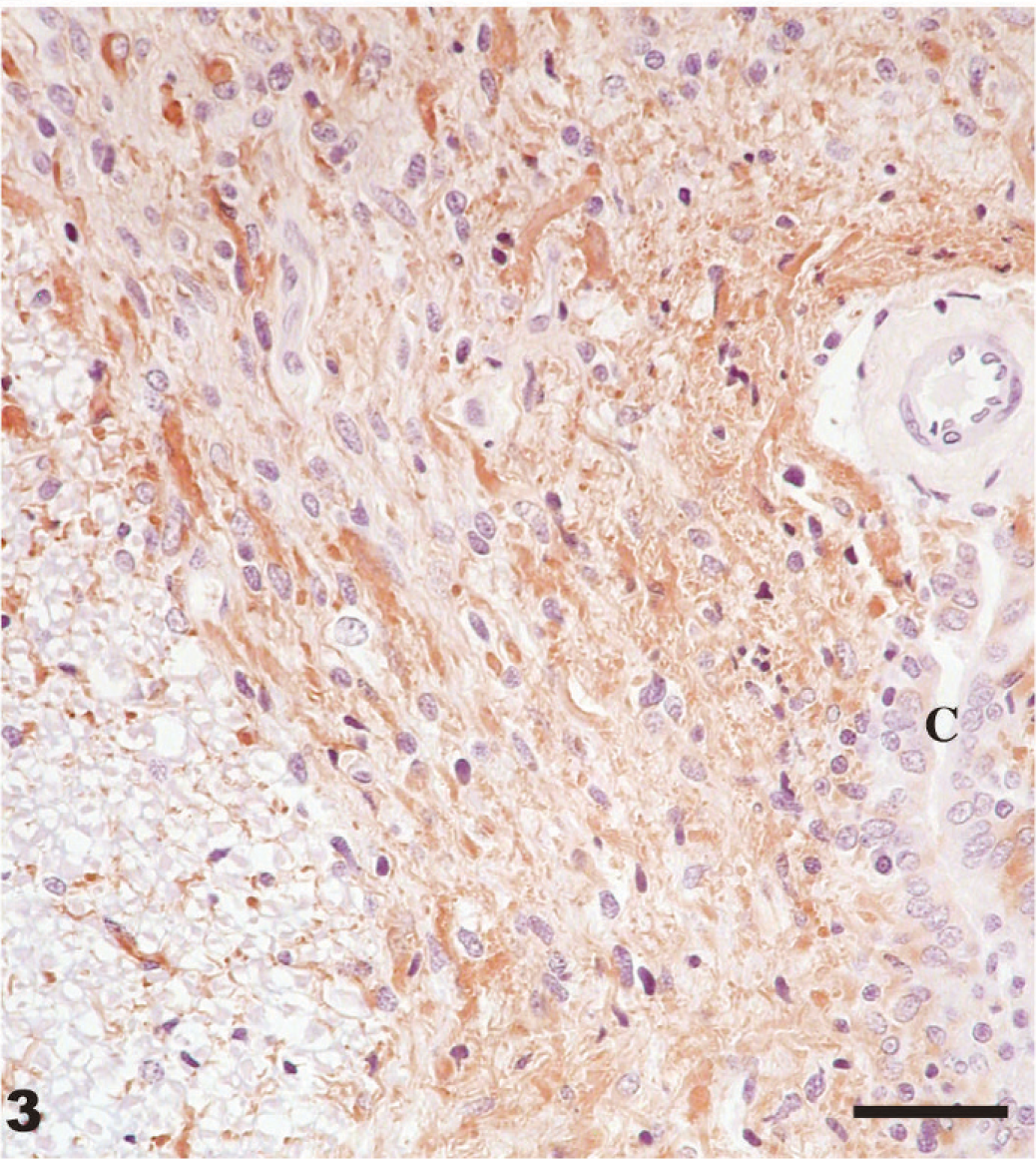
Medulla oblongata of raccoon showing extensive infiltration of neoplastic cells in the grey matter around the central canal (c). Most of the neoplastic cells are stained positive (brown). Stained for GFAP by immunohistochemistray. Bar = 50 µm.
Diagnosis
The neoplasm was diagnosed as a spinal cord astrocytoma with invasion into the medulla and the roots of the spinal nerves. Nerves in the brachial plexus revealed multifocal areas of axonal swelling (Wallerian degeneration) (Fig. 4), but neoplastic cells were not seen at this site.
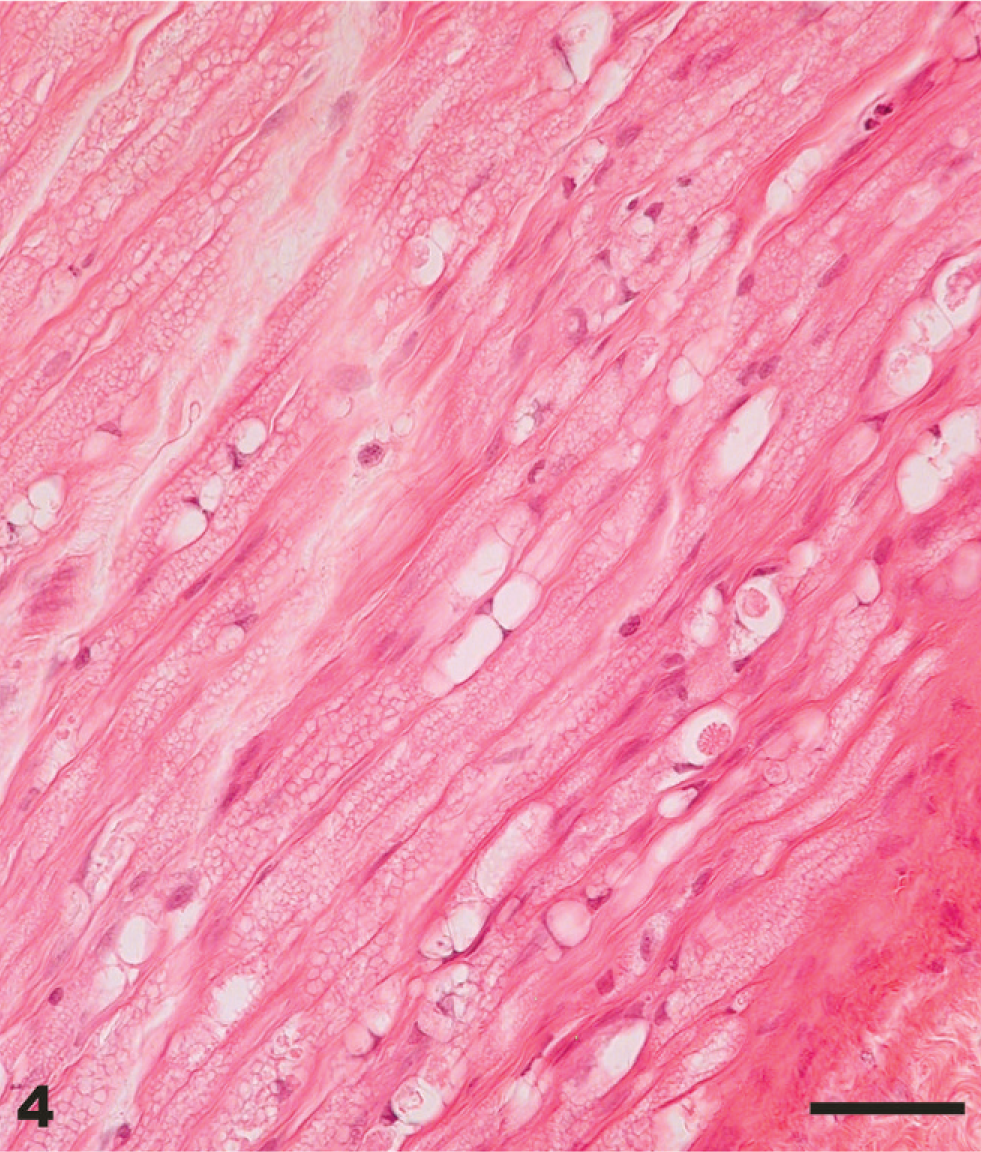
Peripheral nerve from the brachial plexus of raccoon. There is multifocal swelling of axons and axon sheaths (Wallerian degeneration). HE. Bar = 50 µm.
Discussion
As mentioned under the differential diagnosis, trauma, inflammatory and neoplastic processes should have been considered in this raccoon. However, the microscopic examination revealed extensive neoplastic infiltration of the medulla, cervical spinal cord, and roots of the spinal nerves. Immunohistochemical staining with GFAP provided the definitive diagnosis of this neoplasm.
Neoplastic lesions have infrequently been documented in the family Procyonidae. With the exception of thyroid adenomas, neoplasia appears to be rather rare in raccoons. 4, 5 In a retrospective survey of more than 400 raccoon necropsies, 2 cases of neoplasia, an astocytoma of the brain, and a fibroma of the skin were seen. 2 A review of neoplasms of raccoons found records of skin fibroma, pancreatic adenoma, thyroid adenoma and adenocarcinoma, brain astrocytoma, nasal adenocarcinoma, and intestinal adenocarcinoma. Since then, 4 other neoplasms of raccoons have been recorded. These were lymphosarcoma, adrenal gland adenomas, hepatocellular adenoma, and viral papillomatous growths on the skin of lower legs of raccoons; recently, a transitional cell neoplasm of urinary bladder was described in a raccoon housed in a laboratory. 4, 5
As mentioned previously, one other astrocytoma of the brain has been described previously in a raccoon. 2 In that case the neoplasm involved only the right cerebral hemisphere, posterior to the olfactory bulb. However, in that case report the description did not include immunohistochemical examination for the presence of GFAP.
Although the astrocytoma in the raccoon described in this report had extensively infiltrated neural tissues and had resulted in extensive neurogenic atrophy of the neck, shoulders, and leg muscles, the animal had managed to survive in the wild. The raccoon probably had considerable difficulties in climbing and obtaining food, and its survival in the wild can be partly attributed to the regular feeding by the owners of the home in the area where the animal had resided.
Footnotes
Acknowledgements
We thank Dr. Brian Summers, Cornell University, New York, for immunohistochemistry and expert advice; James Fosse and Michael Marti, NADC, Iowa for the photographs; and Martha Church, Ginny Montgomery, and Micky Fenneman, NADC, Iowa, for technical assistance.