
Abstract
A 7-year-old male Belgian Shepherd dog was presented with sudden onset of lateral recumbency and tetraparesis. At the level of the third cervical vertebra, magnetic resonance imaging demonstrated an intrameningeal and intramedullary mass lesion. The animal was subsequently euthanatized. A necropsy revealed a semitranslucent solid mass infiltrating dorsal and ventral dura mater and the spinal cord. Histologic examination revealed a lobulated pleomorphic mass, mainly resembling undifferentiated cartilage interspersed by spindle-shaped and polygonal cells with highly vacuolated cytoplasm (physaliphorous cells). Immunohistochemistry of the tumor cells demonstrated dual expression of vimentin and cytokeratin. Based on the histologic and immunohistochemical results, the diagnosis of a chordoma with chondromatous component was made.
According to the World Health Organization classification of tumors, chordomas are currently classified as tumors of notochordal origin 15 and are characterized by dual expression of epithelial and mesenchymal proteins. 6 Chordomas are believed to originate from the notochord and may arise anywhere along the vertebral column but most commonly involve the cranial and caudal limits of the axial skeleton. Most notochord remnants are extradural, and, in most species, chordomas are more commonly bone tumors than central nervous system (CNS) tumors. 2, 19 Chordomas are uncommon in humans and rare in animals; up to now, only a few reports are available from dogs, 7, 14, 17, 18 rats, 21 minks, 9 ferrets, 6, 11, 22 and one cat. 4 Apart from ferrets, where this tumor is usually located on the tip of the tail, 6 they mainly occur in the sacrococcygeal and sphenooccipital region. 10, 15, 16 In rats, these tumors are most commonly located in lumbosacral vertebrae, 21 whereas, the single feline chordoma developed lateral to the cervical vertebrae. 4 Interestingly, besides the cervical and sacrococcygeal vertebrae, brain, spinal cord, and skin are reported sites for chordomas in the dog. 7, 14, 17, 18
In humans and animals, chordomas are usually slowly growing and locally destructive. 16, 19 The rate of recurrence after surgical removal is high in human chordomas. 10 Metastases are described in humans, 1, 5, 10, 12 rats, 21 and ferrets, 22 as well as in the single feline case. 4 Up to now, chordomas have not been reported to metastasize in dogs.
In ferrets 6 and mink, 9 chordomas usually show chondromatous components. In humans, besides the classical chordoma, a chondroid type marked by the presence of cartilage, was described. 13 To our knowledge, this is the first immunohistochemically confirmed case of a cervical spinal chordoma with a chondromatous component in a dog.
This report describes the case of a chordoma with a chondromatous component in a 7-year-old male Belgian Shepherd dog. The animal was referred to the University of Veterinary Medicine Vienna with the history of acute tetraparesis and recumbency; there was no evidence of trauma before the onset of clinical symptoms. A neurologic examination revealed miosis of the left eye and nonambulatory tetraparesis characterized by absent postural reactions in all limbs and increased muscle tone in the left thoracic and left pelvic limbs; the segmental spinal reflex was moderately exaggerated in the left thoracic limb. Palpation of the thoracolumbar spine and motion of the neck was free of pain. The urinary bladder was large and difficult to express. Besides a mild blood leukocytosis (18,990 cells/μl), cytology of cerebrospinal fluid revealed neutrophilic pleocytosis (19 cells/μl) and a mildly elevated specific gravity (1.015) by a normal total protein level. According to the results of neurologic examination, myelopathy from the first to the fifth cervical vertebra was assumed, and the dog was referred to magnetic resonance imaging (MRI).
MRI, including dorsal T1, sagittal T2, transverse T2-like (CBASS), and dorsal STIR (short tau inversion recovery, fat suppression) images, revealed a mass within the left side of the spinal cord at the level of the third cervical vertebra (C3). Compared with the unaffected spinal cord tissue, the lesion appeared hyperintense on transverse T2-like weighted image. The intervertebral disc between the second cervical vertebra and C3 had a reduced volume and signal on T2-weighted images. The results of the MRI were interpreted as a noncompressive disc disease or spinal-cord mass lesion.
Physical therapy, treatment with oral prednisone (Prednisolon; Nycomed Austria GMBH) (0.5 mg/kg q 12 hours), and oral antibiotics (sulfonamide-trimethoprim), as well as urethral catheterization were performed. The dog showed no clinical improvement after 14 days of conservative therapy and was euthanatized.
A necropsy revealed an irregularly shaped semitranslucent solid mass infiltrating the spinal cord and the dorsal and ventral dura mater at the site of C3 (Fig. 1); the mass had a maximal laterolateral diameter of about 4 mm and a craniocaudal extent of 1.5 cm. On histologic examination, the lobular tissue consisted mainly of pleomorphic chondrocytic cells surrounded by cartilaginous intercellular matrix, highly resembling chondrons of physiologic cartilage (Fig. 2), revealing positive results in Ladewig staining. The lobules were interspersed by undifferentiated, pleomorphic spindle-shaped mesenchymal cells with indistinct cell borders (Fig. 3), surrounded by little fibrous tissue. Beside these cells, a population of polygonal, physaliphorous cells, was also present within the chondroid lobules (Fig. 4). Some of them showed a marginal nucleus and a markedly vacuolated cytoplasm with periodic acid–Schiff positive granules. Mitotic figures were not present. Adjacent to the chondroid mass severe acute malacia with numerous gitter cells was present. Immunohistochemistry by using antibodies against vimentin (1 : 500, BioGenex, San Ramon, CA, USA) revealed intense reactivity of physaliphorous and spindle-shaped cells, with some of the latter also expressing cytokeratin (1 : 500, Boehringer Ingelheim, Ingelheim, Germany). Furthermore, most chondrocytic cells were strongly immunoreactive with antibodies against vimentin and cytokeratin (Fig. 5). By using antibodies against S-100 protein (1 : 1000, DakoCytomation, Glostrup, Denmark), the number of immunopositive cells was smaller and mainly limited to physaliphorous cells, whereas no immunoreactivity was found in the entire mass for glial fibrillary acidic protein, (1 : 1000, DakoCytomation) or neuron-specific enolase, (1 : 5000, Chemicon/Millipore, Billerica, MA, USA).
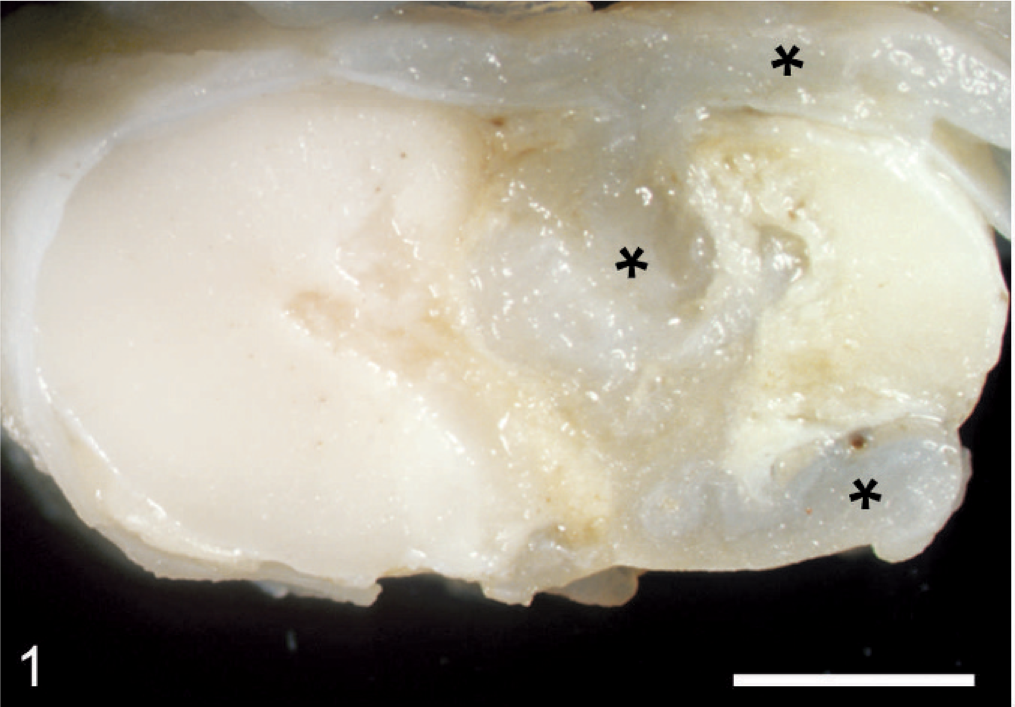
Spinal cord; dog. Macroscopic view of the spinal chondroid chordoma (asterisks) at the site of C3 with complete dural infiltration. Bar = 3 mm.
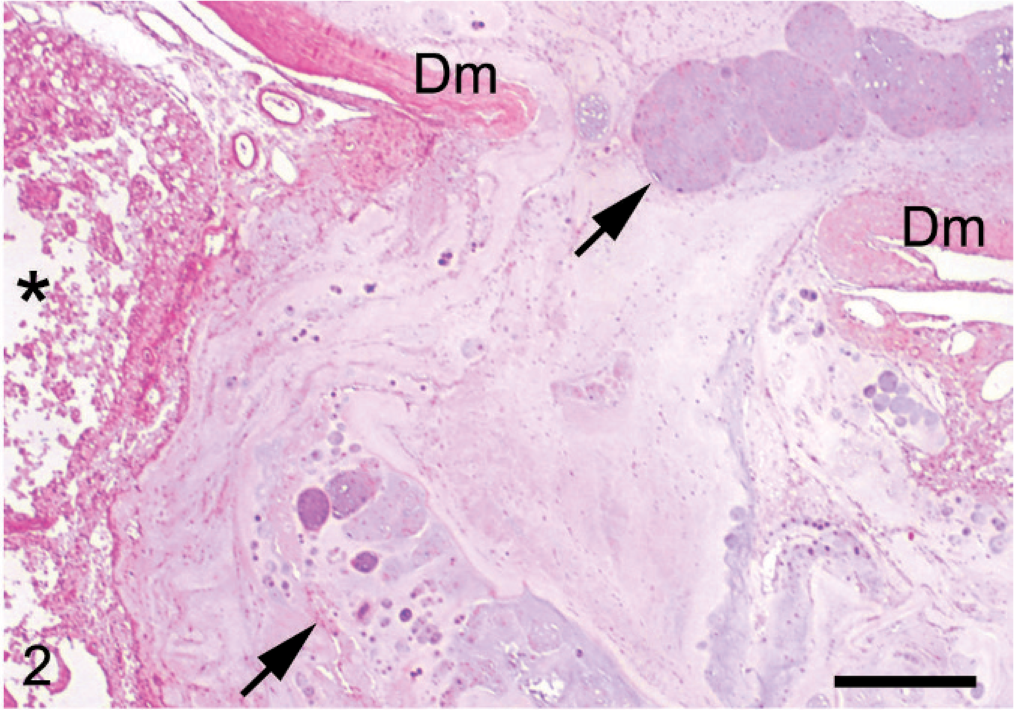
Spinal cord; dog. Chordoma, consisting of variably differentiated chondroid tumor matrix (arrows). Note tumor extension with full-thickness infiltration of dura mater (Dm) and malacia of adjacent spinal cord tissue (asterisk). HE. Bar = 500 μm.
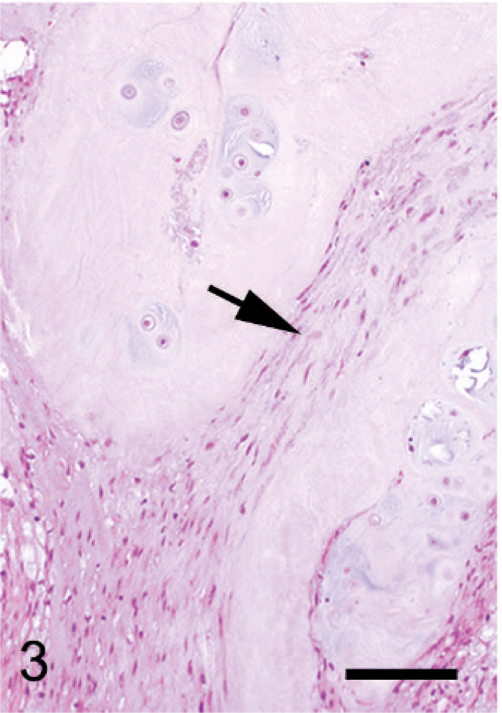
Spinal cord; dog. Lobulated chondroid tumor matrix interspersed by undifferentiated spindle-shaped mesenchymal cells (arrow). HE. Bar = 100 μm.
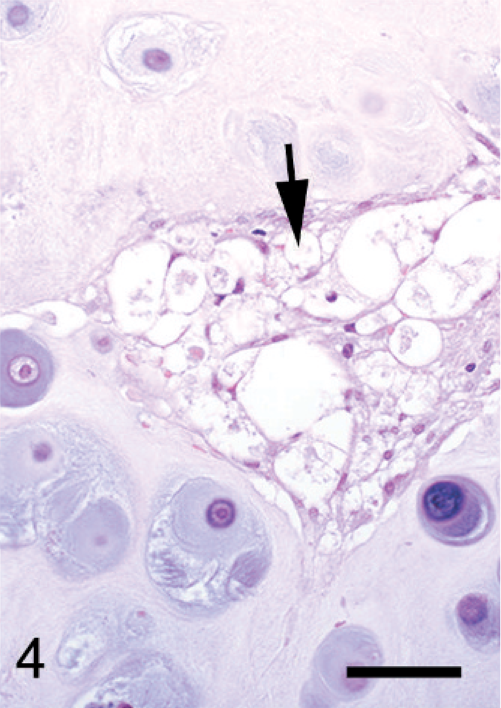
Spinal cord; dog. Typical vacuolated (physaliphorous) cells (arrow) within the chondroid tumor matrix. HE. Bar = 50 μm.
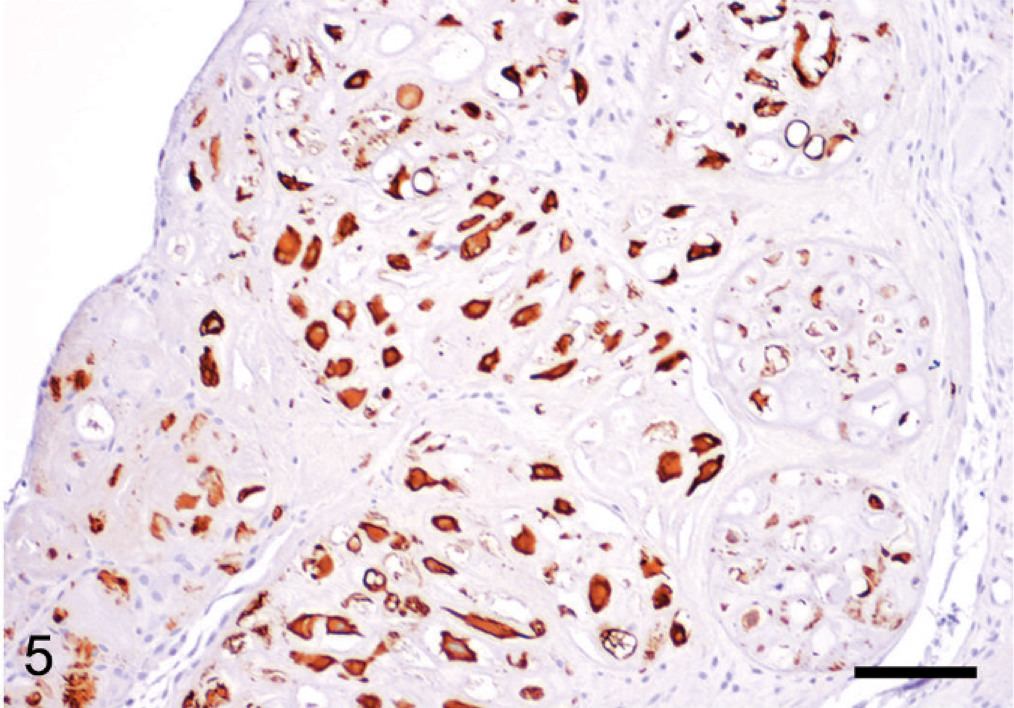
Spinal cord; dog. Strong expression of cytokeratin by chondroid tumor cells; avidin-biotin complex immunohistochemistry with monoclonal anti-cytokeratin antibody, hematoxylin counterstain. Bar = 50 μm.
Since the first description of chondroid chordoma, there has been controversy about the existence of this tumor variant; some investigators suggest chondroid chordoma to represent low-grade chondrosarcoma. 3 However, Gottschalk et al. 8 demonstrated, with matrix gene expression analysis and molecular in situ localization techniques, the chondrocytic differentiation potential of tumorous chordoid cells as a characteristic facet of chordomas and showed that chondroid chordomas are variants of this tumor. The macroscopic appearance of chordomas described in humans and different animal species fits the well-defined, lobulated, and semitranslucent mass in the cervical cord of this dog.
Human chordomas are histologically classified as classical, dedifferentiated, and chondroid variants. The latter are distinguished from the classical form by the presence of a chondromatous component and spindle cells. Because survival rates are higher and prognosis is better in chondroid chordomas, this variant is separated from the classical type. 13, 20
Whereas, chordomas reported in rats 21 and a cat 4 are most consistent with classical types, in ferrets, 6, 11 mink, 9 and the dog of this report, they contain cartilage and physaliphorous cells and, therefore, resemble human chondroid chordomas. The different tumor components are arranged in lobules separated by fibrous stroma and physaliphorous cells, often surrounded by a mucinous extracellular matrix. Mitotic figures are rare in the ferret 6 and not seen in the mink 9 nor in our dog.
Three cases of canine chordomas are reported, but just two of them were investigated by immunohistochemistry. One case of a canine chordoma with localization in the skin adjacent to the second coccygeal vertebra was described as lobulated, nonencapsulated, and firm. The tumor contained a population of spindle-shaped cells arranged in loose bundles, supported by mucinous, fibrovascular stroma surrounded by a population of polygonal cells, some of which resembled physaliphorous cells; mitotic figures were present. 17 Another skin-located chordoma was soft and composed of creamy white, semitranslucent nodules divided by connective tissue septa. On microscopic examination, the main cell groups corresponded to physaliphorous cells. Scattered among those cells were small polygonal or ovoid cells; multinucleated tumor cells were present but mitotic figures were rare. 14 In a 4-year-old Labrador Retriever, a chordoma developed in the lumbar spinal cord. The tumor consisted of small stellate and physaliphorous cells with irregular lobules of hyaline cartilage and bone; mitotic figures were scarce. 18 This case is most like ours; however, there was no immunohistochemical confirmation of a chondromatous component.
The clinical presentation and MRI examination were suggestive of protrusion or extrusion of a disc in this case. The differential diagnosis for a mass within the spinal cord should include primary tumors of the CNS and tumors of the vertebral column, such as chondrosarcomas and osteosarcomas, which can be differentiated from chordomas by immunohistochemistry. The immunohistochemical expression of both epithelial (cytokeratin) and mesenchymal (vimentin) proteins by tumor cells in this dog is consistent with results of previous studies of chordomas in various species. 6, 16, 17, 21 Furthermore, as described in chordomas of humans 20 and ferrets, 6 some tumor cells expressed S-100 protein as well.
In conclusion, this report demonstrates, that the histologic appearance and protein expression profile of this canine chordoma are mostly consistent with chondroid chordomas in humans and that immunohistochemistry is more valuable than routine histology or MRI for differentiation of physiologic cartilage from chordoma and for detailed definition of tumors with chondroid morphology.
Footnotes
Acknowledgements
The authors thank Mag. Dieter Malleczek for performance and evaluation of the MRI, Klaus Bittermann for excellent photographic work and Nora Nedorost and Karin Fragner for their skilled technical assistance.