
Abstract
Odontoameloblastoma (OA) is a mixed odontogenic tumor that is an ameloblastoma with concurrent histologic evidence of odontoma differentiation. As a mixed tumor, OA is a tripartite lesion comprised of neoplastic odontogenic epithelium, induced dental ectomesenchyme (dental pulp), and mineralized dental matrix. Although rare, OA represents a diagnostic conundrum, as it is histologically closely related to 2 other mixed odontogenic tumors: odontoma (complex and compound) and ameloblastic fibro-odontoma. Herein we describe an OA arising from the mandible of a 4-mo-old Fischer 344 rat that had been exposed in utero to the mutagen ENU (N-ethyl-N-nitrosourea), and a naturally occurring lesion in a 2-y-old Appaloosa horse. In order to satisfy the diagnostic criteria for this lesion, mineralized dental matrix in relationship to neoplastic odontogenic epithelium must be identifiable within the OA lesion. This group of odontogenic tumors is differentiated by the degree to which the dental matrix is organized and the relative proportions of pulp ectomesenchyme, odontogenic matrix, and odontogenic epithelium.
Odontogenic tumors arise from odontogenic elements within the jaws and adjacent gingival mucosa of humans and veterinary species. As a result of the myriad combinations and proportional ratios of the cellular and matrical components present in odontogenic tumors, these lesions are histologically interesting but can also pose a diagnostic challenge. Odontogenic tumors are derived from the germinal tissues of embryonic teeth; to various degrees, these tumors recapitulate the intricate inductive processes of tooth embryogenesis.
Odontoameloblastoma (OA) is a rare tumor in both humans 1 and veterinary species. In humans, it is a locally aggressive oral tumor that occurs in both the mandible and maxilla and is similar in both behavior and prognosis to ameloblastoma. 1 Most cases are associated with displaced or unerupted teeth. Radiographically, OA appears as a well-defined unilocular or multilocular radiolucent lesion with variable amounts of interspersed radiopaque material.
OA has historically been associated with a problematic and closely related term that is not directly synonymous, namely ameloblastic odontoma. Today, ameloblastic odontoma is considered to represent either (1) OA or (2) ameloblastic fibro-odontoma. 5 Because of this taxonomic imprecision, the use of this older term has been discouraged. Unfortunately, over the past ~50 y, the term ameloblastic odontoma has become enmeshed in the veterinary pathology literature. As a result, our current understanding of previously reported ameloblastic odontoma lesions is a bit muddled. Ameloblastic odontoma lesions have been described in horses,7,9,10 dogs,6,8 llama, 11 rats, 13 and ox. 12 In the 4 peer-reviewed cases of OA described in veterinary species—Japanese monkey (syn. Japanese macaque; Macaca fuscata), 14 calf, 4 rat, 2 and sheep 3 —the mandible appears to be a favored anatomic site.
OA is a locally aggressive, expansile lesion that does not metastasize. The bone of the jaw and alveolus is often focally destroyed and infiltrated by neoplastic odontogenic epithelium in a manner reminiscent of ameloblastoma. Architecturally, the odontogenic epithelium is arranged in follicles, plexiform ribbons, and/or anastomosing trabeculae embedded in a scant fibrovascular to dental pulp-like stroma. In order to satisfy the diagnostic criteria for this lesion, mineralized dental matrix must be identifiable within the OA lesion. Herein we describe OA arising from the mandible of both a Fischer 344 rat and an Appaloosa horse.
A 4-mo-old male Fischer 344 rat was culled from an experimental protocol because of a firm swelling of the left mandible. At gestation day 19, the rat’s pregnant dam had been given the mutagen ENU (N-ethyl-N-nitrosourea, C3H7N3O2) intravenously at a rate of 50 mg ENU/kg body weight. The rat was euthanized according to University of California–Davis IACUC protocols and submitted for autopsy. A complete set of tissues was collected for microscopic examination and preserved in 10% buffered formalin. Tissues were fixed for 48 h, and the mandible was demineralized in 10% formic acid for ~96 h, sectioned, and embedded in paraffin. Five-µm thick slides were cut and stained with hematoxylin and eosin according to standard protocols. Immunohistochemistry was performed using a murine anti-pancytokeratin monoclonal antibody (Lu-5, Biocare Medical, Concord, CA). Immunohistochemistry was performed according to protocols provided by the manufacturer (Biocare Medical).
On postmortem examination of the Fischer rat, a 2.5 × 2 × 2 cm multilobulated mass that expanded and destabilized the left mandible was identified. The mandibular incisors were crossed (malocclusion). The mandibular mass on section was dark red and had numerous blood-filled cystic spaces interspersed with hard white tissue.
Microscopically, the bone of the rat’s left mandible was expanded and distorted by an invasive, unencapsulated, multinodular neoplasm comprised of neoplastic odontogenic epithelium, associated ribbons of eosinophilic matrix, and a supporting fibrous stroma (Fig. 1). Approximately 90% of the examined neoplastic tissue was odontogenic epithelium. Islands of odontogenic epithelium were arranged as follicles and irregularly margined anastomosing trabeculae with rounded botryoid protuberances extending into the adjacent fibrous stroma (Figs. 1, 2). The islands had a crowded, multilayered, peripheral palisade of columnar-to-cuboidal epithelial cells with anti-basilar nuclei (neoplastic ameloblasts). Centrally, the odontogenic structures had stellate epithelial cells with long, strand-like intercellular junctions (stellate reticulum; Figs. 2, 3). Scattered odontogenic structures demonstrated central keratinization with dystrophic mineralization or abrupt central necrosis and cyst formation. The cystic structures were either empty or contained blood. Within the odontogenic epithelium, 20 mitotic figures were present in ten 400× fields. Neoplastic epithelium and mucosal epithelium within the section (positive control, not shown) stained with a pancytokeratin immunohistochemistry assay (Fig. 4).
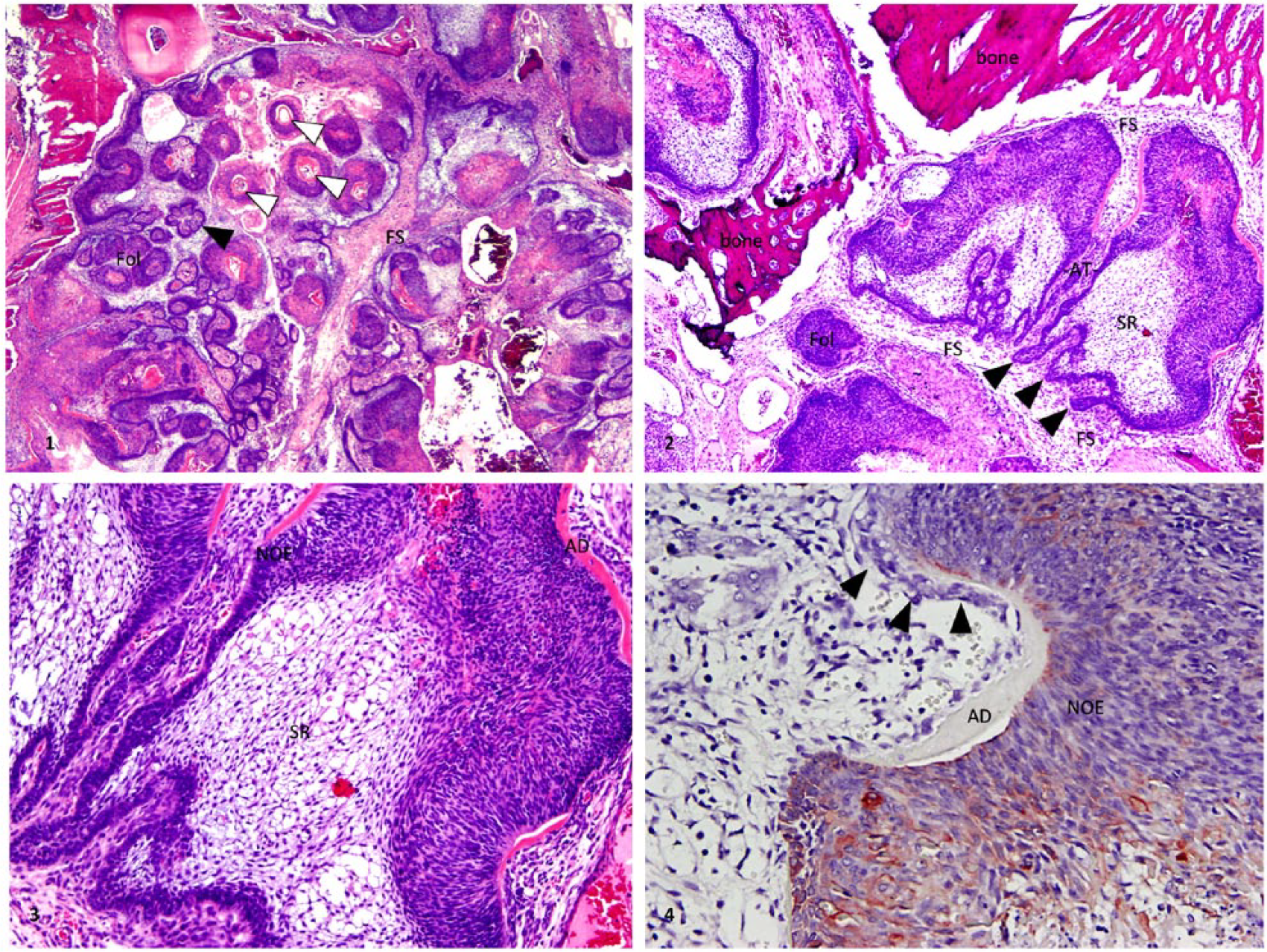
Mandibular odontoameloblastoma in a Fischer rat.
Multifocally, variably thick ribbons of brightly eosinophilic matrix with an amorphous to finely fibrillar structure lay adjacent to the palisading ameloblasts (atubular dentin). Rarely, this eosinophilic matrix had lens-like lacunae with embedded small pyknotic cells (osteodentin). The dental matrix was arranged as linear, serpentine, ring, and cup-like structures. On the matrical face opposite the ameloblasts, infrequent aggregates of polygonal mesenchymal cells forming jumbled palisades (odontoblasts) were variably present (Fig. 4). The stroma was comprised of variably dense sheets and streams of mesenchymal cells with bland ovoid nuclei. Several histologically normal remnant tooth cross-sections were embedded within the neoplastic tissue. The mandibular cortex was thin and multifocally replaced by parallel plates of woven bone (periosteal hyperplasia).
A 2-y-old Appaloosa gelding had a hard, non-painful, smooth, expansile mass of the left mandible that the owner had become aware of ~1 mo prior to presentation. The mass was 16 × 13.5 × 7.5 cm, bony, and extended from the first to the third molar tooth. Computed tomography (CT) examination was performed on the mandibular lesion. The mass formed a large, cystic expansion of the left mandibular medullary cavity. The lesion was associated with the roots of the permanent second and third molar teeth. The deciduous third molar was impacted (unerupted) and was encased by a thin rim of bone; the medial (lingual) aspect of the mandibular cortex was thin. The CT results were considered to be most consistent with a neoplasm of dental origin. At the request of the owner, the gelding was euthanized and a routine autopsy performed. Tissues were processed for microscopic examination as described above for the rat.
On transverse section, the mass was relatively well-circumscribed and consisted of mineralized, irregularly shaped, heterogeneous tissue associated with the root of the second molar (Fig. 5). The ventral aspect of the mandible was cystic and fluid-filled. The tissue surrounding the second molar was firm, brown-to-tan fibrous tissue admixed with numerous white, hard nodules 0.2–0.6 cm diameter. The remainder of the autopsy examination was unremarkable.
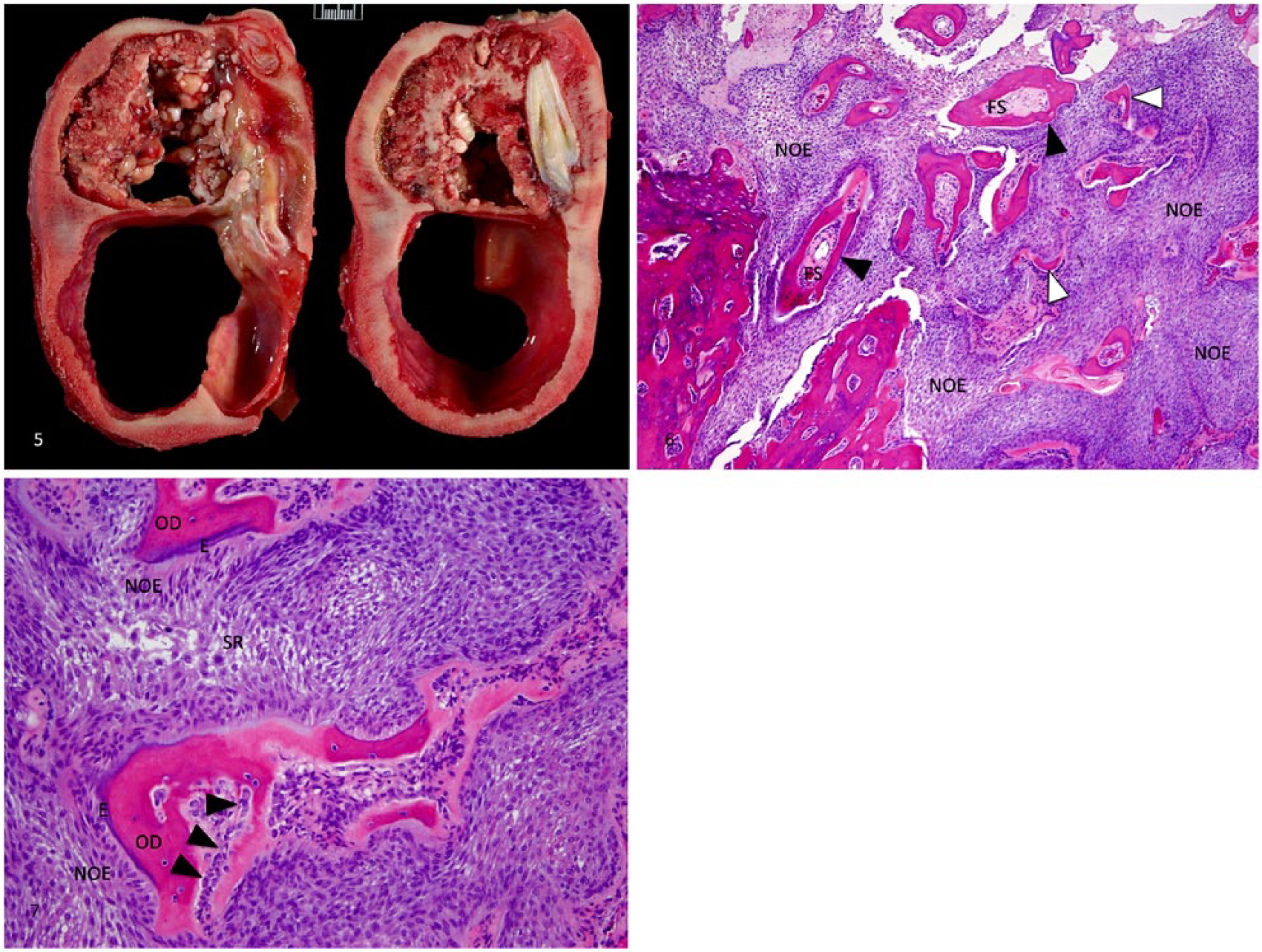
Mandibular odontoameloblastoma in a horse.
Microscopically, the mandibular architecture was effaced by neoplastic odontogenic epithelium forming invaginated sheets and nodules, with closely associated ribbons of eosinophilic matrix and minimal fibrous stroma. The examined regions of the tumor were comprised of ~70% odontogenic epithelium and 30% matrix (Fig. 6). The epithelium was bordered by a crowded palisade of cuboidal-to-columnar cells with variably evident, round-to-ovoid, anti-basilar nuclei and basilar cytoplasmic clearing (neoplastic ameloblasts). Centrally, the epithelial structures were comprised of compressed squamoid to loosely arranged stellate epithelial cells with long intercellular bridges (stellate reticulum). Variably thick, branching, serpentine ribbons and rings of atubular, homogeneous to finely fibrillar eosinophilic matrix with small numbers of embedded pyknotic cells (osteodentin) separated the epithelial sheets and nodules. Multifocally, the osteodentin contained coalescing botryoid globules or linear strips of purple enameloid matrix. A jumbled palisade of cuboidal mesenchymal cells (odontoblasts) multifocally aligned along the ribbons of osteodentin opposite the ameloblasts (Fig. 7). In some regions of the tumor not depicted in our figures, osteodentin with intermixed basophilic-staining globules or ribbons of enameloid matrix formed extensive, interlinking sheets. Broad, anastomosing trabeculae and sheets of cemento-osseous bone, often with amphophilic-to-basophilic matrical staining, were at the lesion periphery.
The mandibular lesions of both the rat and horse were considered to be histologically consistent with OA. ENU, delivered to the Fischer rat in utero, is an alkylating agent and potent mutagen, and may have played a role in the development of the mandibular OA. In support of this speculative pathogenesis, 4 rats exposed orally multiple times to a high dose of the mutagen N-butylnitrosourea developed ameloblastic odontomas of the mandible. 13 Although the researchers used the older and somewhat ambiguous term ameloblastic odontoma, their histologic description of the lesion is consistent with a diagnosis of OA.
Odontogenic tumors are classified by how closely and completely they parallel the processes of tooth embryogenesis. The simplest odontogenic tumors are comprised of odontogenic epithelium alone. The complexity of these lesions increases as they progressively demonstrate more sophisticated features of tooth embryogenesis. During normal tooth embryogenesis, a cap-like structure of odontogenic epithelium (ameloblasts) induces the differentiation of the subjacent ectomesenchyme to develop into the dental papilla (dental pulp). The dental pulp then differentiates into odontoblasts, which produce a ribbon of mineralized dental matrix (dentin) at the ameloblast–odontoblast interface. Subsequently, the presence of dentinal matrix induces the palisading ameloblasts to produce a layer of enamel along the surface of the dentinal matrix. This process of ameloblasts signaling odontoblasts to produce dentin, which then signals ameloblasts to produce enamel, is called reciprocal induction. In this manner, the tooth crown is formed.
Mixed odontogenic tumors are composed of neoplastic odontogenic epithelium and induced pulp ectomesenchyme. Whether the mixed odontogenic tumor in question also demonstrates mineralized dental matrix is diagnostically relevant, for without it, the mixed odontogenic tumor is an ameloblastic fibroma or, in cats, feline inductive odontogenic tumor. Three closely related odontogenic tumors concurrently demonstrate the tripartite histologic features of (1) neoplastic odontogenic epithelium, (2) pulp ectomesenchyme, and (3) mineralized dental matrix (some combination of tubular dentin, atubular dentin, osteodentin, and/or enamel matrix): OA, odontoma, and ameloblastic fibro-odontoma (AFO). In a given lesion, these 3 histologic features are not necessarily equally represented, and some of the tissues may even be difficult to identify, particularly the pulp ectomesenchyme. OA, odontoma, and AFO are differentiated by the degree to which the dental matrix is organized and the relative proportions of pulp ectomesenchyme and odontogenic epithelium (Table 1).
Diagnostically relevant features of mixed odontogenic tumors.
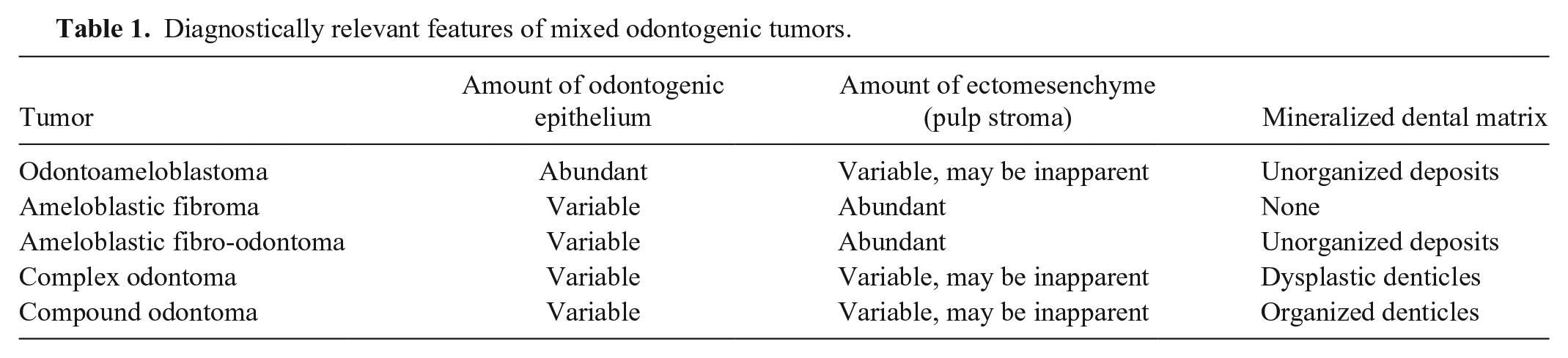
Of the 3 tumors in this group, OA has the greatest proportion of neoplastic epithelium; the majority of the tumor should be neoplastic odontogenic epithelium. OA can be thought of as an ameloblastoma that also produces mineralized dental matrix; that is, OA is a cross between an ameloblastoma and an odontoma. This interpretation is implicit in the name. The other 2 entities in this category, odontoma and AFO, demonstrate similar histologic features, but in different proportions. Odontomas have a greater proportion of mineralized dental matrix and either form recognizable tooth-like structures (compound odontoma) or a chaotic mixture of the various odontogenic elements (complex odontoma). We have classified the mandibular lesion in the rat as an OA given the abundance of neoplastic odontogenic epithelium. However, a complex odontoma is a plausible differential diagnosis for this lesion. OA has a relative abundance of neoplastic epithelium, whereas a complex odontoma has an abundance of dental matrix, which creates the impression of dysplastic denticles (Table 1). AFO has the greatest proportion of dental ectomesenchyme. In AFO lesions, a substantial proportion of the lesion is comprised of basophilic to pale-staining, induced pulp ectomesenchyme. This tissue forms extensive sheets, generally with homogeneous, hyperplastic, but non-neoplastic cytologic features. The other elements of the AFO lesion (odontogenic epithelium and mineralized dental matrix) are embedded within the sheets of pulp ectomesenchyme.
For AFO and OA, the mineralized dental matrix is often present as thin, atubular, eosinophilic wedge, ribbon, or ring-shaped structures palisaded on one face by cytokeratin-positive columnar epithelial cells (odontogenic epithelium-derived ameloblasts), and along the other face by vimentin-positive, densely packed, jumbled aggregates of polygonal-to-fusiform cells (odontogenic ectomesenchyme-derived odontoblasts). The interposed matrical material is histologically consistent with tubular dentin, atubular dentin, or osteodentin. Osteodentin is rapidly formed, tertiary dentin that often entraps odontoblasts, and demonstrates few (if any) recognizable dentinal tubules; it has a histologic appearance reminiscent of bone. 2 The mineralized component of the dental matrix is typically removed during histologic preparation. Enamel matrix may also be identified in OA lesions, deposited along the surface of the dentin, presumably by ameloblasts. However, because enamel matrix is almost completely mineral (~96%), it is often dissolved out of the section during the demineralization procedure. It is important to distinguish between mineralized dental matrix and metaplastic bone, given that such bone may form within the tumor stroma. Although osteodentin and osteoid can be histologically similar, the thin, ribbon or ring-like appearance of neoplasm-associated dentin is a useful diagnostic feature. Metaplastic bone is more typically arranged in anastomosing trabeculae that may form broad sheets and be covered by palisades of mesenchymal cells (osteoblasts). It is our hope that this report of OA arising from the mandible of both a Fischer 344 rat and an Appaloosa horse contributes to the sparse literature on a rare and potentially confusing entity. As pathologists with an interest in odontogenic neoplasia, we hope to have clarified the diagnostic criteria for the various mixed odontogenic tumors.
Footnotes
Acknowledgements
We thank the UC Davis Comparative Pathology Laboratory, Drs. Steve Griffey and James Angelostro for contributing the rat odontoameloblastoma case, and Drs. Megan Jones and Charles Mohr for the equine gross image and autopsy. We are also grateful for the technical expertise of the UC Davis histotechnology staff and Dr. Kirsten Murphy for editing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.