
Abstract
Lymphoma is the most common nasal cavity tumor in cats, yet few reports specifically address the anatomic, immunohistologic, and cytologic features of this neoplasm. Fifty cats were diagnosed with lymphoma at necropsy, via biopsy or by cytology alone. Ten cats displayed multiorgan involvement, and in 2 of these the involvement was limited to the cerebellum and frontal cortex, respectively. Of the tumors, 41 of 50 (82%) were classified as nasal lymphoma, 5 of 50 (10%) were classified as nasopharyngeal lymphoma, and 4 of 50 (8%) involved both nasal and nasopharyngeal tissue. Histologically, all were considered diffuse lymphoid neoplasms and no cats displayed features of follicular lymphoma. Of the 44 cases available for slide review by the pathologist, 40 of 44 (91%) were classified as immunoblastic lymphoma, 2 of 44 (5%) as diffuse large cell, and 1 as diffuse mixed; 1 was unclassified. Of the 45 cats for which immunohistochemical stains were available, 32 were uniformly positive for CD79a, 7 were uniformly CD3 positive, and 6 had a mixed population of CD79a and CD3 cells. Epithelioptropism was exhibited in 4 of 5 (80%) cats in which there was sufficient epithelium present for evaluation. Of those 4, 3 were B-cell and 1 was a granulated T-cell lymphoma. In the 21 cats which nasal cytology was performed, 15 were cytologically diagnosed with lymphoma; the diagnoses in the remaining five cats were inflammatory (n=4), normal lymphoid tissue (n=1), or nondiagnostic (n=1). The most common biochemical abnormalities were panhyperproteinemia in 26/46 (57%) of cats and hypocholesterolemia in 11/46 (24%) of cats.
Keywords
Nasal lymphoma is the most common nasal tumor in cats, exceeding other neoplasms and inflammatory diseases in recent studies. 14, 19 Nasal lymphoma is reported as generally restricted to the nasal cavity; systemic spread is only occasionally reported. 8, 12– 14, 19 A discrepancy in immunologic characterization of feline nasal lymphoma has been noted, and T-cell lymphomas are reported to account for either 5%, 8%, or 29% of cases studied. 8, 19, 21 Anatomic location, histopathologic classification, and immunophenotype could notably affect treatment recommendations and response to therapy. In one human study, primary nasal lymphoma and nasopharyngeal lymphoma were noted to behave as biologically distinct entities, in which the nasal lymphomas demonstrated a higher frequency of T-cell tumors and a worse prognosis. 17 Whereas previous animal studies have investigated the immunophenotype and histologic classification of this neoplasm, none have made the distinction between nasal and nasopharyngeal lymphoma, nor have they documented the cytologic features of this neoplasm. 8, 19
Biopsy is considered the gold standard for definitively diagnosing nasal lymphoma, yet cytology has diagnostic utility in the form of brush cytology, nasal washes, nasal swabs, biopsy impression smears, and fine-needle aspiration. Few studies have investigated the role of cytology in the diagnosis of nasal lymphoma in cats. Caniatii et al. 6 evaluated the use of brush cytology in the diagnosis of chronic intranasal disease in cats with an overall 86.8% agreement between the diagnosis of inflammatory conditions versus neoplasia, resulting in a sensitivity of 72.7% and a specificity of 96.8%. Seventeen samples were classified by brush cytology as neoplastic, of which 9 were confirmed by biopsy as carcinoma, 6 as lymphoma, and 1 as osteosarcoma. One false-positive diagnosis of lymphoma was made by cytology.
The aim of this study was threefold: 1) to describe the anatomic, histologic, and immunophenotypic features of nasal lymphoma diagnosed at our institution; 2) to investigate the utility of cytology in the diagnosis of feline nasal lymphoma; and 3) to document clinicopathologic abnormalities in cats with feline nasal lymphoma.
Materials and Methods
Selection of cases
A computer search of the medical records and pathology databases of cats examined at the Matthew J. Ryan Veterinary Hospital of the University of Pennsylvania, between January 1988 and August 2005 was performed to identify cats diagnosed with lymphoma in the nasal cavity by cytology, biopsy, and/or necropsy. Fifty cats were included on the basis of a cytologic or histopathologic diagnosis of nasal lymphoma and the presence of a complete medical record. Data collected from the medical records included presenting complaint, duration of clinical signs, physical examination findings, clinicopathologic results (complete blood count [CBC], biochemistry panel), cytologic or histopathologic results, and imaging study results.
Location
The location of the primary tumor was categorized as nasal or nasopharyngeal based on histopathology and imaging modalities, including skull radiographs, rhinoscopy, computed tomography (CT), and/or magnetic resonance imaging (MRI).
Histologic and cytologic preparation
All tissues for histologic evaluation were fixed in 10% neutral-buffered formalin, and routinely prepared slides were stained with hematoxylin and eosin (HE). Cytology preparations were made from impression smears of a nasal mass biopsy (9/21), fine-needle aspirates of the mass (5/21), direct smears of nasal flush fluid (3/21), or nasal swab (1/21). Method of collection was undocumented in 3 cats. Cytology preparations were stained with buffered Wright's-Giemsa. Modifiers were applied to cytologic diagnoses of lymphoma including certain, probable, and possible. A case was diagnosed with certainty if the quality of the smears was good or excellent, if 90% of the nucleated cells were lymphoblasts, and if the remaining 10% of cells were inflammatory cells other than small lymphocytes and plasma cells. A probable diagnosis was applied if the slide quality was poor to fair but lymphoblasts were present in high numbers or if a mixed lymphoid population was present with >90% lymphoblasts. Possible lymphoma was diagnosed in 1 cat in which the majority of cells were broken except for few intact lymphoblasts and in 1 cat that displayed a presumed high percentage of lymphoblasts (>90%); however, the slides had been exposed to formalin resulting in poor staining qualities that obscured definitive cellular morphology.
Immunohistochemical staining
Of the 50 cats, 45 were evaluated immunohistochemically. Two cats were diagnosed by cytology without subsequent biopsy (Nos. 11 and 13) and paraffin-embedded tissue blocks were not available for 3 cats (Nos. 12, 28, and 37). Immunohistochemical staining of paraffin-embedded 4-μm tissue sections was performed with commercially available antibodies (Dako Corporation, Carpentaria, CA) to the pan T-lymphocyte marker CD3 and B-cell antigen receptor complex CD79a. To facilitate labeling with CD3 and CD79a, tissues were pretreated with Proteinase-K (Dako Cytomation, prediluted) and high pH antigen retrieval (BioGenex, San Ramon, CA), respectively. Normal tissues containing the antigen of interest were stained in parallel for use as positive controls.
Clinicopathologic testing
A CBC was performed in 48 cats with an Abbott CELL-DYN 3500 hematology analyzer (Austin, TX) with multispecies settings. All differential leukocyte counts were determined manually by counting 100 cells. Routine serum chemistry profiles were analyzed in 46 cats using an Ortho-Clinical Diagnostics VITROS 250 (Rochester, NY). Ionized calcium concentration was determined in 16 cats using a Nova Stat Profile M (Waltham, MA). Feline leukemia virus (FeLV)/feline immunodeficiency virus testing was performed in 23 cats via S-Nitroso-N-acetylpenicillamine (SNAP) enzyme-linked immunosorbent assay combined immunoassay (IDEXX Laboratories, Westbrook, MA).
Statistical analysis
Chi-square analysis or Fisher's exact tests were used to determine if cytologic vacuolization was significantly associated with immunophenotype and/or anatomic location and if immunophenotype and anatomic location were significantly associated. Results were considered significant at P < .05.
Results
Signalment and clinical history
The most common clinical signs in cats with nasal lymphoma included nasal discharge (42/50), sneezing (34/50), decreased appetite (30/50), increased upper respiratory noise (30/50), ocular discharge (15/50), increased respiratory effort (17/50), facial deformity (14/50), stridor (13/50), wheezing (13/50), and coughing (11/50). An equal numbers of cats had unilateral versus bilateral nasal discharge. Nasal discharge was characterized as purulent (22/42), epistaxis (13/42), serous (4/42), or unclassified (3/42). Ocular discharge was characterized as serous (12/15) or purulent (3/15). Median duration of clinical signs was 60 days (range = 14 days to 1,800 days). Mean age of the affected cats was 8.9 years (range = 3 to 17 years). Breeds included domestic shorthair (n = 32) domestic long hair (n = 7), Siamese (n = 7), Maine Coon (n = 2), and Burmese (n = 1); the breed was undocumented in 1 cat.
Clinicopathologic data
Biochemical analysis was performed in 46 cats. The most common biochemical abnormality was panhyperproteinemia in 26 of 46 cats (57%); hypocholesterolemia was noted in 11 of 46 cats (24%). Hematologic abnormalities included mild to moderate lymphopenia (22/48) and moderate mature neutrophilia (14/48). Two cats had circulating lymphoblasts. No cats were hypercalcemic and 2 of 21 cats were FeLV positive, 1 of which had multiorgan involvement confirmed at necropsy (No. 48).
Imaging and lesion localization
Lesions were classified as primarily nasal or nasopharyngeal based on the tissue submitted for histopathology and results of imaging studies. Of the 50 cats, 17 (34%) had skull radiographs alone, 13 (26%) had rhinoscopy and skull CT, 9 (18%) had skull CT alone, 5 (10%) had skull radiographs and rhinoscopy, 2 (4%) had rhinoscopy alone, 1 (2%) had skull radiographs and skull MRI, and 3 (Nos. 6, 15, 50) had no imaging studies. Of these 3 cats, 2 (Nos. 6, 50) had necropsies that confirmed nasal lymphoma. Cat No. 15 had neither imaging studies nor biopsy and was classified with nasal lymphoma based on aspiration of a mass protruding through the bridge of the nose. Of 20 cats in which rhinoscopy was performed, a mass was visualized in the nasal cavity in 14 and in the nasopharynx in 4. The 2 remaining cats displayed diffusely irregular mucosal surfaces. All 23 cats that had skull radiographs under anesthesia showed evidence of nasal mass lesions; 10 of those had adjacent bony lysis. None of the 5 cats that were eventually classified with nasopharyngeal lymphoma had skull radiographs performed. Common findings on CT included a contrast-enhancing mass of soft tissue opacity that was frequently associated with extensive lysis of surrounding bone and turbinates, fluid in the nasal sinuses, and septal deviation. Excluding the case diagnosed by cytology alone, histopathology and imaging modalities resulted in the classification of 40 of the 49 tumors (82%) as nasal lymphoma, 5 (10%) as nasopharyngeal lymphoma, and 4 (8%) involved both nasal and nasopharyngeal tissue.
Diagnosis and lesion distribution
Cats were diagnosed initially at necropsy (5/50), via biopsy (43/50), or by cytology alone (2/50). For 19 cats, cytology samples were collected in addition to histopathology, resulting in a total of 21 cytologies. Of 22 cats that had antemortem oncologic full staging (n = 13) or a necropsy (n = 9), 10 demonstrated multiorgan involvement. Of 9 necropsied cats, 6 had multiorgan involvement, 2 of which were limited to brain involvement (Nos. 17 and 40). Multicentric lymphomas included 5 B-cell lymphomas (Nos. 17, 39, 40, 48, 50) and 1 granulated T-cell lymphoma (No. 6). Organs involved included small intestine (n = 2), lymph nodes (n = 2), and 1 each of liver, ocular choroid, eyelid, olfactory lobe, kidney, frontal cortex, meninges, trachea, lung, mediastinum, cribriform plate, bone marrow, and heart. Of 13 cats that underwent full oncologic staging, 4 showed evidence of metastatic disease. Central nervous system (CNS) involvement was assumed via CT in 2 cats, and ultrasonography diagnosed mesenteric lymph node involvement in 1 cat and bilateral renal involvement in another.
Histopathology
Of the nasal lymphomas available for staining, 25 of 41 (61%) were B-cell, 6 of 41 (14.6%) were T-cell, and 5 of 41 (12.2%) contain a mixed population of B-cells and T-cell. Of the 5 primary nasopharyngeal tumors, 3 (60%) were B-cell and 2 (40%) were T-cell. Of 4 cats in which both anatomic locations were affected, 2 (50%) were B-cell, 1 (25%) was T-cell, and 1 (25%) contained a mixed population of T-cells and B-cells. No significant relationship was found between immunophenotype and anatomic location (P = .89).
The National Institutes of Health (NIH) working formulation for classification of lymphoma was used to classify the histopathologic features of these neoplasms. This classification scheme was chosen to be consistent with previous large studies of feline lymphoma.12,23 All cases were considered diffuse lesions, and no cases displayed features of follicular lymphoma (Fig. 1). Of the 44 lymphoma available for slide review by the pathologists (MHG, LL), 40 (91%) were classified as immunoblastic lymphoma (Fig. 2). These lesions consisted of densely packed sheets of large lymphoblasts that frequently obliterated the normal nasal tissue. The cells had a large round to oval nucleus, a single centrally located large nucleolus, stippled chromatin, and scant to moderate amounts of eosinophilic cytoplasm. Reflecting the overall trend in immunophenotypes, 63% of the immunoblastic lymphomas were B-cell.
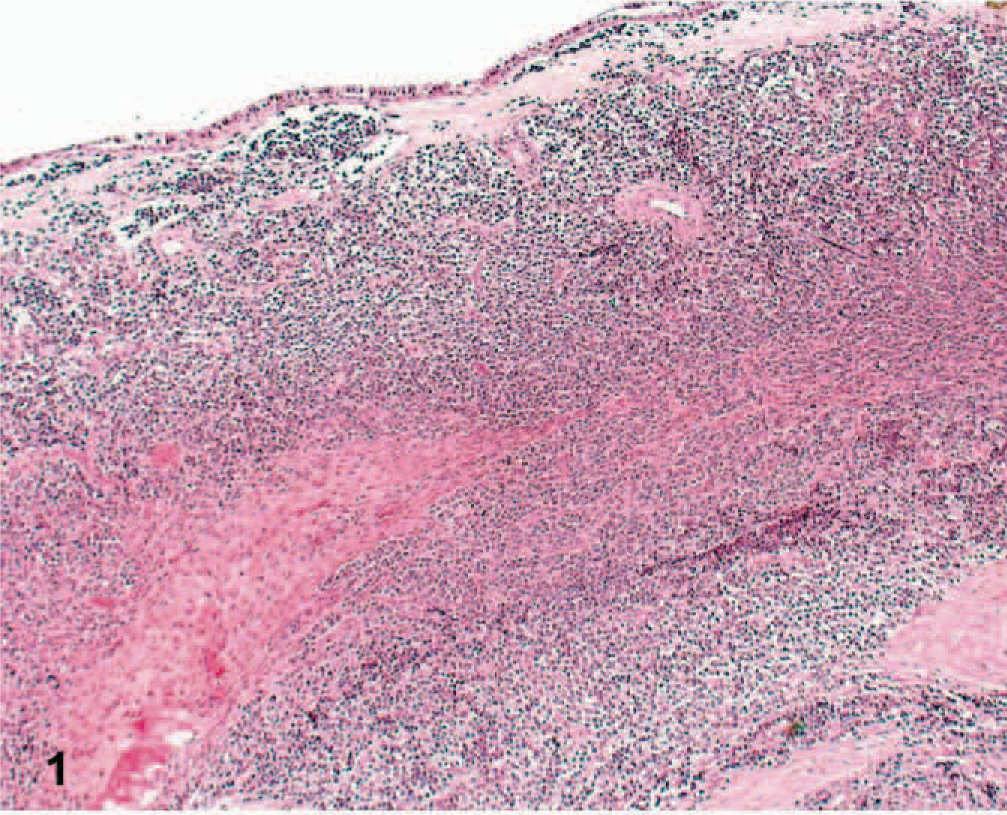
Diffuse pattern of nasal lymphoma; cat No. 7. Note the dense sheets of lymphoblasts and lack of follicle formation. HE.
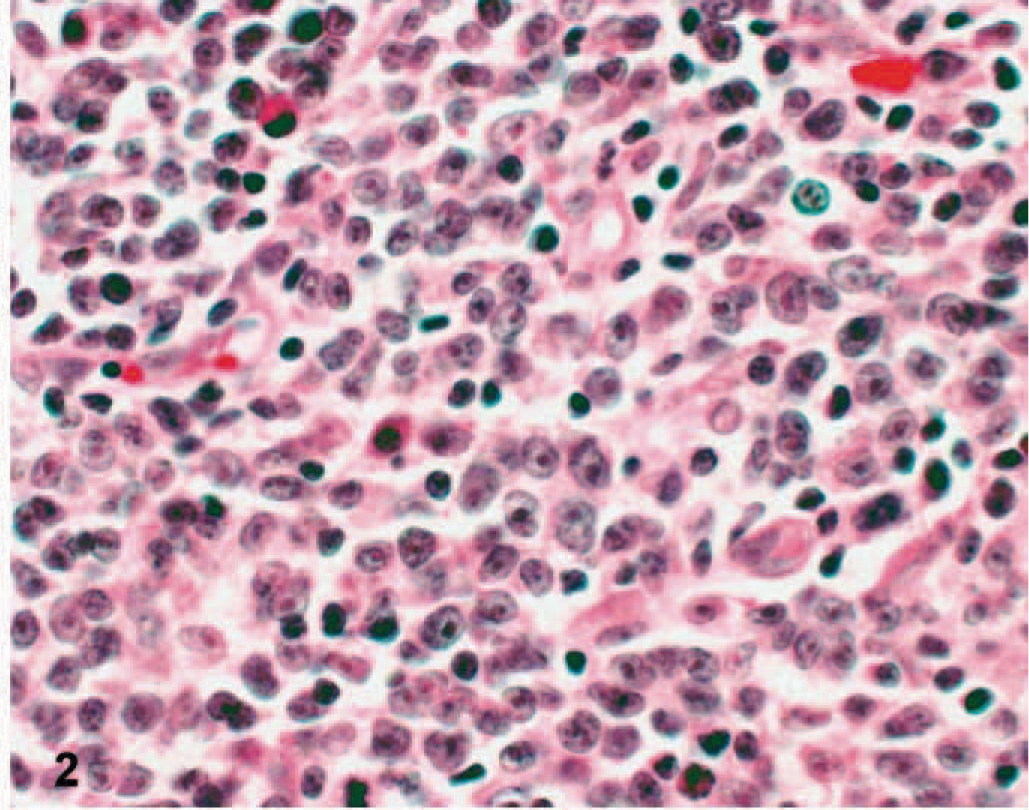
Immunoblastic lymphoma; cat No. 7. Cells contain a large round to oval nucleus and a single centrally located large round to oval nucleolus. HE.
Cat Nos. 39 and 48 were characterized as diffuse large cell lymphoma (Fig. 3). This population displayed a large round to indented nucleus, multiple peripheralized nucleoli, and scant eosinophilic cytoplasm. These 2 cats had multiorgan involvement, exhibited epitheliotropism, and were of B-cell origin. Too few cases of diffuse large-cell lymphoma were diagnosed to include histologic classification in statistical analysis.
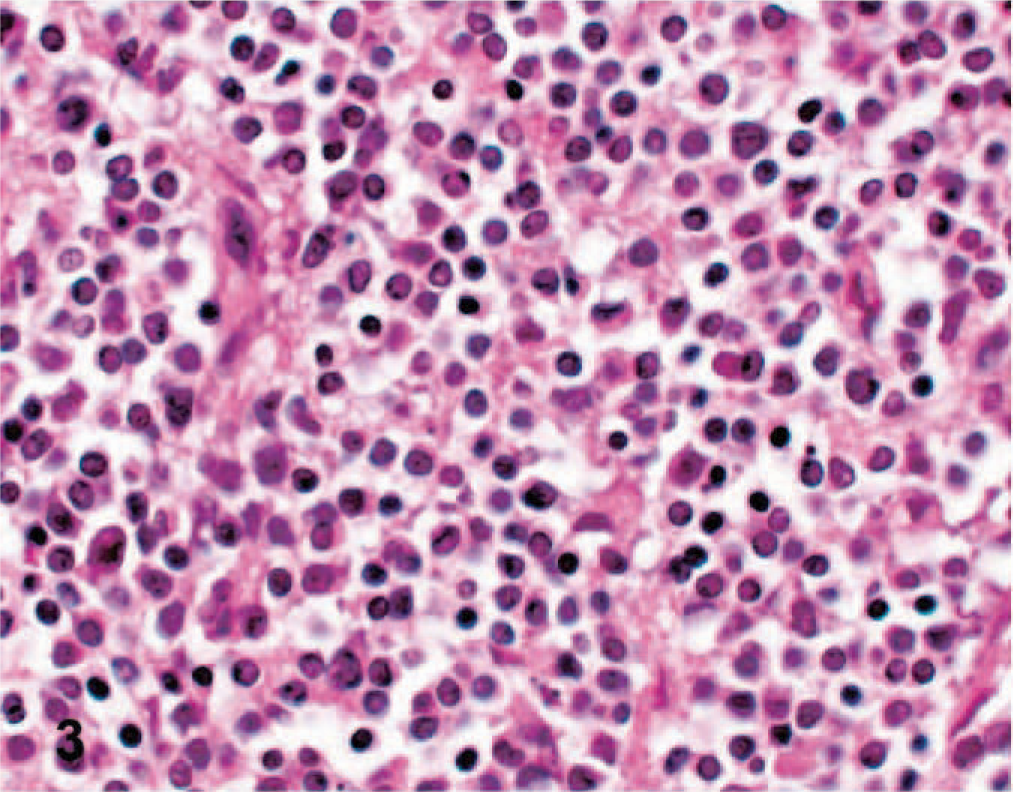
Diffuse lymphocytic lymphoma; cat No. 39. Cells display multiple peripheralized nucleoli. HE.
One cat (No. 22) that exhibited a population of mixed cell size and variably prominent nucleoli was classified as diffuse mixed lymphoma. A single cat (No. 36) displayed plasmacytic morphology and failed to fall into a specific classification category according to the NIH working formulation.
Of the 5 cats in which there was sufficient epithelium present for evaluation, 4 exhibited epitheliotropism (Nos. 3, 6, 39, and 48). Of those 4, 3 had B-cell and 1 had a granulated T-cell lymphoma; 2 had diffuse large cell and 2 immunoblastic lymphomas.
Immunohistochemical staining
Of the 45 cats for which immunohistochemical stains were available, 32 were uniformly positive for CD79a, 7 were uniformly CD3 positive, and 6 contained a mixed lymphocyte population that stained with either CD79a or CD3. No individual cells expressed both CD79a and CD3.
Cytology
Of the 21 cats evaluated cytologically, 15 were categorized as having lymphoma with the following qualifiers: certain (n = 9), probable (n = 4), and possible (n = 2). Cytopathologic features were very similar among the cats with lymphoma: a population of monomorphic intermediate to large lymphoblasts with finely granular chromatin, distinct 1-4 light blue large round to ovoid nucleoli, and scant to moderate amounts of basophilic cytoplasm (Fig. 4). In 12 cats, the lymphoblasts displayed discrete cytoplasmic vacuolization. Cytologic vacuolization was not associated with immunophenotype (P = .52) or anatomic location (P = .45). Inflammatory cells and ciliated columnar epithelial cells were frequently noted in conjunction with the neoplastic lymphoid population.
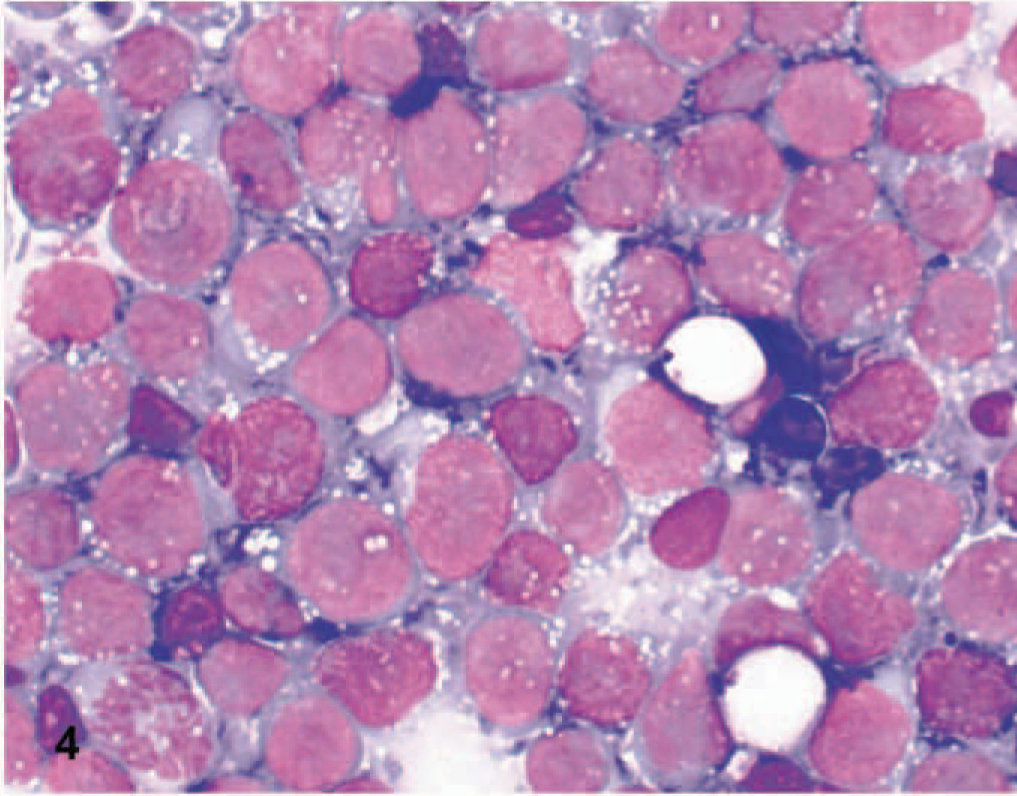
Cytology of immunoblastic lymphoma; cat No. 7. Nasal mass impression smear. Large lymphoblasts with large prominent nucleoli and vacuolated blue-grey cytoplasm. Wright-Giemsa.
Of the remaining 6 cases, 4 were classified as inflammation, 1 as heterogenous lymphoid tissue (Fig. 5), and 1 as nondiagnostic because of inadequate cellularity. Of the 4 inflammatory lesions, 3 were suppurative inflammation and 1 pyogranulomatous inflammation. One cat with lymphoma and 1 with suppurative inflammation exhibited a concurrent bacterial infection, characterized by intracellular bacterial organisms.
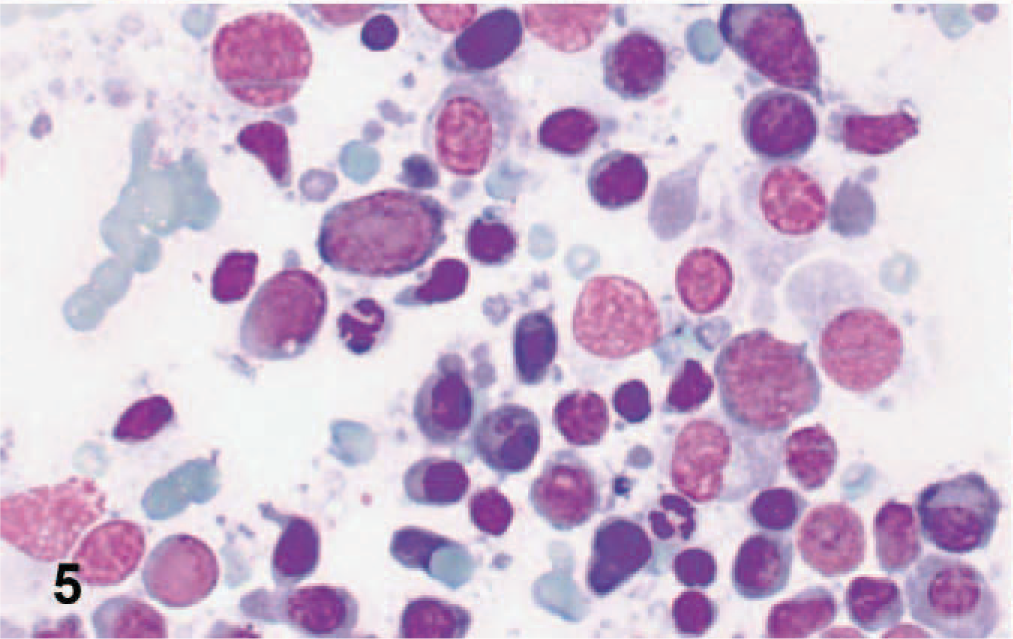
Cytology of heterogenous lymphoid and inflammatory cells; cat No. 35. Lymphoid cells include small lymphocytes, plasma cells, and large lymphoblasts. Wright-Giemsa.
Ten lymph nodes were cytologically evaluated from 9 cats, including mandibular lymph nodes (n = 9) and sternal lymph node (n = 1). All were interpreted as reactive lymphoid hyperplasia, with the exception of 1 inadequate specimen. No lymph nodes showed cytologic evidence of metastatic disease. Four bone marrow aspirates were evaluated, of which 2 showed no significant cytologic abnormalities, 1 showed erythroid hyperplasia, and 1 showed myeloid hyperplasia with mild plasmacytosis and hemosiderosis.
Discussion
This report is the largest study to date that describes the histopathologic, clinicopathologic, and immunophenotypic characteristics of feline nasal lymphoma. 6– 10, 12– 14, 19, 21, 22 In this study we document that sinonasal lymphoma in cats most frequently originates from nasal tissue; only 10% of cases are confined to nasopharyngeal tissue, and 8% involve both nasal and nasopharyngeal tissue. This study agrees with previous studies that document B-cell predominance regardless of location. 8, 19, 21 These findings are in contrast to a human study, in which 75% of nasal lymphomas and only 31% of nasopharyngeal lymphoma cases were T-cell. 17 In the aforementioned study, nasal lymphoma had a poorer response to chemotherapeutic agents and faster relapse rates than nasopharyngeal lymphoma. Future studies will investigate whether a similar relationship is present in the feline patients in the present study. Determining the tissue of origin was based on a combination of imaging modalities and histopathology, and only 3 cats lacked imaging studies. Two of these cats had necropsies that confirmed nasal lymphoma. The third cat was diagnosed with lymphoma by cytology of a mass protruding through the bridge of the nose, and was therefore classified as having nasal lymphoma. We cannot rule out that this case included both nasal and nasopharyngeal tissue.
An association between viral infection and sinonasal lymphoma immunophenotype has been made in human Asian populations. There is increased incidence of Epstein-Barre virus (EBV)–positive T-cell phenotypes in Asian countries and Peru, and EBV-negative lymphomas of B-cell origin in the United States and European countries. 1, 3 Only two cats were documented as FeLV positive, of which one was B-cell and the other was a mixed T-and B-cell population.
Mulitorgan involvement is historically rare in association with nasal lymphoma; however, in this study, 6 of 9 (67%) necropsied cats had confirmed extension beyond the nasal cavity and 4 of 13 (31%) cats with complete oncologic staging displayed potential multiorgan involvement. However, the staging postulations of multiorgan involvement were not confirmed histologically or cytologically. In addition, we cannot confirm that those cats that initially presented with multiorgan involvement originated from the nasal cavity; however, in a previous study of 118 cats with lymphoma, only 1 case of nasal lymphoma was documented in addition to any other location, including mediastinum, abdominal organs, nodal, or multicentric. 13 Direct extension of nasal lymphoma to the CNS was confirmed by necropsy in 2 cats and was suspected in 2 staged cats. To the authors' knowledge, this is the first study to document CNS extension by nasal lymphoma and the relatively common finding of multiorgan involvement.
To be consistent with previous studies of lymphoma in cats, the NIH working formulation was used to classify these neoplasms. 12, 22 Ninety percent of the cats were classified with high-grade immunoblastic lymphoma, which historically constitute 37% of all feline lymphomas. 22 Only 4 (8%) cats were classified with intermediate-grade diffuse large-cell lymphoma, which historically constitutes only 8.5% of all feline lymphoma cases. 22 In the study by Day et al. 8 study of 18 cats with nasal lymphoma, 12 were classified as diffuse large-cell type; however, this study used the Revised European-American Lyphoma/World Health Organization classification scheme. Regardless of classification scheme, this study is in agreement with the study by Day et al. 8 in that the majority of cases histologically show densely packed sheets of large lymphoblasts and a single prominent nucleolus. In contrast to the study by Day et al., 8 no cases of follicular lymphoma were documented in this study. Two cases did not conform with the NIH working formulation; 1 cat had a mixed population of T- and B-cells and 1 cat displayed plasmacytoid differentiation. We hypothesize the former was a T-cell rich B-cell lymphoma, but tissue was unavailable to confirm B-cell clonality with polymerase chain reaction (PCR). Tissue was also unavailable for special stains in the latter case, which prevents ruling out a localized extramedullary plasmacytoma.
Epitheliotropism has been documented as a feature of T-cell feline nasal lymphoma, but to the authors' knowledge, this is the first report of epitheliotropism by a B-cell nasal lymphoma in domestic species. 19 Epitheliotropism was noted in 4 cats, 3 of which were B-cell and 1 a granulated T-cell lymphoma (Fig. 6a, b). T lymphocytes can be found in epithelial tissue in health, but under certain pathological conditions, the intraepithelial migration of lymphoid cells can be greatly increased. 16 The specific position of lymphoid cells within tissues results from numerous cell-cell and cell-matrix interactions that mediate the migration of lymphoid cells from the bloodstream to the different compartments of the tissue. 16 In cats, epitheliotropism has been reported in association with T-cell lymphomas involving the skin, gastrointestinal tract, and/or nasal tissue. 19 Human studies have documented that reactive B-cells invade the tonsillar crypt epithelium in tonsillar hyperplasia and malignant B-cells migrate into the epithelium in mucosa-associated lymphoid tissue lymphomas (MALTomas). 16 These studies concluded that the adhesion pathways used in epitheliotropism are associated with the nature of the lymphoid cell (reactive or neoplastic, B or T) and/or the site of the epithelium involved. More cases are needed to determine the significance of this finding in cats.
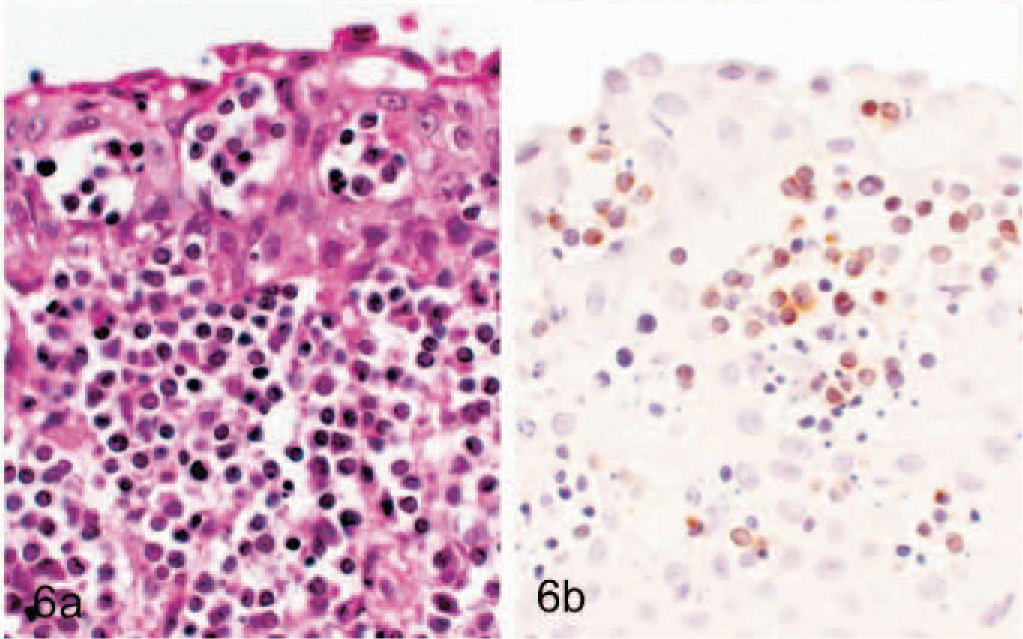
Epitheliotropism of neoplastic lymphocytes; cat No. 6. Lymphoblasts abut and migrate through the basement membrane. HE.
This is the first study to document the use of different cytologic techniques for the diagnosis of nasal lymphoma. In a previous study investigating the use of brush cytology in the diagnosis of chronic intranasal disease in cats, overall agreement between cytology and histopathology of inflammation versus neoplasia was reached in 86.8% of cats. 6 In the present study, cytology proved to be a useful adjunct to biopsy in the diagnosis of nasal lymphoma. Specificity and sensitivity of cytologic preparation techniques could not be determined because all nonlymphoma cases were excluded; however, biopsy impression smears resulted in 89% correct lymphoma diagnoses compared with 60% of fine-needle aspirations (FNAs). Although 1 of 1 nasal swab and 1 of 3 nasal flushes were diagnostic for lymphoma, conclusions cannot be drawn as to significance because of the low numbers. The 4 lymphoma that were diagnosed as inflammation on cytology were collected by nasal flush (n = 2), FNA (n = 1), and unknown method (n = 1). The significance of the vacuolization of lymphoblasts is uncertain, particularly because of the lack of vacuoles in histologic sections. It was not associated with phenotype or histologic classification, and it likely represents an artifact of fixation with Wright-Giemsa. No studies have been performed to date that document an association between vacuolated lymphoblasts and anatomic site; however, renal, gastrointestinal, and/or mediastinal lymphomas have a tendency to display this morphology. A weakness of this study is the lack of identification of false-positives, which could have a significant impact on patient survival and result in unnecessary treatment or euthanasia. Cats have a larger proportion of nasal tumors of nondescript round cell type, for which differential diagnosis is difficult, particularly among undifferentiated carcinomas, sarcoma, lymphomas, mast cell tumors, and olfactory neuroblastomas. 15 Cytology could potentially be very useful in differentiating those tumors that cannot be histologically classified without special stains. Future studies will be aimed at evaluating the use of cytology in differentiating carcinomas and lymphomas. Confirmation of lymphoma clonality with PCR could strengthen conclusions in the next phase of this study.
The mean age of cats in this study was similar to that previously reported in cats with nasal neoplasms. 8, 19 Cats with nasal neoplasia are commonly reported to have a unilateral nasal discharge; 14 however, we discovered equal numbers of affected cats displaying unilateral and bilateral nasal discharge. Panhyperproteinemia was most commonly attributable to dehydration and volume contraction. Mild to moderate hyperglobulinemia with normoalbuminemia was present in 4 cats. This abnormality was attributed to upregulation of globulin production secondary to inflammation within the neoplastic lesions. Protein electrophoresis was not performed to assess for monoclonality; therefore, neoplastic production of a monoclonal gammopathy could not be ruled out. Mild to moderate hypocholesterolemia was noted in 24% (n = 11) of cats in this study. This change has been noted in cats with hyperglobulinemia associated with multiple myeloma and in dogs with hemophagocytic histiocytic sarcoma. 18, 20 None of the cats in the present study with hypocholesterolemia had hyperglobulinemia or evidence of histiocytic sarcoma. In addition, no cats had evidence of hyperthyroidism, hepatic functional insufficiency, or protein-losing enteropathy. Most notably, 30 of 50 cats were reported to have decreased appetite, which could contribute to decreased cholesterol secondary to malnutrition. In humans with hematologic neoplasms, including lymphoma, leukemias, polycythemia vera, and myeloma, cholesterol is significantly lower in patients with leukocytosis and acts as a negative acute-phase protein inflammation. 2, 4, 5, 11 Neutrophilia was seen in conjunction with hypocholesterolemia in 5 of 11 cats in this study. However, if hypocholesterolemia were secondary to inflammation in these cats, one would expect them to have concurrent hyperglobulinemia and hypoalbuminemia, which was absent.
In summary, nasal lymphoma is more common than nasopharyngeal lymphoma in cats. Regardless of location, B-cell tumors predominate, and the majority of lesions are histologically classified as immunoblastic. This report documents for the first time local extension into the CNS, multiorgan involvement in a noteworthy number of cases, and epitheliotropism by T-cell and B-cell populations. The significance of these findings needs to be further investigated and evaluated, including the association between location, immunophenotype, histologic classification, and treatment modalities.
Footnotes
Acknowledgements
The authors would like to thank Dr. Martin Lamb for his collection of data, Dr. Adrienne French for collecting necropsy cases, Dr. Karen Oberthaler for oncology consultation, Ms. Julie Brown and Ms. Jackie Ferracone for their technical assistance, and Fran Shofer for her assistance in statistical analysis.