
Abstract
Ciliary body adenocarcinomas are well-recognized tumors in dogs; however, invasion of the lens by the tumor has not been described in veterinary species. Evaluation of the right eye of a 10-year-old Labrador Retriever revealed a ciliary body mass spanning from the 10 o'clock to 2 o'clock position that was impinging on the lens. Histologic evaluation of the enucleated eye revealed a ciliary body adenocarcinoma with lens invasion. Where the tumor encroached on the lens, the lens capsule was absent and there was scrolling of the broken ends of the capsule. Tumor cells were juxtaposed to the lens fibers and dissecting between the lens fibers. There were no inflammatory cells within the lens associated with the breaks in the capsule or within the anterior chamber. To our knowledge this is the first report of lens invasion by a tumor in any veterinary species.
A 10-year-old neutered male Labrador Retriever was evaluated for a 12-day history of blepharospasm and hyperemia of the right eye (OD). Direct and indirect pupillary light reflexes and menace response were absent OD. Enophthalmos, blepharospasm, chemosis, conjunctival hyperemia, corneal edema, aqueous flare, and hemorrhage in the anterior chamber and vitreous were present OD. Additionally, a large, pale yellow, vascularized mass overlying the dorsal region of the ciliary body spanning from the 10 o'clock to 2 o'clock position was visible just posterior to the iris, impinging on the lens and dislocating it anteriorly and ventrally (Fig. 1). The retina could not be clearly visualized. The tear production was normal, and the intraocular pressure was elevated at 31 mm Hg using applanation tonometry. Standard subconjunctival enucleation was pursued without complications for diagnostic and therapeutic purposes.
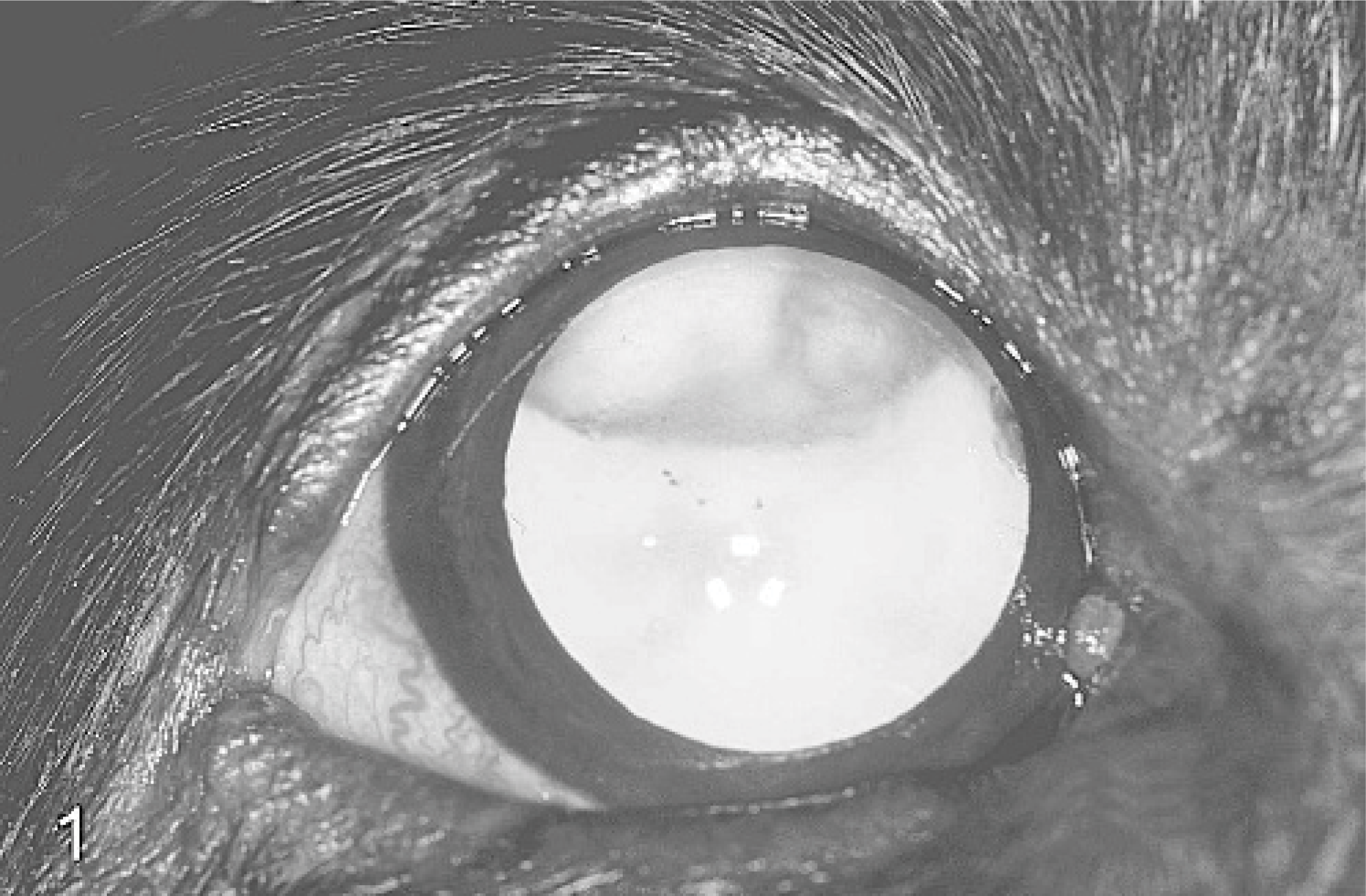
Right eye; dog. Ciliary body adenocarcinoma. A dorsally located vascularized mass extends ventrally from the region of the ciliary body to impinge on the lens. Very small amounts of hemorrhage are present in the anterior chamber and the vitreous.
The globe was fixed by immersion in Davidson's solution (95% alcohol, 10% buffered neutral formalin, distilled water, glacial acetic acid). Gross findings on the fixed specimen included a discrete, tan to pink, solid soft-tissue mass located just behind and adherent to the dorsal aspect of the posterior lens capsule and the iridociliary tissue. The globe was embedded in paraffin and sectioned at 5 μm for routine histologic examination. Sections were stained with HE. Microscopically, a large mass was identified posterior to the lens and confluent with the ciliary body. The mass was composed of numerous palisading rows of monomorphic cells aligned along a basement membrane (Fig 2). The cells had pleomorphic oval to oblong nuclei with prominent nucleoli and abundant apical eosinophilic cytoplasm. Occasionally, the cells formed pseudorosettes around endothelium-lined dilated lumina, which often contained red blood cells. Mitoses were rare. There was no scleral invasion. The mass infiltrated the lens along the majority of its posterior and temporal equatorial surfaces. At the anterior most aspect of tumor invasion into the lens, neoplastic cells were identified external to the lens, between the laminae of the capsule, and associated with a full-thickness capsular tear.
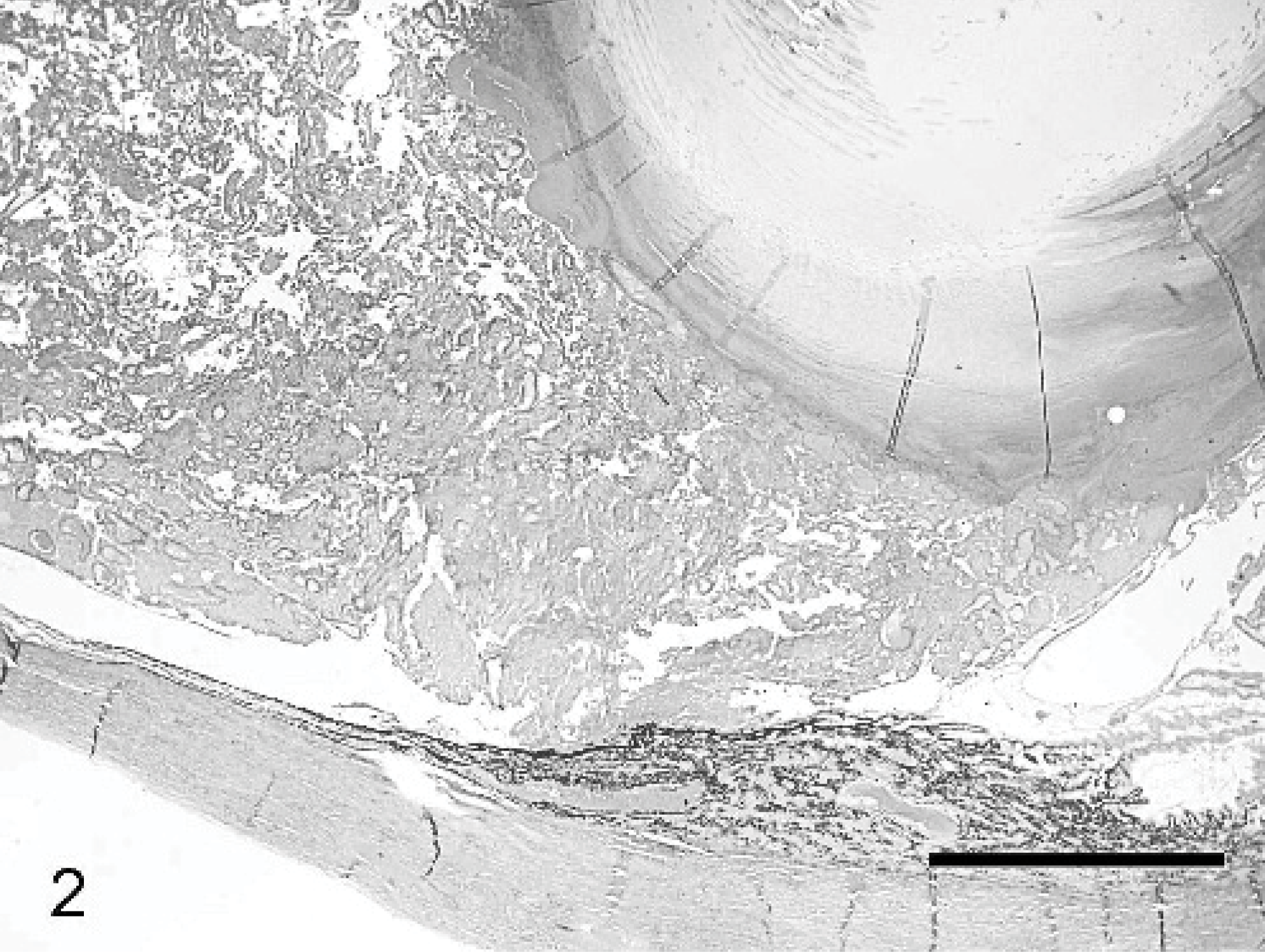
Globe; dog. Ciliary body adenocarcinoma. A large mass confluent with the ciliary body is infiltrating the posterior and equatorial lens capsule and lens. HE. Bar = 2 mm.
The capsular rupture was identified by a characteristic scrolling of the capsule (Fig. 3). Fractured lens fibers were present with tumor cells dissecting between the lens fibers (Fig. 4). There were no inflammatory cells within the lens associated with the breaks in the capsule or free within the anterior chamber. Although bladder cells and Morgagnian globules were present, they were few in number considering the concurrent pathologic processes. There were several areas of coagulative necrosis surrounded by numerous neutrophils within the vitreal aspect of the neoplastic mass. The diagnosis was a ciliary body adenocarcinoma with lens invasion.
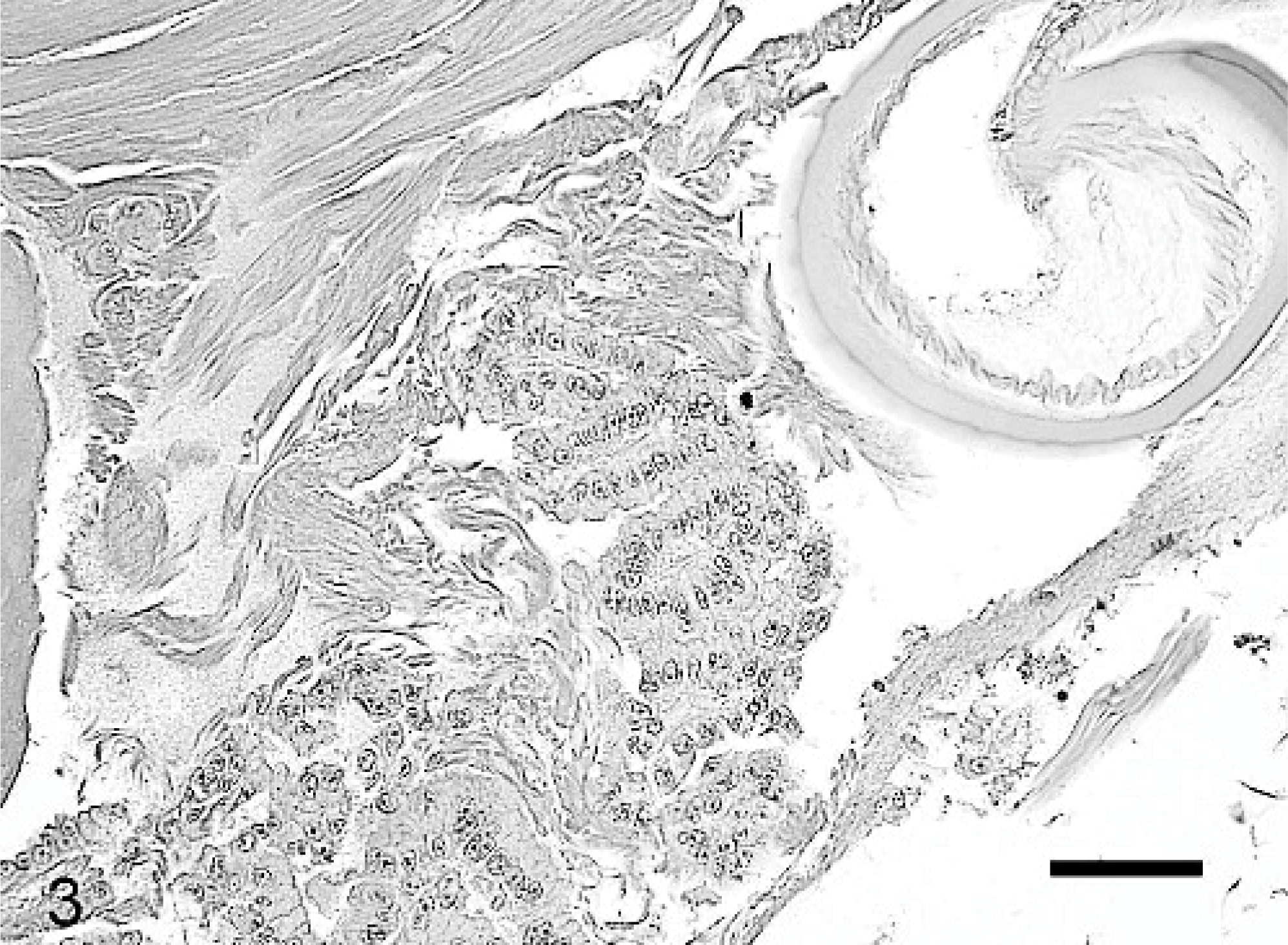
Globe; dog. Ciliary body adenocarcinoma with lens rupture. The neoplastic cells are adjacent to and internal to a ruptured scrolled lens capsule. Tumor cells are juxtaposed to the lens fibers. HE. Bar = 50 μm.
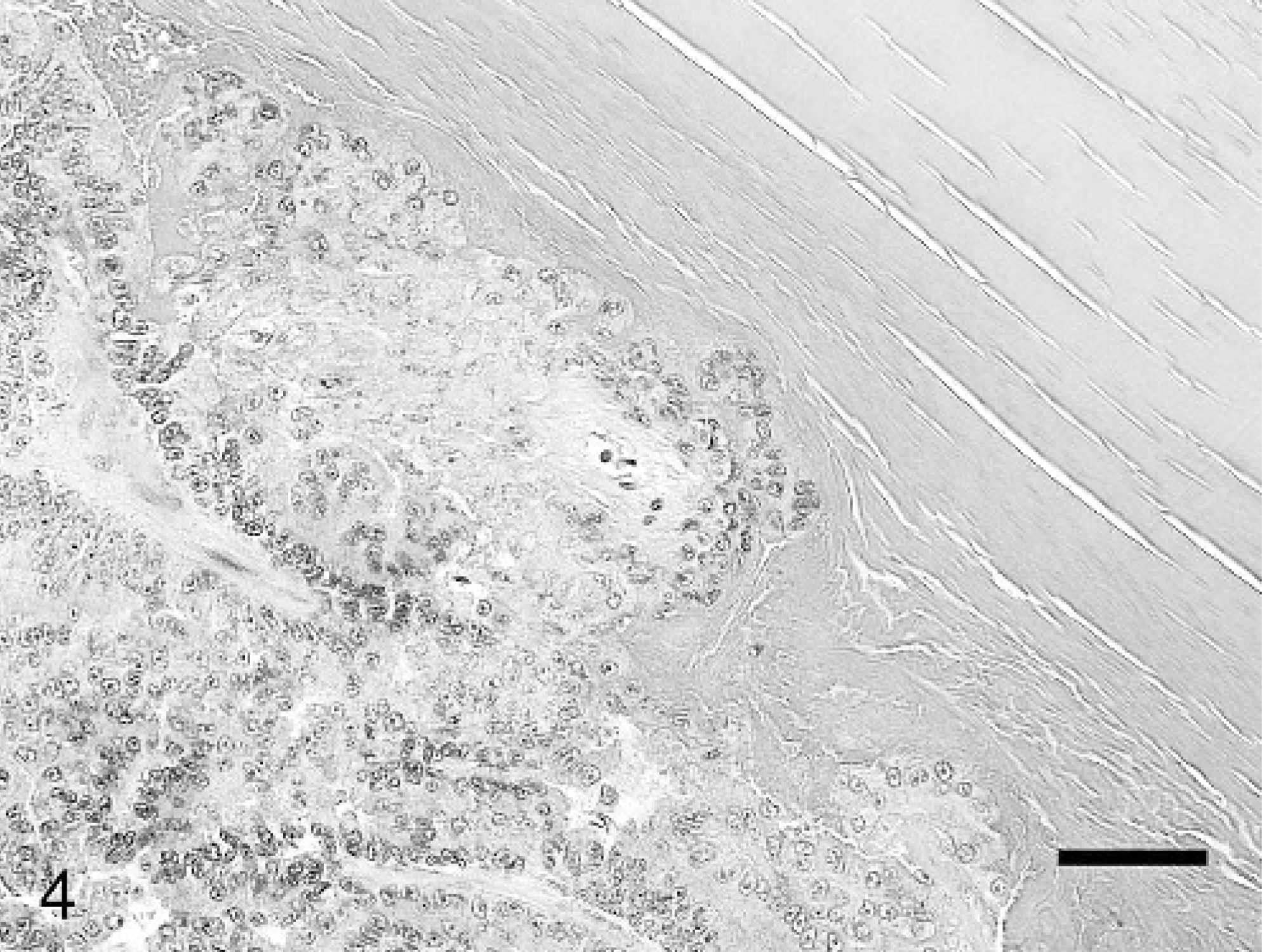
Globe; dog. Ciliary body adenocarcinoma. The large mass is composed of numerous palisading rows of monomorphic cells aligned along a basement membrane. Fractured lens fibers are present, and the tumor cells are dissecting between the lens fibers. HE. Bar = 50 μm.
Additional histologic findings in the eye included: 1) separation of the corneal lamellae, suggestive of corneal edema; 2) a preiridal fibrovascular membrane, traversing the iridocorneal angle and spanning the anterior border of the iris causing ectropion uvea; 3) a partial nonrhegmatogenous retinal detachment located dorsally just posterior to the tumor and ventrally in the nontapetal fundus with associated subretinal proteinaceous fluid, photoreceptor outer segment degeneration. and hypertrophy of the retinal pigmented epithelium “tomb-stoning”; and 5) decreased numbers of retinal ganglion cells in the ganglion cell layer. The combination of the large size of the tumor, the partial retinal detachment, and the ganglion cell loss secondary to the elevated intraocular pressure, in combination, were thought to have caused the blindness.
Iridociliary epithelial tumors are relatively common intraocular tumors in dogs and occur only second in incidence to melanoma. 5 There have been many case reports and 2 large retrospective studies 5, 14 describing this condition in dogs. Most commonly the tumors are primary, but they may also metastasize to the eye from distant locations. Iridociliary epithelial adenomas and adenocarcinomas can be pigmented or nonpigmented, solid or papillary, and invasive or noninvasive. 5, 14
It has been suggested that invasiveness of canine iridociliary epithelial tumors can be defined based on local invasion through the sclera. 5, 14 Metastatic spread is considered rare, although Dubielzig has suggested the presence of a malignant variant. 5, 6, 14 Invasion of intraocular tumors through the lens capsule and into the lens is exceedingly rare in all species. Only 3 human cases of malignant tumors of the ciliary body (a melanosarcoma, a malignant epithelioma, and a pleomorphic ciliary body adenocarcinoma) that invaded the lens have been described. 8, 10, 12 The rarity of lenticular invasion by intraocular tumors suggests an inherent resistance of the lens capsule to rupture based on its physical characteristics. The lens capsule is the thickest basement membrane of the body. 17 The lens capsule is elastic and easily moldable. 17 It is composed of collagen, laminin, entactin, and heparan sulfate proteoglycans. 2 It is generally thought to be impermeable to bacteria, inflammatory cells, and other particulate matter. 7 Because of its thickness and other characteristics, breaches of the lens capsule rarely occur. The lens capsule most commonly ruptures after accidental or surgical trauma or severe inflammatory processes. 1, 7, 11, 16
In addition to the inherent qualities of the lens capsule, tumor invasion of the lens capsule may be uncommon due to biologic behavior characteristics of the tumors. The vast majority of ciliary body tumors appear to be noninvasive and fail to metastasize. These tendencies may be related to the inability to degrade basement membranes. Multiple in-vitro studies have used bovine lens capsule as a substrate for tumor cells for evaluating the malignancy and invasiveness of some tumor types. 3, 4, 15 Generally, for tumors to invade surrounding tissues, the cells must be able to attach to the extracellular matrix, degrade the matrix, and then migrate into the altered matrix. 13 Specifically, some cathepsins, including cathepsins B, H, and L and tumor cathepsin-B−like protease, have the ability to digest the lens capsule in vitro. 9 Additionally, matrix metalloproteinases appear to play a role in cancer invasion. 13 The tumors described previously and in this report may be producing an increased amount of proteases or have an imbalance in the proteases and natural protease inhibitors.
The case described herein lacks the previously described lesions that typically accompany rupture of the lens capsule presumed secondary to trauma. These lesions include lymphocytic-plasmacytic iridocyclitis, intralenticular neutrophils, perilenticular inflammation that varies from suppurative to lymphocytic, perilenticular fibroplasia, and scleral or corneal lesions associated with the trauma. 16 The lack of histologic findings consistent with traumatic lens rupture supports the interpretation that there was a primary invasion of the lens by the tumor in this case. There were neither signs of trauma nor historical evidence of trauma. The lack of an inflammatory response in this case, even in light of lens capsular degradation, was likely due to the close apposition of the tumor to the lens fibers, preventing exposure of the lens antigens to the uveal immune system.