
Abstract
The present case is the first description of a triple infection with canine distemper virus (CDV), canine adenovirus (CAV) type 2, and Mycoplasma cynos in a dog. The 5-month-old female Miniature Pinscher was euthanized because of dyspnea, croaking lung sounds, weight loss, and lymphopenia. Pathologic examination revealed a fibrinous necrotizing pneumonia with large amphophilic intranuclear and acidophilic intracytoplasmatic inclusion bodies in different lung cells. Immunohistochemically, CDV antigen was present in lung and many other organs. In situ hybridization for detection of CAV nucleic acid showed positive signals in the lung only. Polymerase chain reaction of lung tissue and consecutive sequencing of the amplification product identified CAV type 2. Bacteriologic examination of lung tissue yielded large amounts of M cynos. This infection was confirmed by immunohistochemistry detecting abundant positive signals in the lung tissue.
Keywords
Common infectious causes of pulmonary disease in dogs are canine distemper virus (CDV) and canine adenovirus (CAV) type 2. CDV is a member of the family Paramyxoviridae, genus Morbillivirus. After aerosol exposure, primary replication occurs in macrophages of the tonsils and bronchial lymph nodes. If protective antibody levels are not reached, the infection persists in lymphoid tissues; spreads to the epithelia of the alimentary, respiratory, and urogenital tract and the skin and endocrine glands; and may reach the brain. 10 The virus can target the lungs either directly as a viral pneumonia or by its immunosuppressive effects, rendering the lungs susceptible to secondary bacterial infection. 17 CAV-2 belongs to the genus Mastadenovirus of the family Adenoviridae and is involved in the kennel cough complex or infectious laryngotracheitis. Pulmonary lesions are bronchointerstitial pneumonia with necroses and large basophilic intranuclear viral inclusion bodies in bronchiolar and alveolar epithelial cells. 17 Simultaneous infections with CAV-2 and CDV have been described. 7, 17
Mycoplasmas are wall-less bacteria that colonize the mucous membranes of the respiratory and genital tracts as well as red blood cells and are found in many animal species and in humans. 6 In dogs, mycoplasmas are considered to be part of the normal bacterial flora in the upper respiratory tract. 21 Mycoplasma canis, Mycoplasma cynos, Mycoplasma edwardii, Mycoplasma maculosum, and Mycoplasma spumans have been isolated from the nasal cavity of healthy and diseased dogs. 5 However, M cynos is the only species of mycoplasma that has commonly been associated with respiratory disease. 6, 20, 21, 27 Untyped mycoplasmal species have also been recovered from dogs with pneumonia. 14 There are, however, conflicting reports on the presence of mycoplasmas in the lower respiratory tract of healthy dogs. 19, 21 It is also assumed that mycoplasmas colonize the lungs during pneumonia 21 or due to the immunosuppressive effects of CDV or other viral agents. 17, 20 However, Rosendal 20 described an experimental M cynos infection in 1-week-old dogs that induced bronchitis, peribronchitis, and inflammation of the adjacent lung tissue, reminiscent of lesions in rats with Mycoplasma pulmonis infection. Naturally occurring primary M cynos pneumonia has been described recently. 27
Here we report, for the first time, a case of pneumonia caused by a concurrent triple infection with CDV, CAV-2, and M cynos in a puppy. Pathologic findings and further diagnostic investigations including immunohistochemistry, in situ hybridization (ISH), transmission electron microscopy (TEM), polymerase chain reaction (PCR), and sequence analysis are reported.
A 5-month-old, female Miniature Pinscher puppy was bought in a pet store in Nice (France) and brought into Austria. The vaccination document showed that the puppy had been vaccinated against canine parvovirus, CDV, and CAV-2 infections, as well as leptospirosis, twice within a range of 2 weeks. Exact dates and manufacturer of the vaccine were not available. The dog developed signs of catarrhal oculonasal discharge and coughing 1 week after purchase. Following a 1-week treatment (with the antibiotic tetracyclin twice a day, eye ointment including tetramycin/dexamethasone, and a mucolytic therapy with ambroxol) by a local veterinarian, the dog showed no improvement, and weight loss was noticed additionally. The dog was then referred to the University of Veterinary Medicine, Vienna, with mucopurulent oculonasal discharge, severe moist cough, retching, and signs of pulmonary disease. The puppy was dehydrated and afebrile. The blood count showed lymphopenia (741 lymphocytes/μl, reference range for adult dogs 780–4,500/μl), elevated band neutrophils (1,945/μl, reference value <500/μl), segmented neutrophils (5,556/μl, reference value 3,300–11,250/μl), and monocytosis (1,019/μl, reference value <500/μl). The therapy started with antibiotics (amoxicillin/clavulanic acid), an oral mucolytic agent (bromhexine hydrochloride), infusions (lactated Ringer's solution), and administration of oxygen.
An x-ray radiograph revealed signs of pneumonia and pleurisy. Conjunctival swabs tested positive for CDV by PCR. Ultrasound examination showed an enlargement of the right heart.
The puppy's condition continued to deteriorate to pumping breathing with croaking lung sounds, the body temperature rose to 40°C, and even small excitements provoked severe dyspnea accompanied by mouth breathing. The antibiotic therapy was extended with azithromycin; however, because of the severe clinical signs, the dog was euthanized.
Complete necropsy was performed. Pharyngeal and tracheal swabs as well as lung samples were taken for bacteriologic examination. The nutritional status was mild emaciation, and there was moderate anemia. The entire lungs were compact, dark red, and edematous, with slight serous effusion in the pleural cavity. Both heart ventricles were moderately dilated. Besides a severe congestion of the liver and kidneys, no macroscopic abnormalities were found in other organs.
Histologically, the lung parenchyma showed a severe diffuse acute fibrinous pneumonia with an accompanying exudation of neutrophils and macrophages into the alveoli and hyperplasia and exfoliation of type II pneumocytes. Additional findings were severe hyperemia with multifocal extensive hemorrhage and multifocal coalescing necrotic areas (Fig. 1) with degenerate neutrophils and cell debris in their center. Severe necrotizing bronchiolitis was also present. Many large amphophilic, intranuclear inclusion bodies were found predominantly in hypertrophic alveolar epithelial cells (Fig. 2), in cells within the alveolar lumina, and in the bronchial epithelial cells. In addition, there were a few acidophilic intracytoplasmic inclusion bodies in the epithelial cells of the bronchial glands (Fig. 3) and in the alveolar epithelial cells. Intracytoplasmic inclusion bodies were also found in the epithelial cells of the stomach. The white pulp of the spleen showed central depletion of lymphocytes. Other tissues, including the brain, were apparently normal.
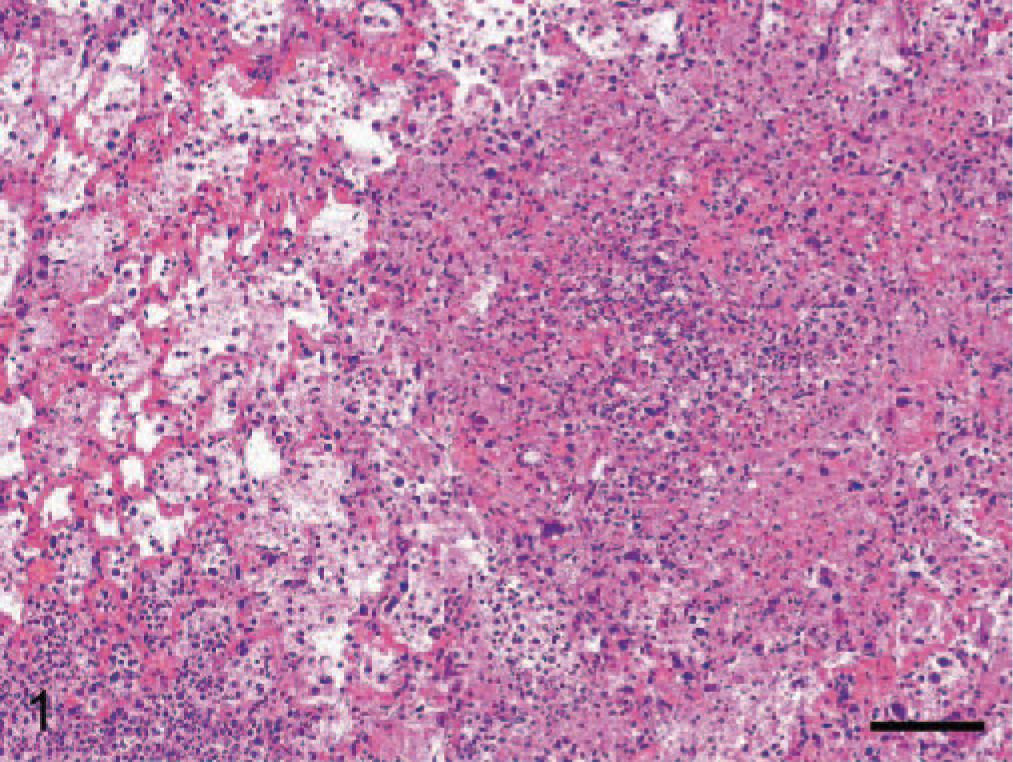
Lung; dog. Fibrinonecrotic pneumonia with hemorrhages is seen. HE. Bar = 98 μm.
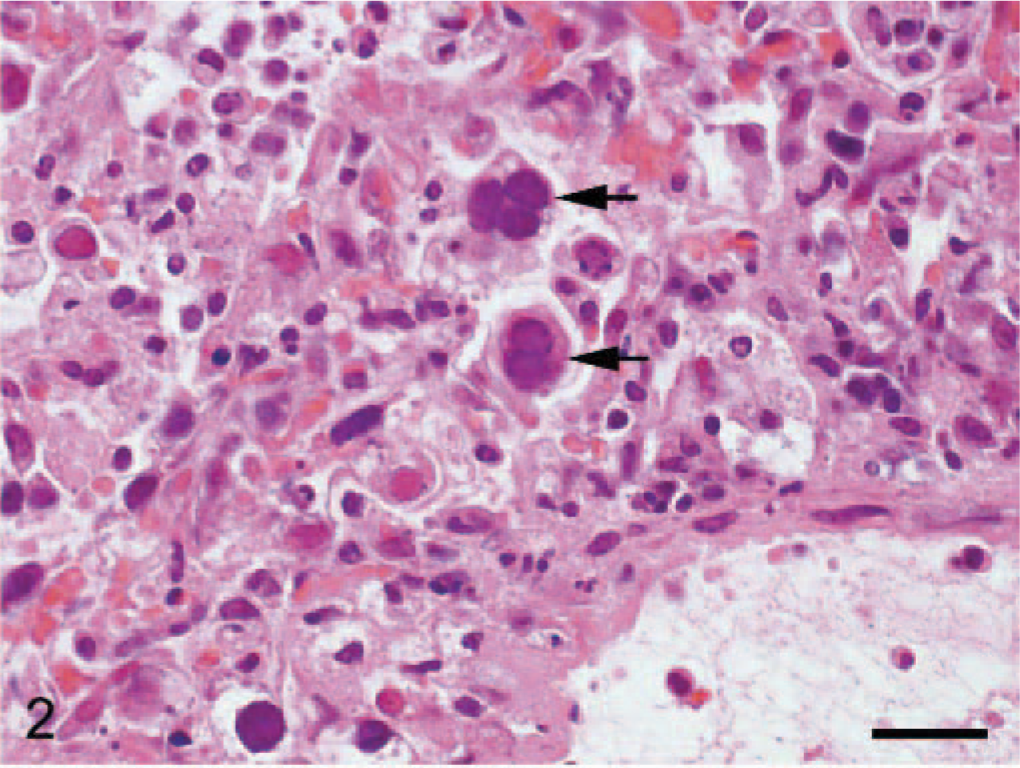
Lung; dog. Large basophilic intranuclear viral inclusions are seen in alveolar epithelial cells (arrows). HE. Bar = 25 μm.
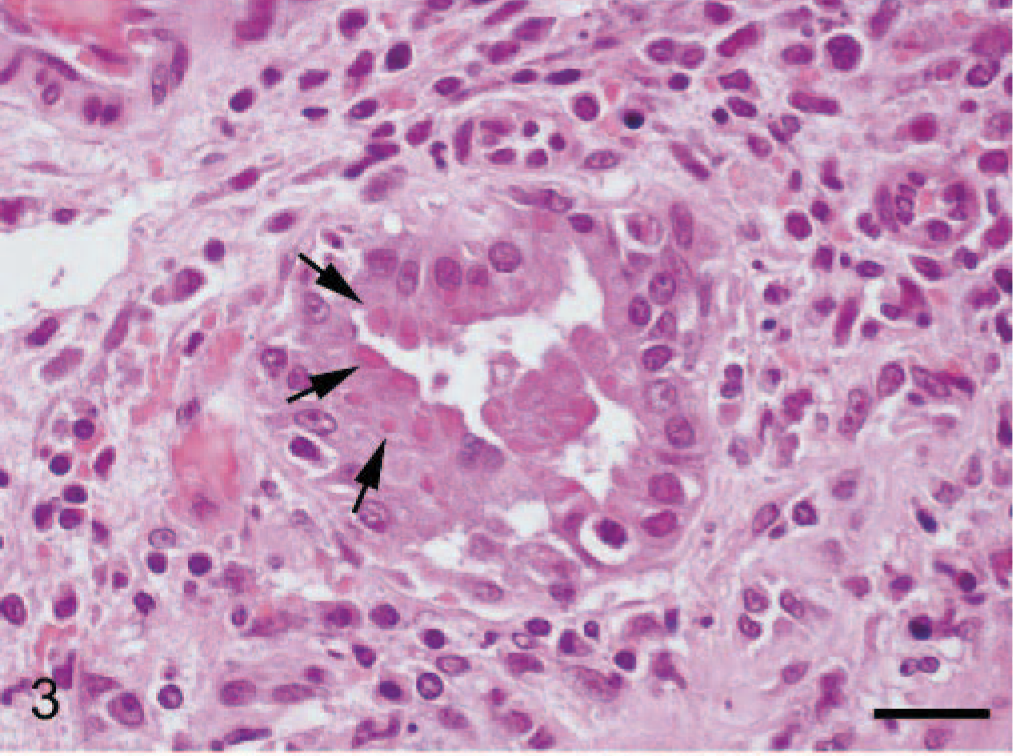
Lung; dog. Acidophilic inclusion bodies are seen in bronchial gland epithelial cells (arrows). HE. Bar = 25 μm.
Immunohistochemically, CDV protein was demonstrated by a standard avidin-biotin-complex method as described previously. 23 The lung showed abundant positive signals in the epithelial cells of the peribronchial glands, alveolar epithelial cells, and intra-alveolar cells (Fig. 4), which frequently also contained large amphophilic intranuclear inclusions. The white matter of the cerebrum and cerebellum showed large numbers of positive astrocytes (confirmed by immunohistochemistry for an astrocyte-specific marker, glial fibrillary acidic protein on consecutive serial sections); in the cerebellum, positive signals were found additionally in cells with microglia morphology. There was also strong immunopositivity in epithelial cells of the stomach, cells of the white and red pulp of the spleen, Kupffer cells of the liver, as well as in fibroblasts and fibrocytes of kidney and heart.
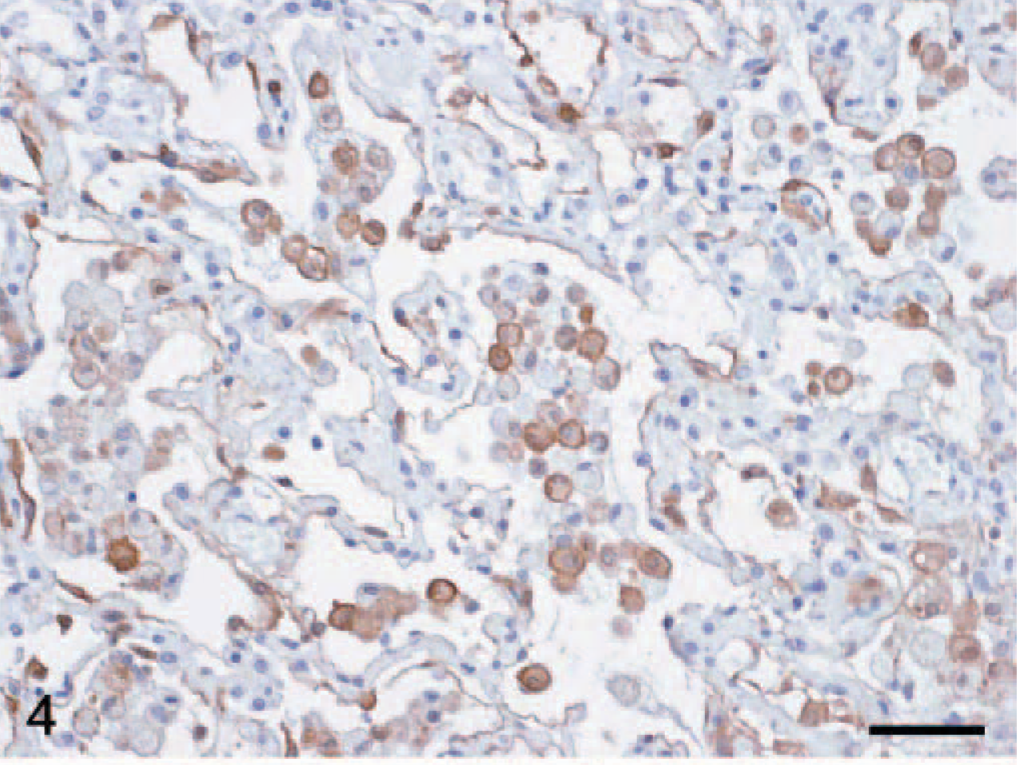
Lung; dog. Canine distemper virus antigen is seen in the alveolar epithelial cells and intra-alveolar cells. Immunohistochemistry. Bar = 49 μm.
For immunohistochemical detection of M cynos antigen in lung tissue, the avidin-biotin-complex technique using a polyclonal hyperimmune serum against M cynos was applied. Large amounts of M cynos were detected multifocally within the necrotic areas as punctate signals within the cytoplasm of alveolar macrophages but also extracellularly (Fig. 5).
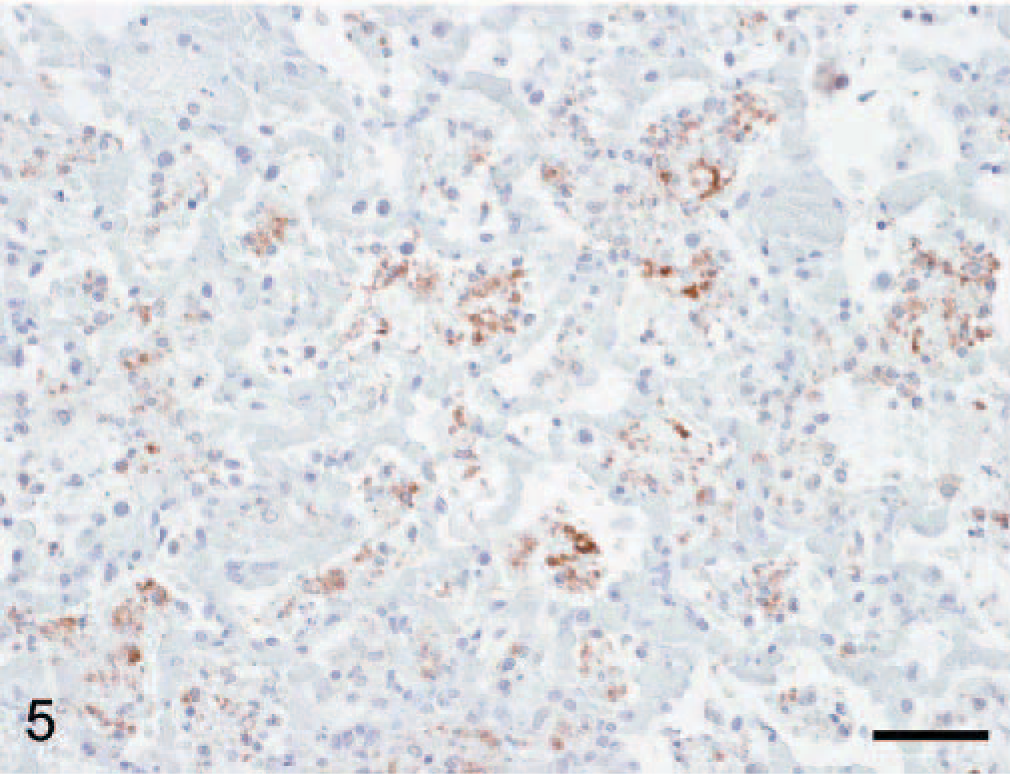
Lung; dog. Focal Mycoplasma cynos immunoreactivity is discernible as punctate signals within lung tissue. Immunohistochemistry. Bar = 49 μm.
An ISH for detection of CAV nucleic acid was performed according to Benetka et al. 2006. 4 Intranuclear signal was found in the lung, especially in alveolar (Fig. 6) and bronchial epithelial cells, but no signal was present in the epithelial cells of the bronchial glands. The signal clearly corresponded with the observed presence of large intranuclear inclusion bodies. No signal was found in other organs such as the liver, spleen, kidney, and brain.
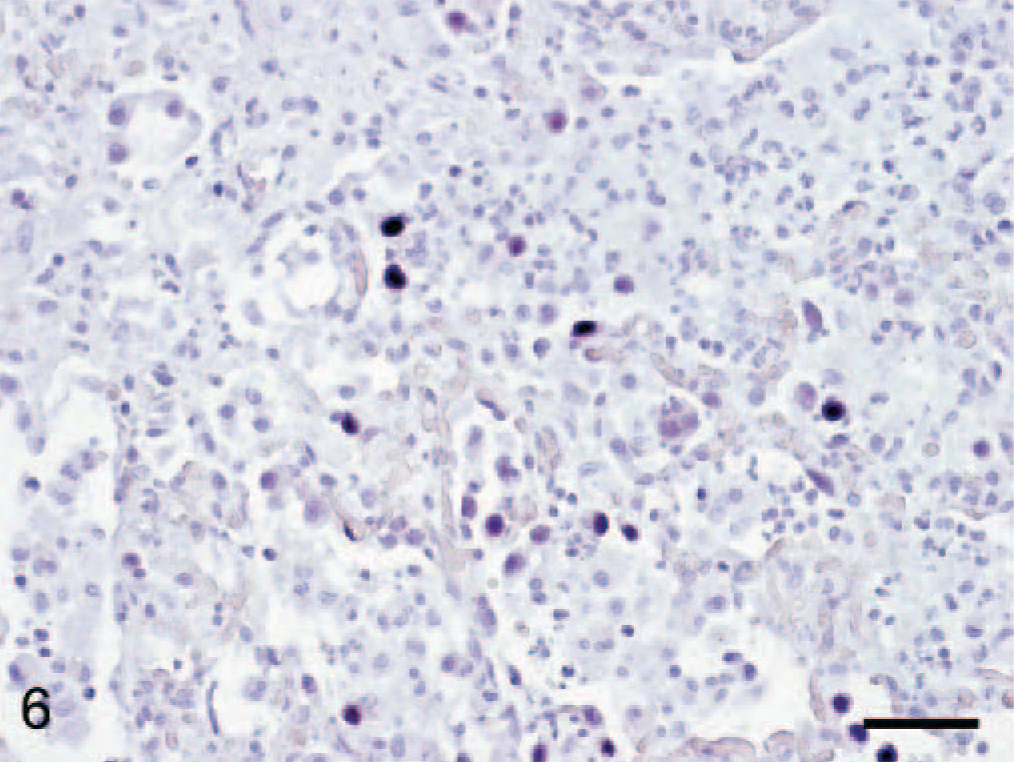
Lung; dog. Canine adenovirus nucleic acid is detected in the nuclei of alveolar epithelial cells. In situ hybridization. Bar = 49 μm.
Small cubes of the lung fixed in 7% buffered formalin were used for TEM. They were washed in phosphate-buffered saline, pH 7.2, for 24 hours, postfixed in glutaraldehyde and osmium tetroxide, and embedded in Glycid ether 100 (Serva, Heidelberg, Germany) according to standard techniques. Ultrathin sections were stained with uranyl acetate and lead citrate and examined in a transmission electron microscope. Adenovirus particles, predominantly in paracristalline arrays, were abundant in many nuclei of lung cells, the majority of which showed morphologic features of type 2 pneumocytes (Fig. 7). Paramyxoviral or mycoplasmal structures were not unequivocally identified.
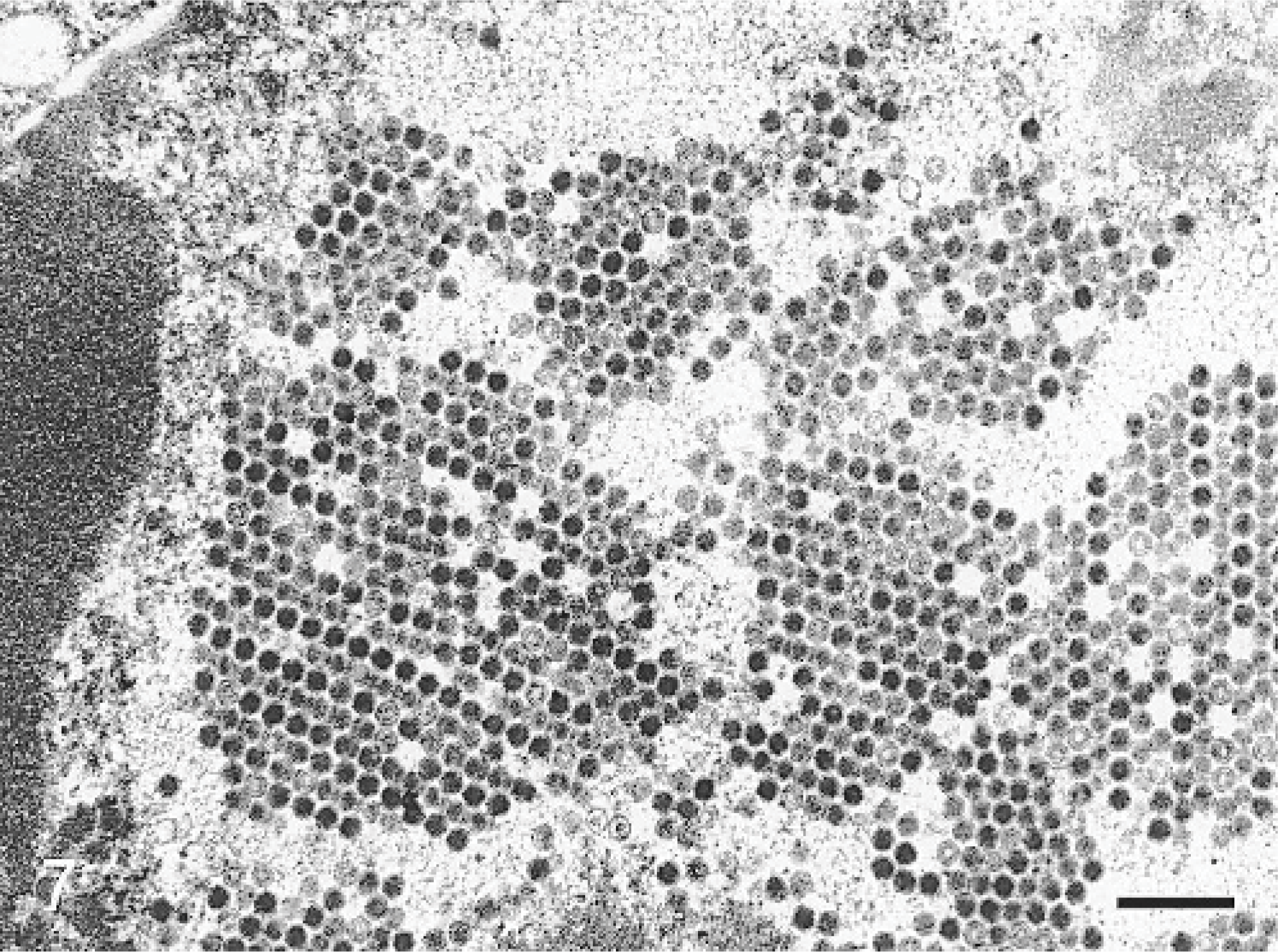
Lung; dog. Crystalline arrays of adenovirus particles are seen in the nucleus of a lung cell. Transmission electron micrograph. Bar = 0.4 μm.
Lung samples and tracheal and pharyngeal swabs were cultured using conventional methods for isolation and differentiation of aerobic and anaerobic bacteria as well as fungi. Identification was done on all isolates using standard identification methods. In addition, samples were plated on modified Hayflick agar for propagation of mycoplasmas, and colonies were identified using the colony immunoblot technique. 24
M cynos was abundantly recovered from the lung, besides little amounts of β-hemolytic Streptococci and Klebsiella sp.; M cynos was also isolated from pharyngeal and tracheal swabs, accompanied by little amounts of Proteus sp. and Escherichia coli.
Lung tissue was also analyzed by PCR for the detection of CAV, canine herpes virus (CHV), and CDV-specific nucleic acids as described previously. 4, 12 The sample tested positive for CDV and CAV, but negative for CHV. Consecutive sequencing of the amplification product obtained after CAV-specific PCR (564 bp) revealed 100% homology with the CAV-2 reference strain Toronto A26/61 (GenBank acc. no. U77082, position 8024–8587) and only 89% homology with 2 CAV-1 reference strains (CAV-1 complete genome, acc. no. Y07760 and CAV-1 acc. no. U55001). Thus, the virus was clearly identified as CAV-2. The amplification product obtained after CDV-specific PCR (266 bp) was 98% identical to German and Swiss CDV isolates (acc. nos. AJ009656, pos. 674–939, AF164967, pos. 781–1046). For this part of the genome, no sequences of isolates from France or Austria are available in the GenBank.
In this article, we describe a case of concurrent infection with CDV, CAV-2, and M cynos. Despite the development of effective vaccines, CDV remains endemic in most parts of the world. 8, 11, 18 Furthermore, it has frequently been isolated in pet shops or in dog shelters where kennel cough had been diagnosed. 8 Key features of CDV infection are depletion of B and T cells, 26 interstitial pneumonia, and the presence of both intracytoplasmic and intranuclear eosinophilic inclusions in the epithelial cells of many tissues. 17 Nervous system involvement is common, and the extent of neuropathologic alterations depends on the age and the immune status of the animal at the time of infection. 16, 25 In the present dog, CDV had induced a generalized infection with large amounts of virus in the lung, lymphatic tissues, and central nervous system. The observed lymphopenia and lymphoid depletion indicated severe immunosuppression. The lung lesions, however, were at least partially due to direct viral effects because there was strong viral replication in lung tissue. The virus had also reached the brain, but demyelination or other neuropathologic lesions had not yet developed. The abundant replication or growth of the 2 other pathogens was most likely due to the immunosuppressive effects of CDV. 9 On the basis of molecular analyses, canine adenoviruses can be grouped into 2 distinct but related virus species, CAV-1 (infectious canine hepatitis virus) and CAV-2. 3, 13 A spontaneous dual infection with CDV and CAV-1 has been reported, with bronchointerstitial pneumonia and hepatocellular necroses as the most prominent findings. 15 Concurrent infections of CAV-2 with CDV have also been observed. 7– 9
On the basis of the abundant distribution of CAV-nucleic acid and associated inclusion bodies, this virus also significantly contributed to the severity of pneumonia, predominantly of the bronchial and the pneumocyte-2 lesions. The presence of typical intranuclear inclusion bodies was suspicious for adenovirus infection, which could be confirmed by ISH, PCR, and electron microscopy. There were no lesions or intranuclear inclusion bodies in the liver, excluding a CAV-1 infection. Sequencing of the amplification product also clearly proved CAV-2 as the involved agent.
Infections of the respiratory tract with mycoplasmas in dogs are still controversial, and there is little information on specific infections caused by Mycoplasma sp. In addition to the scarce reports on pneumonias associated with mycoplasmas in dogs, 2, 6, 22, 27 the present case adds to the assumption that M cynos can be involved in canine pulmonary disease. The bacteria seem to have been responsible for a strong necrotizing component of the pneumonia, as they were predominantly localized in such areas. This potential of M cynos has already been observed previously. 27 The importance and distribution of M cynos, the mechanisms of pathogenicity, and the nature of the immune response to this pathogen are currently unknown because the study of canine mycoplasmas has for a long time been neglected due to the difficulties in isolation associated with mixed infections and the difficulty of identification at the species level.
Finally, it should be mentioned that the puppy had been vaccinated against CDV and CAV infections. However, due to the lack of a detailed vaccination history, no interpretation of the efficacy of this vaccination is possible.
Footnotes
Acknowledgements
We thank Karin Fragner, Nora Neodorost, Christine Schneider, Christine Glatzer, and Rosa Romstorfer for excellent technical assistance and Klaus Bittermann for the professional digital artwork.