
Abstract
Dozens of red, raised nodules scattered along the serosal surface of the small intestine and the right and left ovaries were observed as incidental findings on gross examination in a 21-year-old Thoroughbred mare euthanatized for severe lameness. Histologically, these nodules were composed of numerous, variably sized, redundant vascular profiles filled with red blood cells and fibrin thrombi. Based on the presence of multiple nodules composed of benign vascular channels scattered within the small intestine and ovary, a diagnosis of angiomatosis is proposed. To the authors' knowledge, this is the first report of small intestinal and ovarian angiomatosis in a horse.
Angiomatosis is a malformative disorder characterized by benign nodules composed of numerous abnormal blood vessels that are scattered throughout various organ systems.3 In humans, these lesions can be congenital or a reactive, tumor-like vascular proliferation after birth, termed bacillary angiomatosis.3 There is a lack of consensus within the veterinary literature over the classification of nodules composed of vascular channels, with similar histologic lesions reported as either single neoplasms (angiomas, hemangiomas) or as disseminated benign vascular malformations (angiomatosis, hemangiomatosis).
In horses, angiomatosis has been rarely described. In one report, angiomatosis was documented in the skin of 9 horses and in the large intestine of a single horse.6 A focal, benign malformative vascular lesion, termed hemangiomatosis, has also been reported in the meninges of a horse.4 In addition, there are 2 separate reports of benign spinal cord vascular lesions in individual horses. In one horse, it was reported as a single angioma, while in the second it was reported as a focal vascular malformation.1,5 To the authors' knowledge, this is the first report of angiomatosis in the small intestine and ovary in a horse.
A 21-year-old intact female Thoroughbred presented to the referring veterinarian with a 7-month history of severe hind limb lameness and swelling, which was unresponsive to treatment. Due to the poor prognosis, the horse was humanely euthanatized and submitted for necropsy at Cornell University.
On postmortem examination, there was severe, locally extensive suppurative fasciitis, tenosynovitis, arthritis, and osteitis within the left fetlock, which likely caused the clinical signs noted before euthanasia. In addition, there were few incidental findings. Scattered along the serosal surface of the small intestine were dozens of red, slightly raised, 0.5- to 1-cm-diameter, red, gelatinous nodules that extended into the tunica muscularis. On the surface of the left ovary there was a focal, 2-mm-diameter, red, slightly raised nodule that extended slightly into the parenchyma. The right ovary was markedly distended by an 8.5 cm × 7 cm × 17 cm blood-filled, encapsulated cystic structure. Representative samples were taken and immersion-fixed in 10% neutral buffered formalin and routinely processed for paraffin embedding, sectioned 3- to 5-um thick, and stained with HE.
Histologically, within the small intestine, there were multiple fairly well-demarcated, unencapsulated nodules that extended from and expanded the tunica muscularis (Fig. 1). The nodules were composed of variably sized, blood-filled channels lined by a single layer of nonreactive, flattened endothelial cells surrounded by a thin tunica media and supported by a stroma composed of mature collagen (Fig. 2). Fibrin thrombi were present in the lumens of a few scattered vascular channels within the nodule.
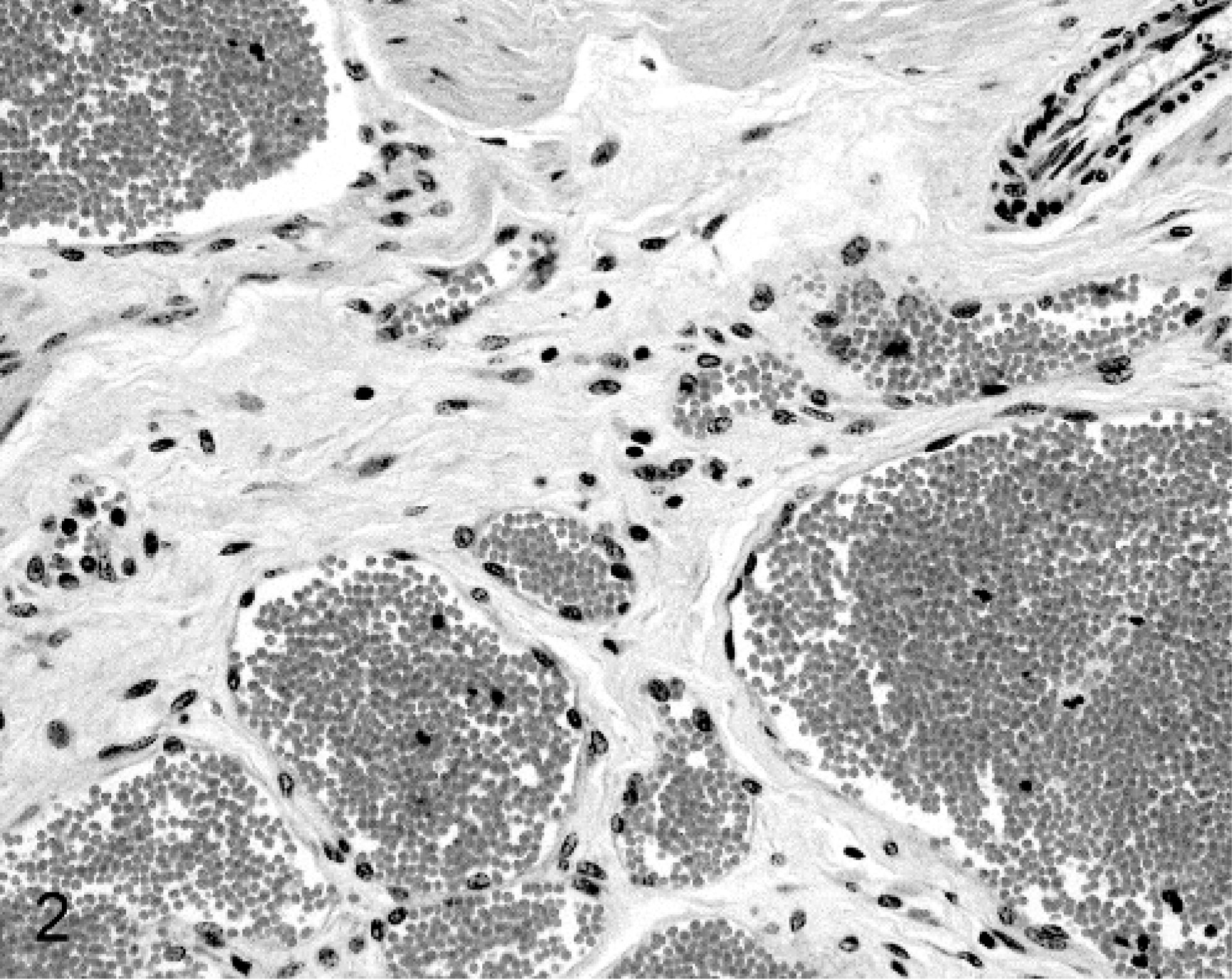
Small intestine; horse. The vascular channels are lined by bland endothelium and filled centrally with blood. HE stain.
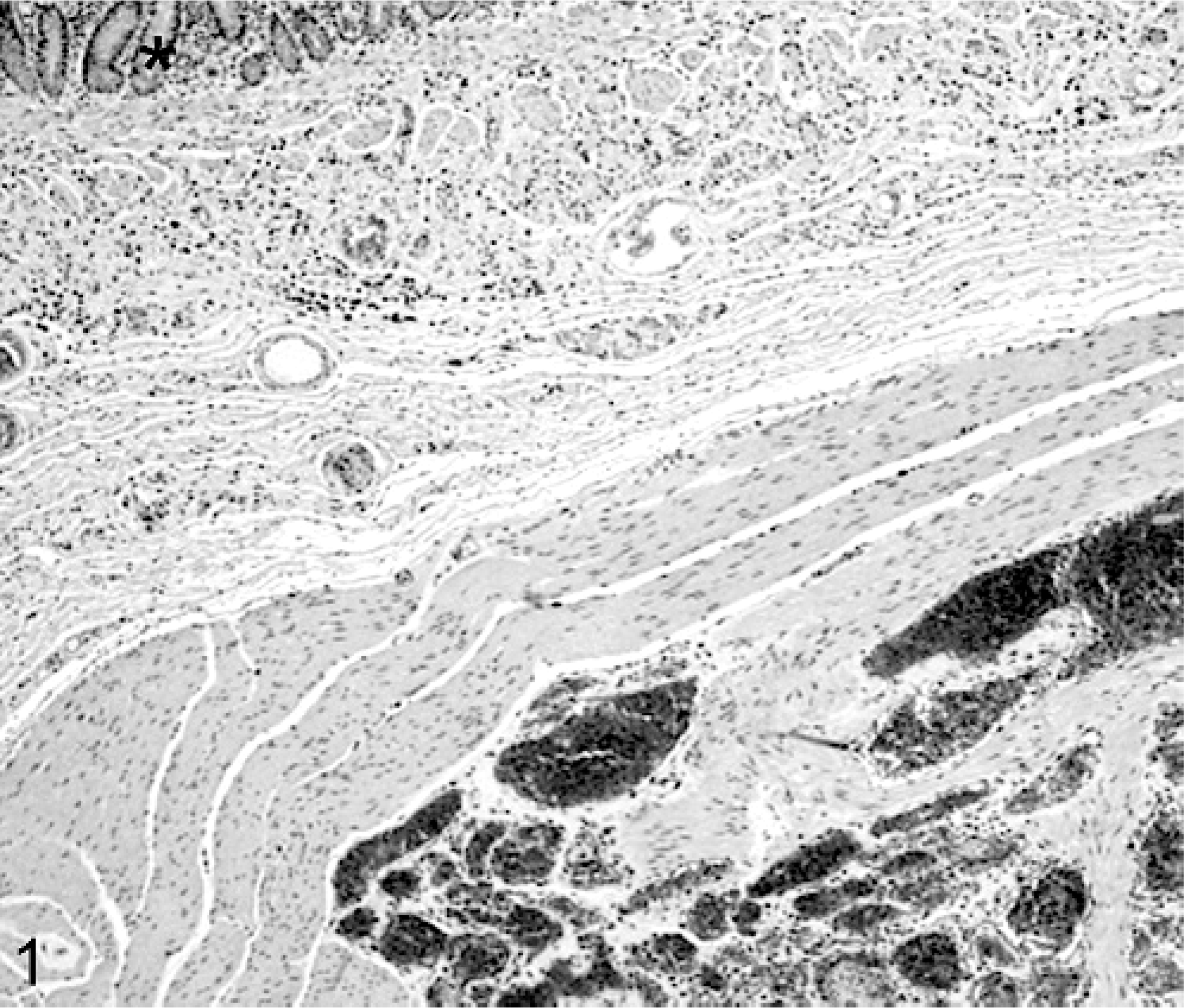
Small intestine; horse. There is a well-demarcated nodule composed of numerous redundant vascular channels within the muscularis. The asterisk marks the intestinal mucosa. HE stain.
In histologic sections of the left ovary and extending from the ovarian stroma, there was a similar, though poorly demarcated, aggregate of bland, blood-filled vascular channels similar to those in the small intestine (Fig. 3). Within the right ovary, a hemorrhagic anovulatory follicle (autumn follicle) diagnosed grossly was confirmed histologically. In addition, within this section there was a fairly well-demarcated, multilobulated, nodule that expanded the serosal connective tissue and muscle of the ovary adjacent to the anovulatory follicle. The nodule was composed of bland, blood-filled vascular channels similar to those in the small intestine and the right ovary.
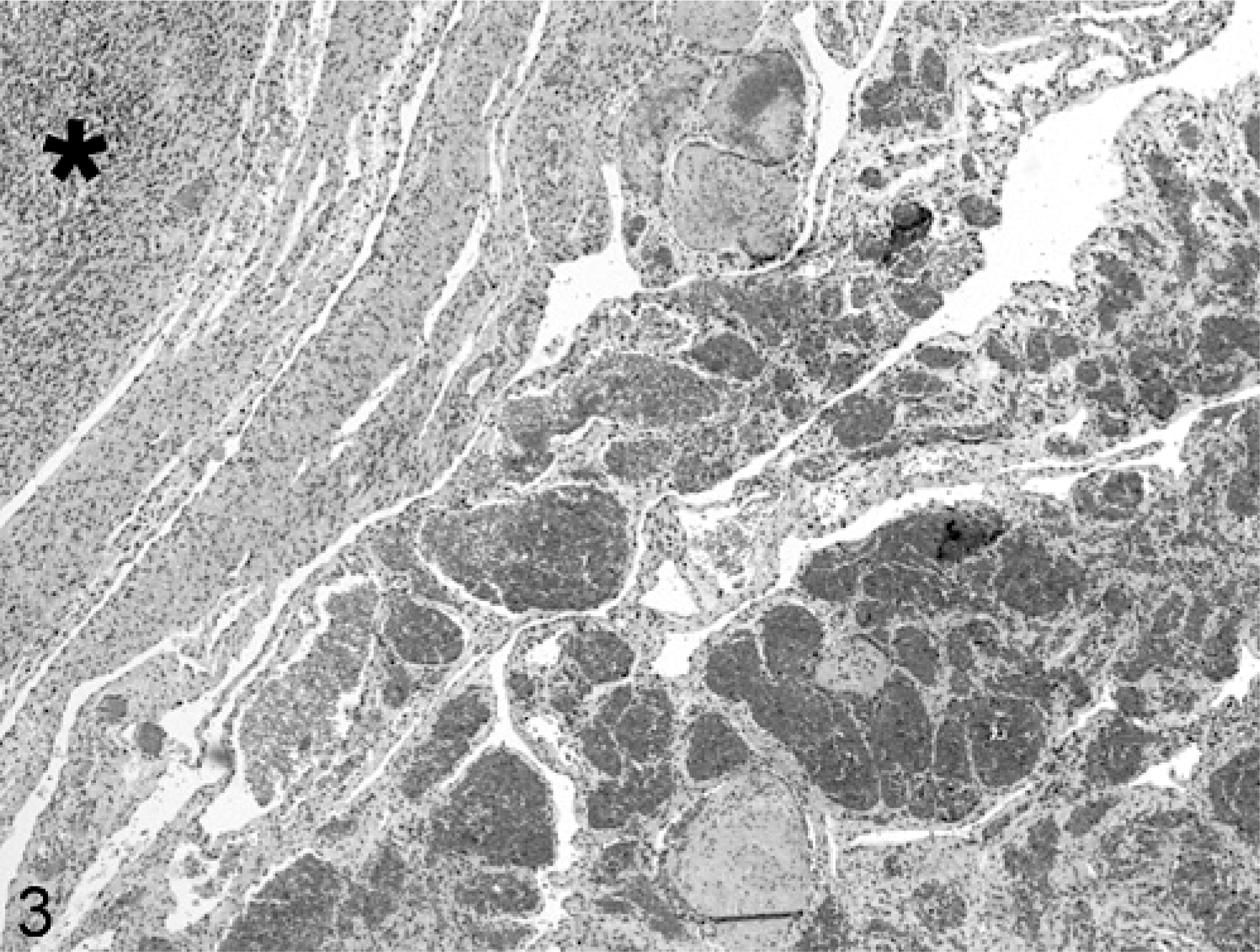
Right ovary; horse. The connective tissue and muscle surrounding the right ovary is markedly expanded by numerous, redundant vascular profiles. The normal ovarian stroma is marked with an asterisk. HE stain.
Streptavidin-biotin staining with a mouse monoclonal antibody for von Willebrand factor (Dako Corp., Carpinteria, CA) was applied to 4-um sections of the nodules within the small intestine and ovaries (Fig. 4). The cells lining the vascular channels were positive for von Willebrand factor, confirming endothelial origin. Based on the distribution of the vascular proliferations of endothelial origin, angiomatosis of the small intestine and ovaries was diagnosed.
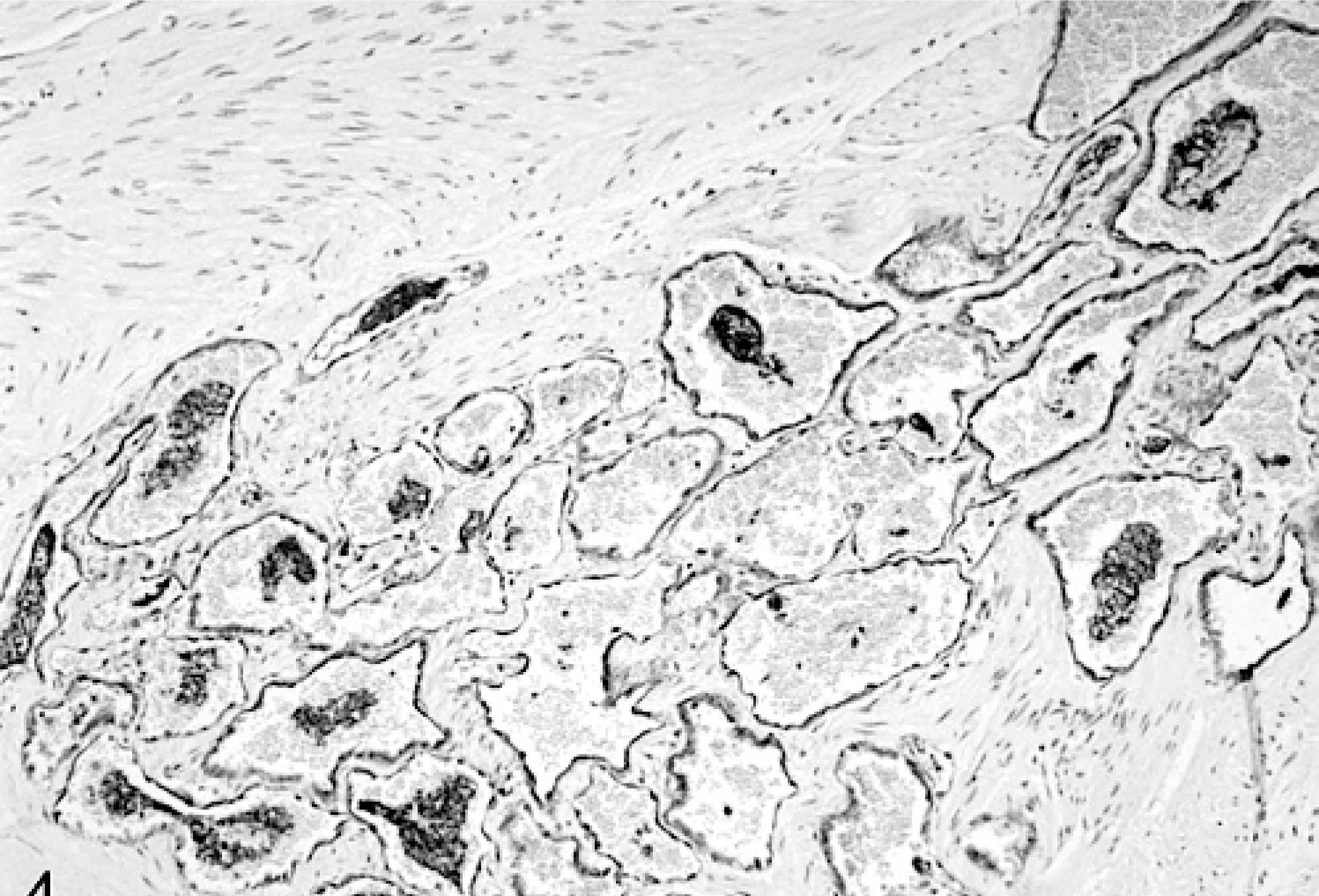
Small intestine; horse. Within the nodule, the endothelial cells lining the vascular channels are positively labeled with von Willebrand antibody. Streptavidin-biotin staining for von Willebrand.
The nodules within the small intestine grossly resembled those of hemomelasma ilei. Hemomelasma ilei grossly appear as one to multiple oval, red, raised plaques along the antimesenteric serosal surface of the distal small intestine, particularly the ileum. Unlike hemomelasma ilei, the angiomatous lesions in this horse were distributed throughout the entire small intestine and were relatively small and round. Histologically, hemomelasma ilei is characterized by subserosal hemorrhage, a mononuclear inflammatory infiltrate, and varying amounts of blood breakdown pigments. When red, raised lesions within the intestine are seen on gross examination, angiomatosis should exist as a differential in addition to hemomelasma ilei. Angiomatosis has been reported previously as an incidental finding in the colon, which did not interfere with function.6 This is the first report of angiomatosis in the small intestine. The nodules did not appear to interfere with intestinal function in this horse as there was no indication of colic or obstruction within the history.
The presence of malformative vascular lesions within the ovaries was also quite unusual. Vascular tumors and malformations are rarely reported in horses. A single study of ovarian lesions in Egyptian donkeys reported focal ovarian cavernous hemangiomas in 6% of cases.8 There is also a single report of a focal congenital ovarian vascular hamartoma in a horse.7 This is the first report of angiomatosis within the ovaries of a horse represented by numerous nodules composed of redundant vascular profiles. There is no indication within the history provided that the angiomatosis interfered with reproductive function.
We believe angiomatosis represents a malformative process, which may be focal or multifocal and may involve multiple organ systems. In this horse, the lesions did not appear to interfere with function based on the clinical history. Furthermore, the primary problem in this horse was lameness, and there were no lesions of angiomatosis within the limbs that could have contributed to this or the swelling and edema noted on gross examination. If the angiomatosis lesions remain small and do not involve critical sites such as the central nervous system, it is likely that they will not cause clinical disease in an affected horse and will remain undiagnosed until a complete necropsy is performed.
Footnotes
Acknowledgements
We would like to thank Dr. Brielle Rosa for submitting this case for necropsy. We would also like to thank Dr. Donald Schlafer and Dr. Brian Summers for consulting on this case.