
Abstract
Equine dysautonomia, or grass sickness, is a frequently fatal disease of unknown etiology, manifested as poor gastrointestinal motility and colic as a result of degenerative changes in the autonomic nervous system. Examination of ileal biopsies collected at laparotomy is currently the best antemortem diagnostic method to distinguish equine dysautonomia from colic cases, which can present with similar signs, but their value has not been previously critically evaluated. Using simulated biopsies collected postmortem from 23 cases of equine dysautonomia and 11 of colic, the sensitivity and specificity of 1-cm long, formalin-fixed ileal biopsies was 100% for the diagnosis of equine dysautonomia. There was therefore no advantage to using larger biopsies or examining jejunum either in addition to or instead of ileal biopsies. Furthermore, although cryostat sections of ileum, 1-cm long, had a sensitivity of 100%, the specificity was only 73%, meaning that 27% of cases would have been misclassified, resulting in unnecessary euthanasia. Increasing the size of the cryostat or examining jejunum in addition to ileum cryostat sections did not significantly improve the specificity. Results of the current study indicate that in diagnostic practice, 1-cm long, formalin-fixed biopsies are likely to be the most suitable for accurate diagnosis, despite the slower turnaround time compared with cryostat sections.
Equine dysautonomia (ED), or grass sickness, is a frequently fatal disease that was first recognized in Scotland in 1909 and currently occurs in the United Kingdom, mainland Europe, 1 and the southern part of South America. 9 Equine dysautonomia has been identified in at least 1 indigenous horse in the United States (Philip Johnson, personal communication, 2009). The incidence is highest in the United Kingdom, where it is an important cause of equine morbidity and mortality. Equine dysautonomia occurs in 3 overlapping forms (acute, subacute, and chronic), and although the first 2 forms are fatal, more than 40% of chronic cases may recover with appropriate management. 2 The major clinical signs relate to dysfunction of the alimentary tract and include pharyngeal and esophageal dysphagia, colic, reduced gastrointestinal motility, and nasogastric reflux. The etiology is unknown, but recent research has focused on the hypothesis that ED is a toxicoinfection with Clostridium botulinum type C that is acquired from soil while grazing. 4,5 Equine dysautonomia is characterized by neuronal degeneration resembling chromatolysis and a reduction in the number of neurons in the prevertebral and paravertebral autonomic ganglia and the enteric plexuses. 3,6 Neuronal damage in the gastrointestinal tract is not uniform, and although the ileum is usually the most severely affected, 8 the jejunum can be more severely affected than the ileum in a minority of cases. 3
Histopathologic examination of the autonomic ganglia postmortem is considered the gold standard method for diagnosis. Antemortem diagnosis is problematic, because the clinical signs are similar to those of other causes of acute colic, and the most reliable method currently available is histopathologic examination of the enteric plexuses in ileal biopsy samples obtained at laparotomy, 7 which is invasive, time-consuming, and expensive. Although in many cases a definitive diagnosis can be made based on a single ileal biopsy, in a significant number of cases, the diagnosis is uncertain or incorrect in ED-affected horses. This is a particular problem when small, frozen (cryostat) sections rather than formalin-fixed sections are examined to minimize reporting time, because cryostats are often of inferior quality compared with fixed sections. In addition, there is debate among clinicians and pathologists regarding the minimum size of biopsy required for a definitive diagnosis. There is therefore a clear need for an accurate, rapid antemortem diagnosis, because false positives may result in unnecessary euthanasia, the usual course of action after a diagnosis of acute or subacute ED, and false negatives prolong suffering of cases that have a very poor prognosis. The aims of the current study were to critically assess the diagnostic value of ileal and jejunal biopsies in the antemortem diagnosis of ED by 1) comparing formalin-fixed with cryostat sections, 2) determining whether examination of jejunum in addition to ileum is of diagnostic value, and 3) assessing the size of biopsy required for accurate diagnosis by using simulated biopsies collected at postmortem examination.
All clinical cases were referred to the Dick Vet Equine Hospital (Roslin, Midlothian, United Kingdom) between October 2003 and July 2008 and required euthanasia on clinical grounds. The inclusion criteria were that the case had shown clinical signs for less than 7 days and was in fresh postmortem condition. The clinical cases consisted of 23 cases of ED (11 cases of acute equine dysautonomia [duration of clinical signs: <2 days] and 12 cases of subacute equine dysautonomia [duration of signs: 2–7 days]) and 11 cases of colic of <7 days' duration. The colic group contained Thoroughbred or Thoroughbred crossbreds (6), native ponies (2), other crossbred types (2), and 1 cob, with a median age of 11 years (range: 3–21 years). There were 5 females, 5 geldings, and 1 intact male. The group consisted of cases of enteritis (4), strangulating lipoma (3), large colon displacement (2), entrapment of the jejunum in the epiploic foramen (1), and a non-ED motility disorder of unknown etiology (1). Acute and subacute colic cases were used for comparison, because they represent the cases that must be distinguished from ED cases by intestinal biopsy in clinical practice. The ED group comprised native ponies (10), cobs (7), Thoroughbred or Thoroughbred crossbreds (3), Warmblood or Warmblood crossbreds (2), and 1 other crossbred, with a median age of 7 years (range: 1–13 years). There were 8 females, 14 geldings, and 1 intact male in the group.
All horses were euthanized by IV injection of quinalbarbitone sodium (400 mg/ml) and cinchocaine HCl (25 mg/ml) a because of a poor prognosis. A full postmortem examination, with collection of routine samples for diagnostic purposes, was carried out. All except 4 study samples (2 from ED and 2 from colic cases) were collected within 2 hr of death. The other 4 samples were collected within 5 hr of death. In the ED cases, samples from the cranial cervical ganglion (or in a few cases, the coeliacomesenteric ganglion) were collected and fixed in phosphate buffered formalin (pH 7.4) for routine histologic examination to confirm the diagnosis (gold standard method), and in the colic cases, these ganglia were examined to exclude ED.
Ileal and jejunal samples, each 30 mm long in a circumferential direction and 20 mm wide in an oral-aboral direction, were collected from the antimesenteric border of the midjejunum and the terminal ileum and then divided into 2 30 mm × 10 mm sections. One section was placed in phosphate buffered formalin until trimmed for processing. The other section was snap frozen in isopentane that was precooled with dry ice and kept at −70°C until processed for cryostat sections. For each 30-mm long, fixed, and frozen jejunum and ileum sample, 3 nonconsecutive sections were made (A, B, and C; Fig. 1). All intestinal and ganglion sections were processed by routine methods and stained with hematoxylin and eosin.
The sections on glass slides were marked into 3 1-cm long parts and labeled cm 1, 2, and 3, respectively (Fig. 2). The fixed and cryostat sections were assessed by a pathologist (E. M. Milne) who was experienced in ED diagnosis and blinded to the case identity. The sections were recorded as positive or negative (i.e., ED or non-ED) by assessing each of the following independently: section A, cm 1; section A, cm 1 plus cm 2; section A, whole section; cm 2 on sections A, B plus C. The 4 methods of examination allowed assessment of 1) the optimal size of biopsy for diagnostic purposes, 2) the difference in sensitivity and specificity in using cryostat versus fixed sections, and 3) whether examination of jejunum and ileum together had any advantage over ileum alone. Biopsies were considered negative for ED when neurons in the submucosal and/or myenteric plexus appeared normal in numbers and morphology (Fig. 3) and positive for ED where there was typical degeneration of these neurons (Fig. 4) or a complete absence of neurons. 3,6 Cases were considered positive for ED by the gold standard method of histopathologic examination of ganglion sections collected postmortem (Fig. 5) as previously described.11 The sensitivity and specificity, including 95% exact binomial confidence intervals, were determined by standard methods for each size and type of biopsy, including the results for ileum alone, jejunum alone, and ileum with jejunum.
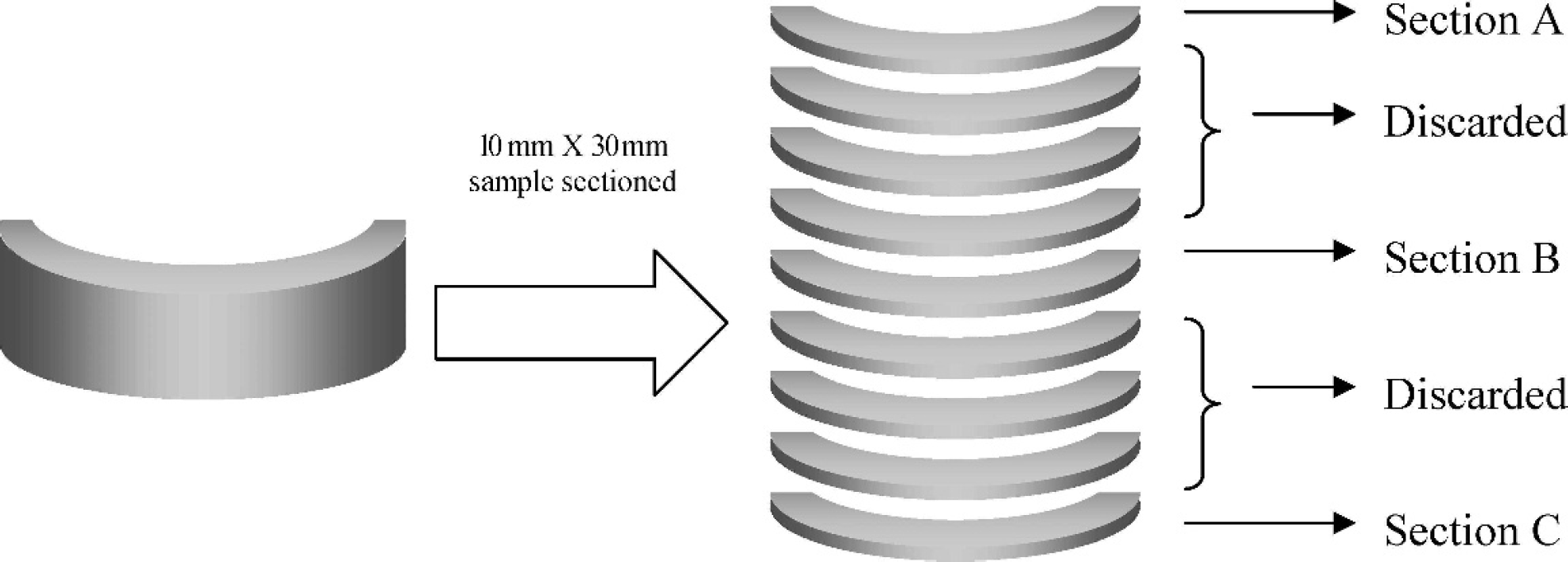
Schematic diagram of the postprocessing sectioning of partial circumferential samples of jejunum and ileum. Four- and 10-μm sections were obtained from formalin-fixed and snap-frozen samples, respectively.
Taking a 1-cm long, formalin-fixed ileal biopsy as the diagnostic tool for ED resulted in 100% sensitivity and specificity (Table 1). Therefore, there was no advantage in taking other ileal sections or combinations of sections, because no improvement was possible. In contrast, although using a 1-cm long, formalin-fixed jejunum biopsy did not result in any change in the specificity, the sensitivity dropped to 61%. Even if multiple sections or a whole 3-cm section of formalin-fixed jejunum was used, sensitivity never reached higher than 87% (all 3 sections considered).
When 1-cm long, ileal cryostat sections were used, the sensitivity remained at 100% and the specificity dropped to 73% (Table 1). Furthermore, the maximum specificity found, with any combination of ileal cryostat sections or with different ileal cryostat section lengths, was only 82% (whole 3 cm on 1 section). The sensitivity and specificity with jejunum cryostat sections were even worse with the maxima found when 3 1-cm long, nonconsecutive sections were examined (78% and 82%, respectively), with only 61% and 73%, respectively, in a 1-cm long jejunum cryostat section. Finally, combining ileal and jejunum cryostat sections did provide 100% sensitivity regardless of the size of the section; however, specificity never reached higher than 91% (whole 3 cm on 1 section).
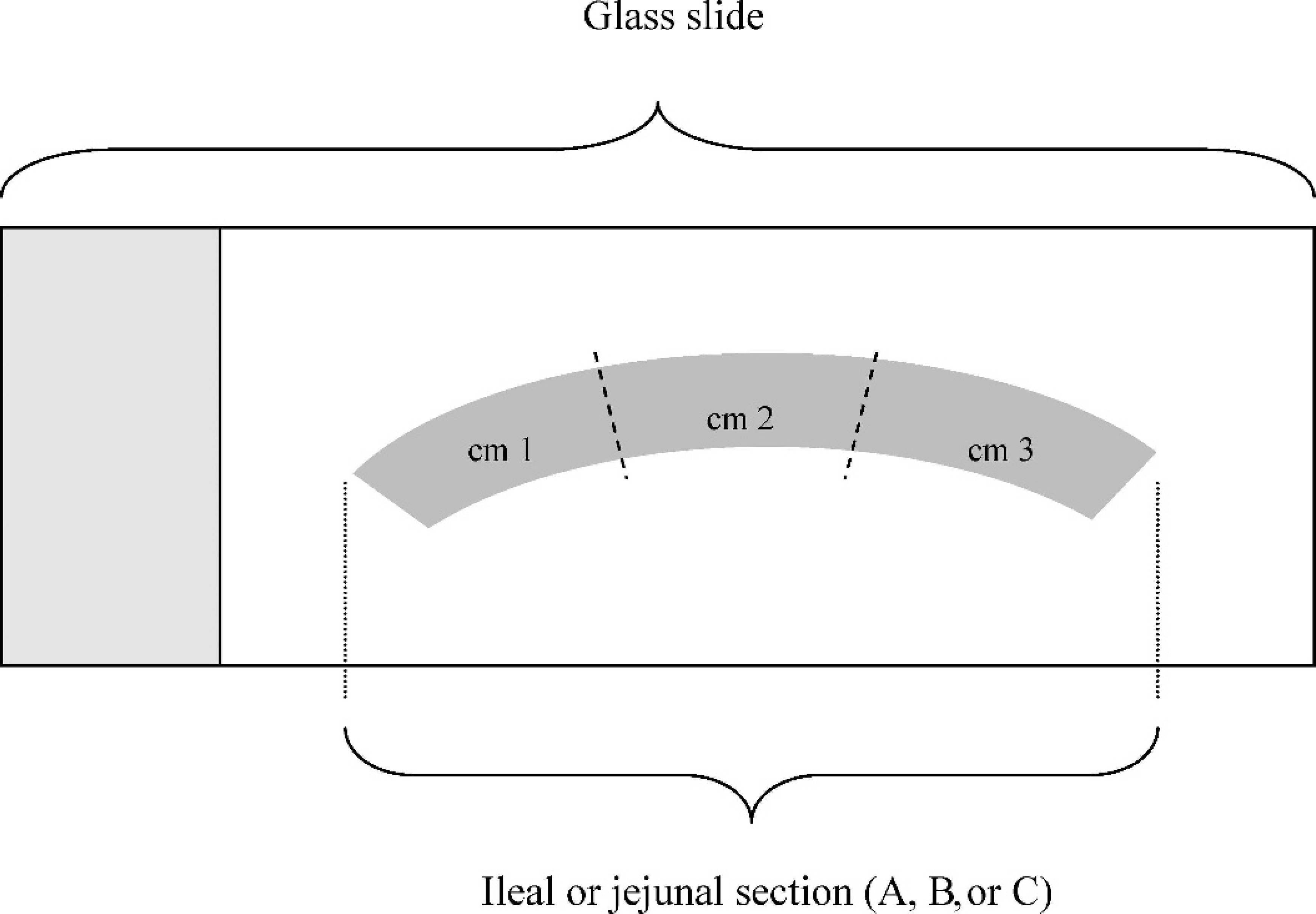
Schematic diagram of the separation of the 30-mm section evaluated histologically into 1-cm sections (cm 1, cm 2, and cm 3) on glass slides.
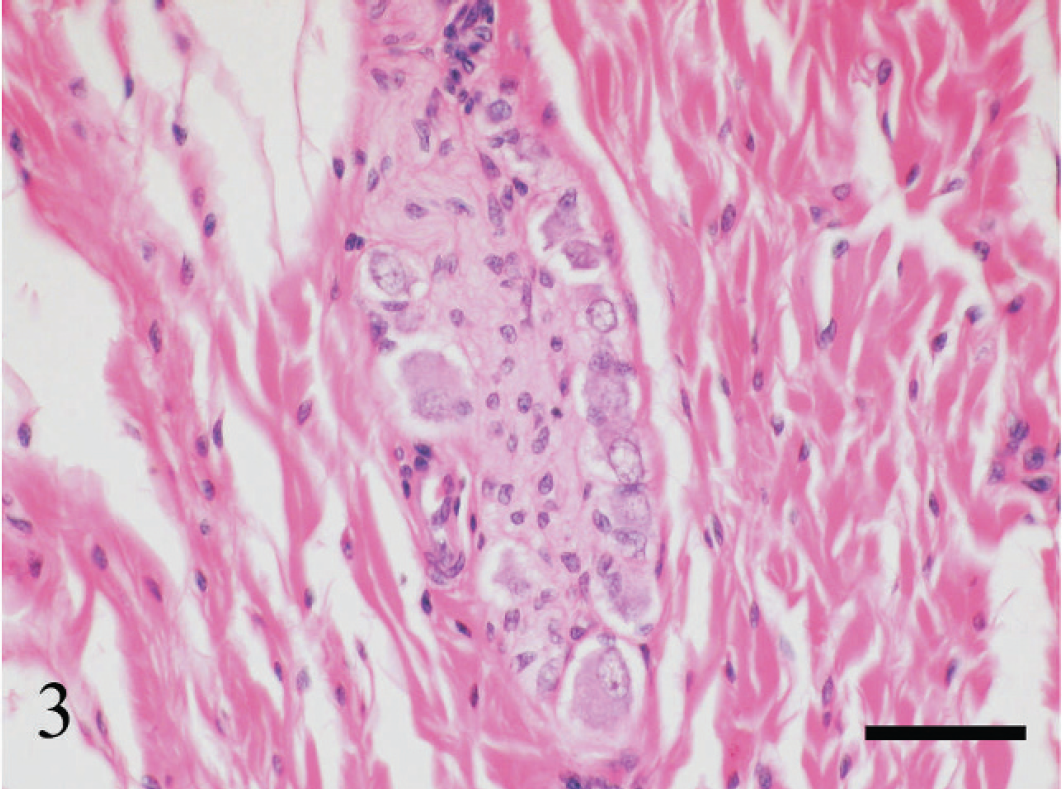
Group of neurons in the submucosal plexus in formalin-fixed ileum from a case of colic (chronic-active enteritis). The neurons are small with normal, basophilic Nissl substance in the cytoplasm and large nuclei with open, stippled chromatin. Hematoxylin and eosin. Bar = 50 μm.
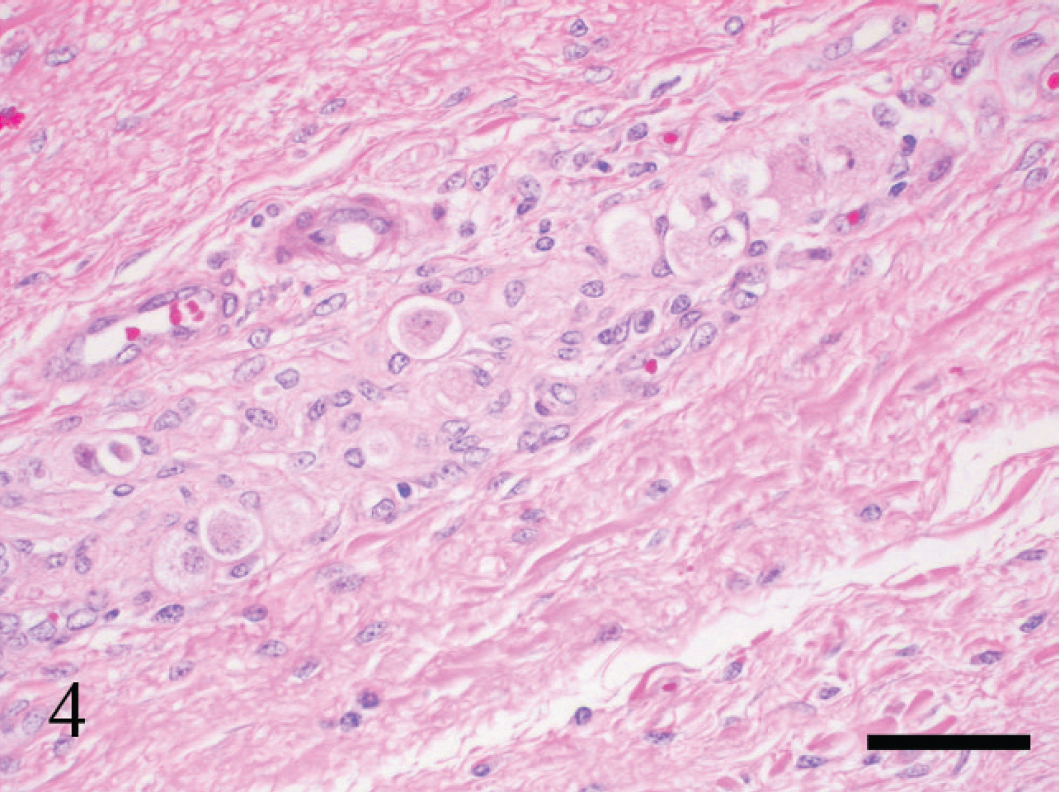
Group of neurons in the submucosal plexus in formalin-fixed ileum from a case of equine dysautonomia. The neurons appear chromatolytic with loss of Nissl substance and cytoplasmic vacuolation. Hematoxylin and eosin. Bar = 50 μm.
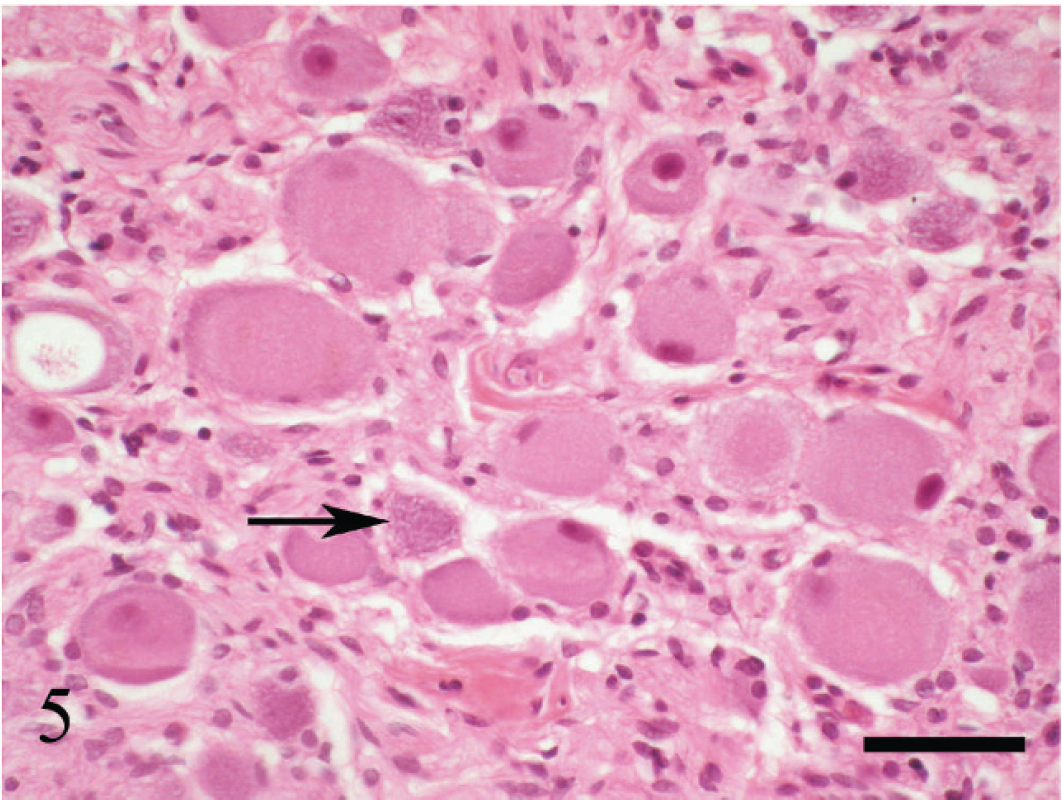
Cranial cervical ganglion from a case of equine dysautonomia to demonstrate the gold standard method of diagnosis. The neurons appear swollen, with markedly chromatolytic, vacuolated cytoplasm and nuclear pyknosis. One normal neuron is present (arrow). Formalin-fixed hematoxylin and eosin. Bar = 50 μm.
Group of neurons in the submucosal plexus in a cryostat section of ileum from a case of colic (chronic-active enteritis). Neurons are indistinct due to loss of clear Nissl substance and nuclear pyknosis. One neuron is swollen with chromatolysis and cytoplasmic vacuolation (arrow). This section was incorrectly classified as equine dysautonomia due to these changes associated with freezing artefact. Hematoxylin and eosin. Bar = 50 μm.
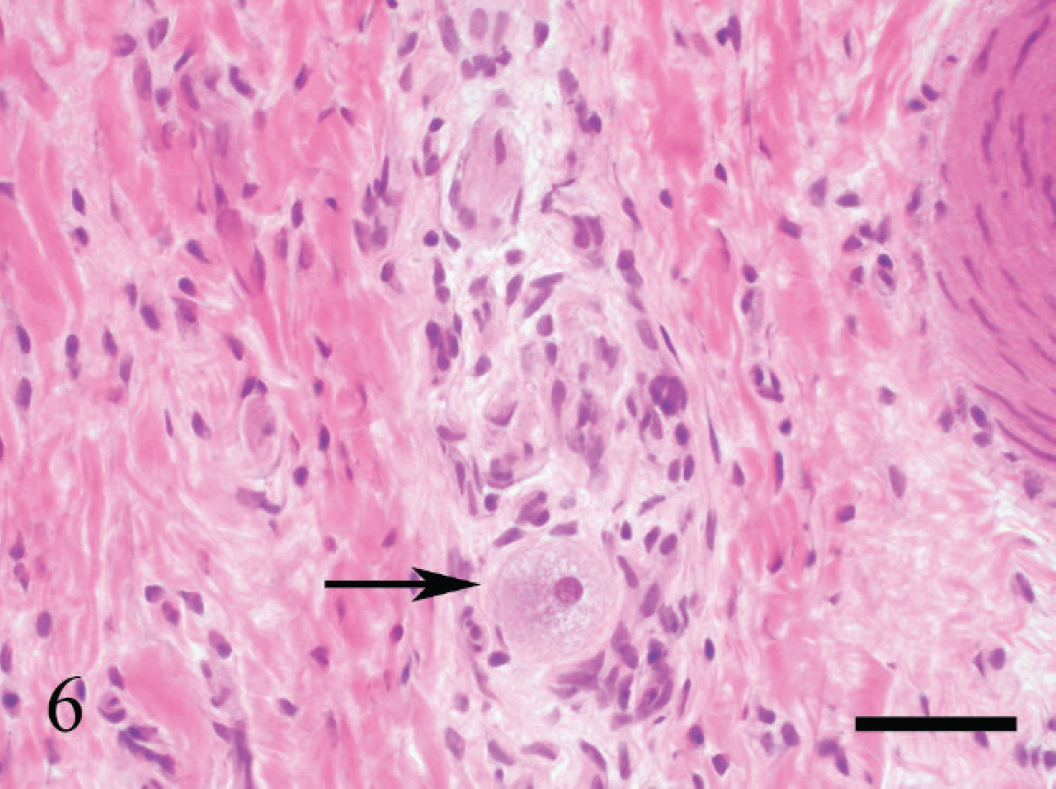
The results of the current study using simulated intestinal biopsies give an indication of the likely reliability of different types of “real” biopsy collected at laparotomy. To the authors' knowledge, this is the first study in which their diagnostic value is critically evaluated. The diagnosis of ED can be highly accurate (100% sensitivity and 100% specificity) using 1-cm long biopsies of formalin-fixed ileum, but false positives may occur with cryostat sections of ileum, which is not improved by examination of larger or serial sections. This is of concern, because cryostat sections of ileum are often submitted to reduce turnaround time and a false-positive result could result in unnecessary euthanasia of a case that did not involve ED. The degenerative changes in autonomic ganglia and enteric neurons consist of a loss of Nissl substance, resulting in chromatolysis, cytoplasmic vacuolation, eosinophilic spheroids within or adjacent to perikarya, nuclear pyknosis or margination, and a reduction in the number of neurons (Whitwell K: 1997, Histopathology of grass sickness: comparative aspects of dysautonomia in various species (equid, felid, canid, leporid). Proceedings of the 1st International Workshop on grass sickness, EMND and related disorders, pp. 18–20. October 1995, Bern, Switzerland). 6 In the enteric plexuses, it was found that these degenerative changes can mimic freeze artefact (Fig. 6), and because diagnosis is often based on subtle changes, this is likely to account for the low specificity of the cryostat sections in the present study.
Selected results with sensitivity, specificity, and 95% exact binomial confidence interval for diagnosis of equine dysautonomia (ED). *
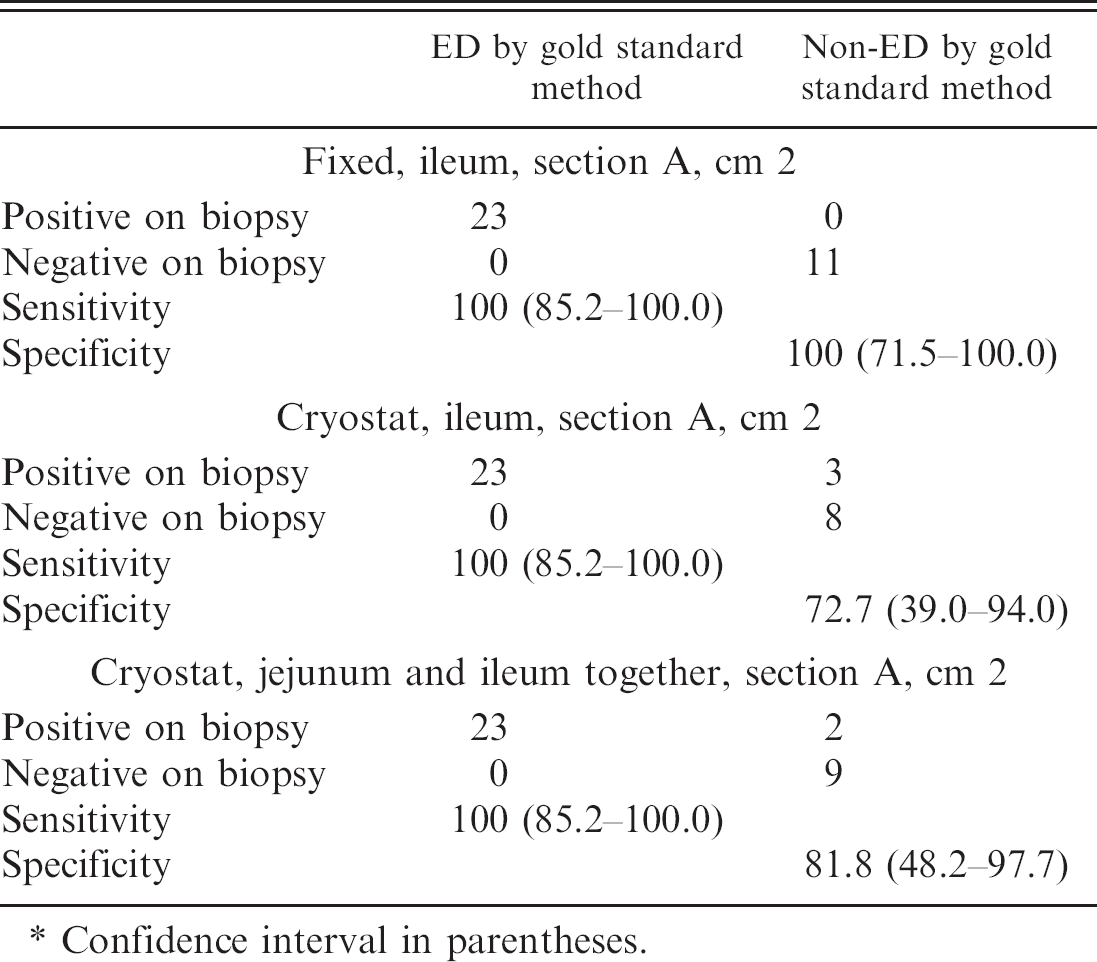
Confidence interval in parentheses.
One study investigated the severity of neurodegeneration in the small intestine in ED cases and demonstrated that in some cases (1 in 14 acute and 2 in 14 subacute), the jejunum was more severely affected than the ileum, whereas in the remaining cases, the reverse was true. 3 However, in none of the cases in the present study was the jejunum more severely affected, and combining an examination of ileum with jejunum was of no advantage for fixed or cryostat sections.
Despite the clear diagnostic benefits of using formalin-fixed sections, as demonstrated in the present study, the clinical requirement for a rapid diagnosis, preferably intraoperatively, must be balanced against the longer time required for processing fixed sections. However, the advent of microwave-assisted tissue processing is likely to reduce this problem, because it can accelerate both formalin fixation and processing such that formalin-fixed sections can be produced in less than 3 hr.
A previous study of rectal biopsy as a diagnostic tool in ED demonstrated a sensitivity of 71% and specificity of 100%. Simulated formalin-fixed biopsies were collected postmortem from 14 cases of ED and 10 control horses, using the presence of at least 3 chromatolytic neurons as the diagnostic criterion. 10 Thus, 29% of their cases would have been falsely negative using this method if reproduced using real rectal biopsies. Rectal biopsy would therefore have no advantage over ileal biopsy from the point of view of correct diagnosis. However, a combination of the 2 techniques (i.e., rectal biopsy followed by examination of fixed sections of ileum obtained at laparotomy of cases negative on rectal biopsy) would avoid a considerable number of laparotomies conducted on suspected ED cases. Further assessment of this combined protocol in clinical practice is warranted.
Acknowledgements. The authors thank the practitioners who referred the cases, the staff of the Dick Vet Equine Hospital who cared for the cases, the staff of the Veterinary Pathology Unit for expert technical assistance, and the Equine Grass Sickness Fund that funded the study.
Footnotes
a.
Somulose®, Arnolds Veterinary Products, Shrewsbury, UK.