
Abstract
Synovial hemangioma was diagnosed in an 8-year-old castrated male Belgian Sheepdog with lameness of 3 months' duration. Pain, soft-tissue swelling, and hemarthrosis were localized to the left stifle joint. Projections of synovial membrane with reddish-purple nodules, excised via arthrotomy, were composed histologically of variably sized vascular channels that were lined by well-differentiated endothelial cells and separated by fibrous septa. Distension of some channels resulted in endothelial disruption, thrombosis, hemorrhage, necrosis, and focal spindle-cell proliferation. The limb was amputated to remove remaining neoplastic tissue. The hemangioma extended focally into the joint capsule and popliteal soft tissue but did not invade skeletal muscle or bone. The dog was free of detectable neoplasia 6 months after amputation. Synovial hemangioma is a rare benign vascular proliferation in people, most commonly in the knee, and should be included in the differential diagnosis for canine synovial tumors.
Synovial sarcoma is considered the most common tumor of canine joints and is the only primary synovial tumor listed in common classification schemes.8,9 In a retrospective study of 35 canine synovial tumors, there were 18 histiocytic sarcomas, 5 synovial cell sarcomas, 6 myxomas, 2 malignant fibrous histiocytomas, 2 undifferentiated sarcomas, and 1 each of fibrosarcoma and chondrosarcoma.3 Vascular tumors are common in the skin and subcutis of dogs but are not recognized in the canine synovium.5 Hemangioma or vascular hamartoma has been described in tendon sheaths but not intra-articular synovium of young horses.8 Human synovial hemangioma is usually classified separately from tendon sheath tumors4 and is defined as a benign vascular proliferation or hamartoma arising in articular or bursal synovial membrane.6 We report a case of synovial hemangioma in the stifle joint of a dog.
A 28-kg, 8-year-old, castrated male Belgian Sheepdog was evaluated for left hind limb lameness of 3 months' duration. Lameness was mild, but soft-tissue swelling was obvious around the left stifle, mainly on the medial aspect of the joint. Aspirated synovial fluid was hemorrhagic. No cranial drawer movement of the stifle joint could be elicited. Radiographically, soft-tissue swelling was present in the cranial and medial aspect of the stifle and displaced the infrapatellar fat pad ventrally. Bony changes were not evident in the stifles or coxofemoral joints. Thoracic radiographs were within normal limits.
Surgical exploration of the left stifle was performed via a 5-cm long incision of the joint capsule along the craniomedial aspect of the joint. Surgical findings included hemarthrosis and several reddish-purple nodular masses (up to 1 cm in diameter) attached by stalks to the synovial membrane. The cruciate ligaments were unremarkable. Accessible nodules were removed and immersed in formalin along with samples of adjacent synovial membrane. Tissues were processed routinely for microscopic evaluation.
Histologically, the biopsy specimens consisted of finger-like projections that were up to 3.5 cm long, 3 to 5 mm thick, and lined by synoviocytes. Capillary-sized to cavernous spaces within the projections were filled with blood, lined by 1 layer of well-differentiated endothelial cells and separated by fibrous connective tissue (Figs. 1 –3). Slit-like vascular channels were occasionally arranged in a radiating pattern around a mature well-differentiated vessel (Fig. 1). Some cavernous spaces were distended up to 5 mm in diameter by partially organized thrombi. Thrombosis and endothelial damage were associated with hemorrhage and necrosis of adjacent tissue. Disorganized layers of spindloid cells with variable nuclear diameter and chromaticity, prominent nucleoli, and rare mitotic figures were occasionally noted adjacent to distended vascular spaces with eroded endothelium.
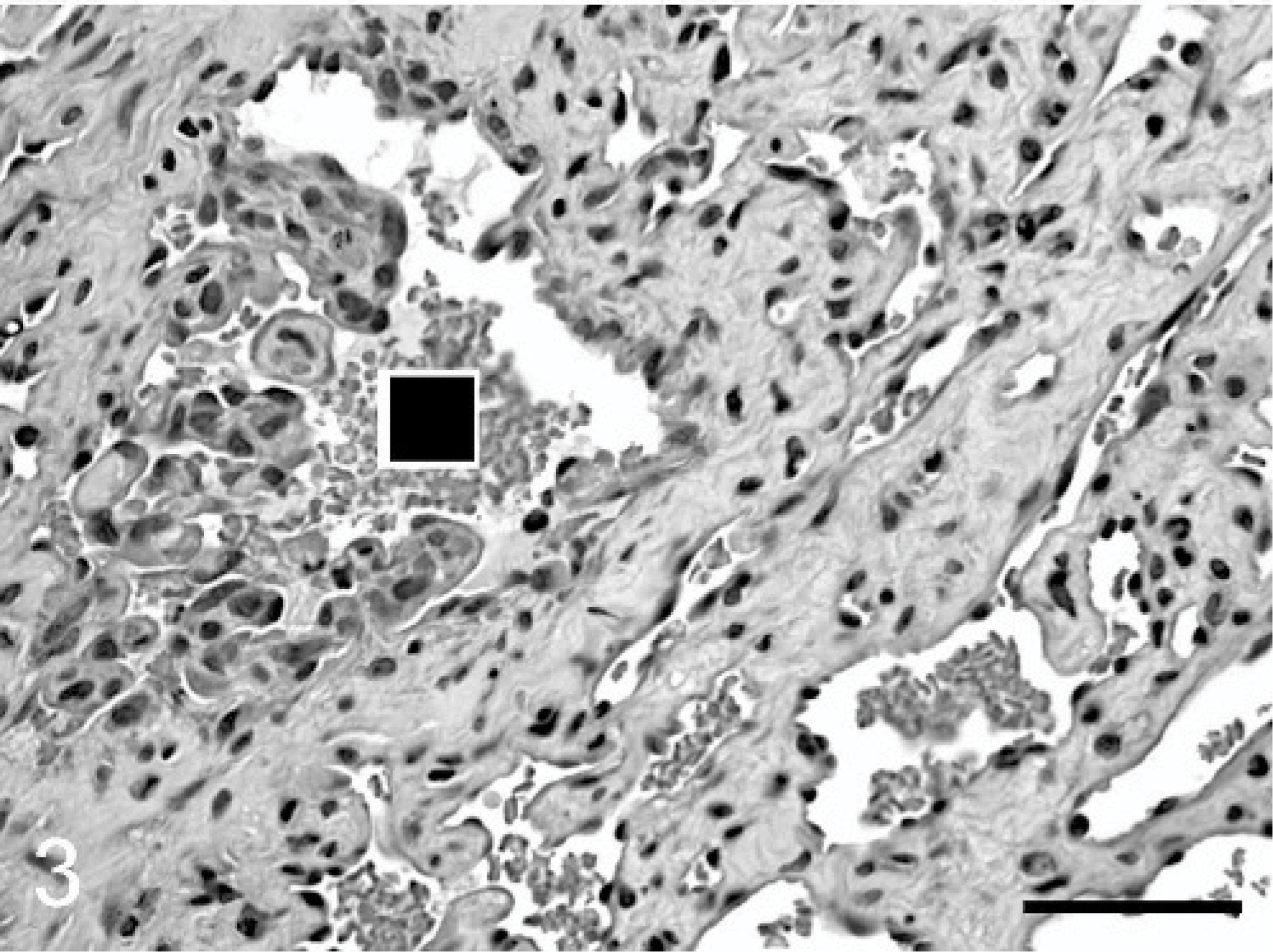
Synovial hemangioma; stifle; dog. Endothelium of 1 vascular channel (black square) forms papillary projections lined by crowded and hypertrophied endothelial cells. HE. Bar = 100 μm.
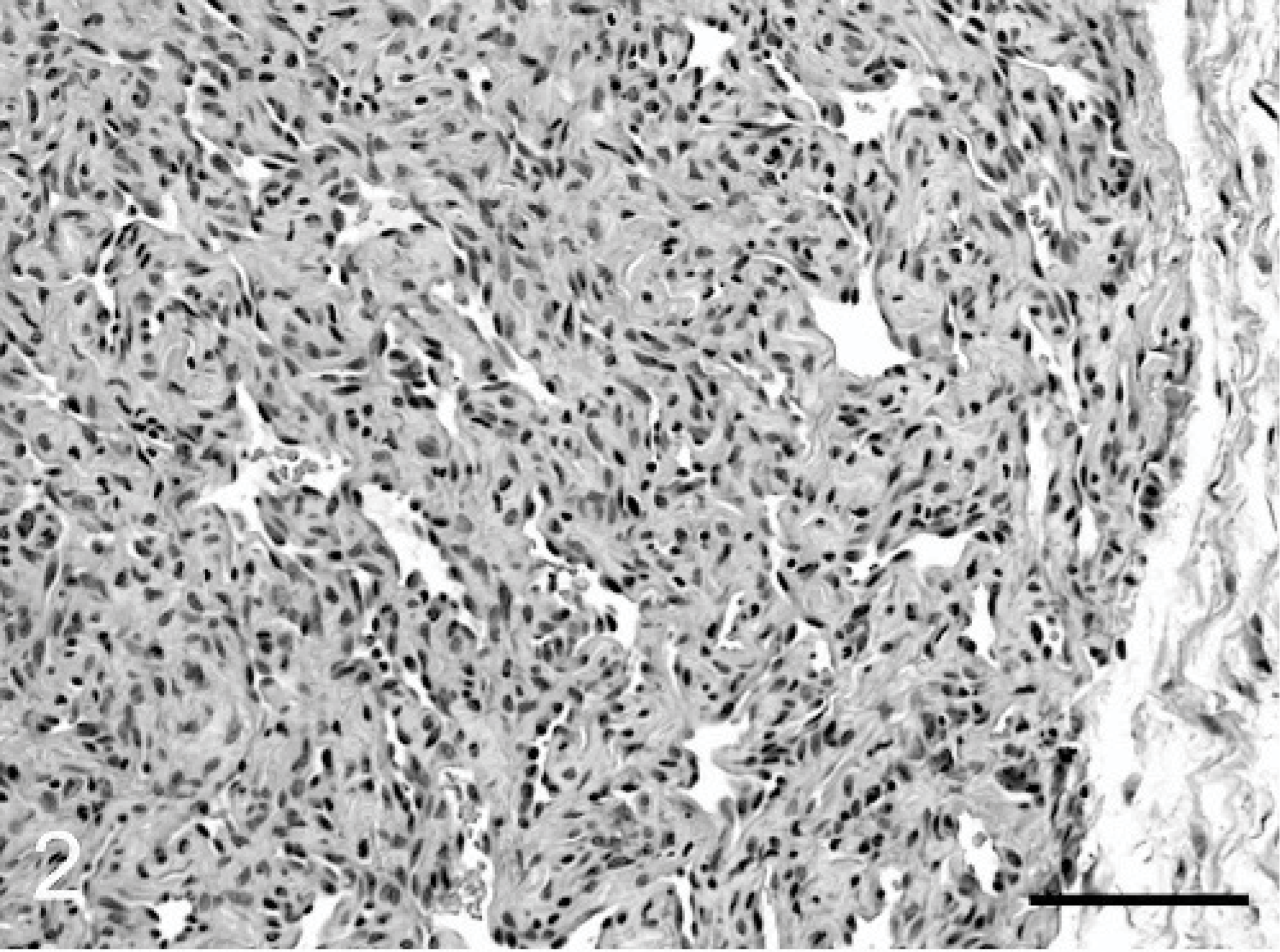
Synovial hemangioma; stifle; dog. Neoplastic tissue consists of narrow vascular spaces lined by a layer of endothelial cells and separated by dense fibrous stroma. The margin of the hemangioma forms an abrupt border with loose fibrous tissue of the joint capsule (right). HE. Bar = 200 μm.
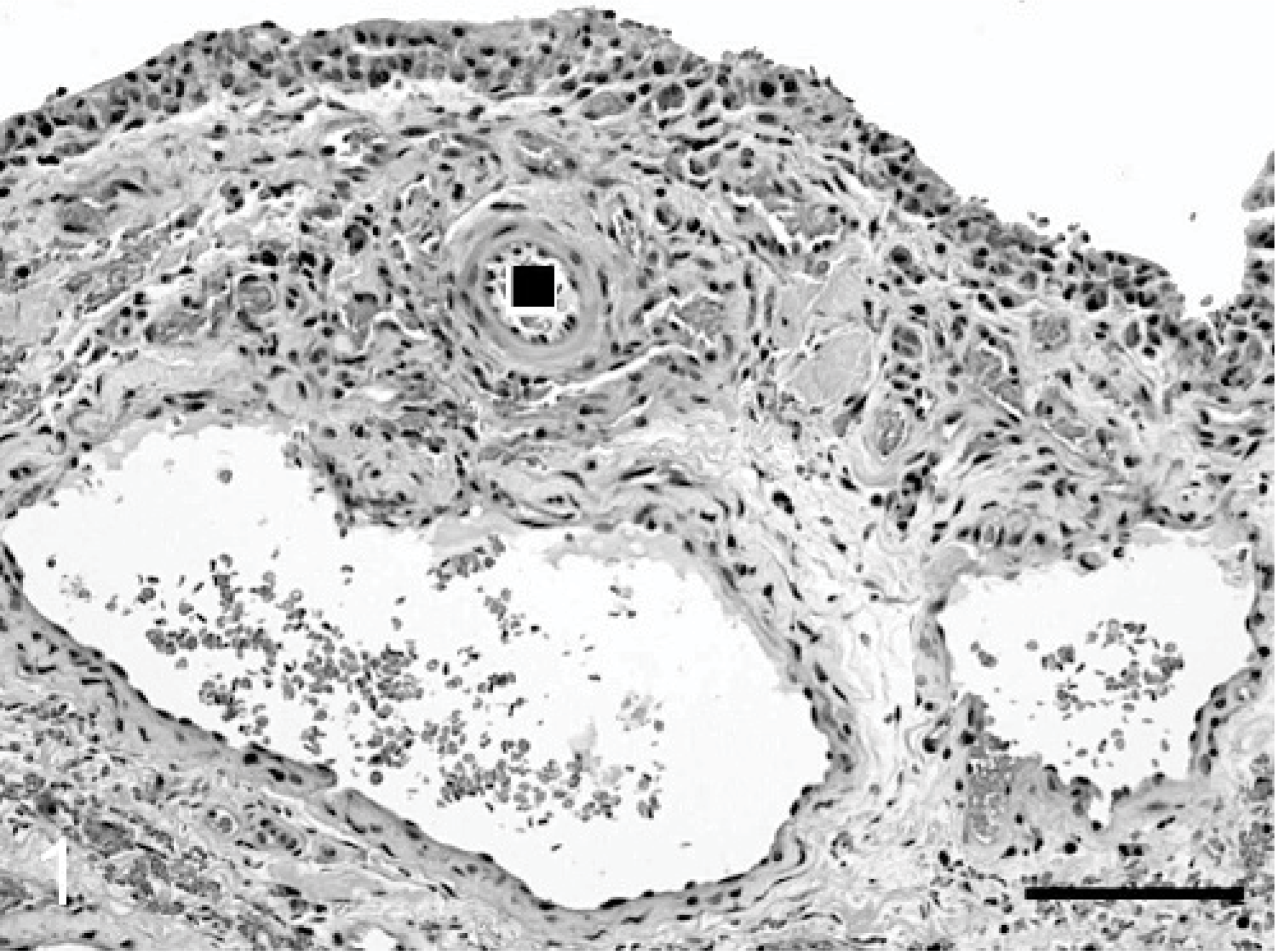
Synovial hemangioma; stifle; dog. Synoviocytes line the surface (top) of this synovial membrane projection. Remaining tissue is composed of vascular channels up to 1 mm in diameter, lined by well-differentiated endothelial cells, and separated by loose fibrous stroma. One normal vessel (black square) is in the midst of the abnormal vascular spaces. HE. Bar = 200 μm.
Fibrous septa between vascular channels varied in density and cellularity (Figs. 1, 2). The spindle cells in these septa were mixed with lipid-laden histiocytes and deposits of hemosiderin and hematoidin. Immunohistochemically, cells lining the vascular channels reacted strongly and uniformly with antibody to the endothelial marker, CD31. Synoviocytes were negative for this marker, and only rare cells in the scattered areas of spindle-cell proliferation between vascular spaces were positive for CD31. The spindle cells were negative for the leukocytic marker, CD18, used in this case to rule out histiocytic sarcoma.
The vascular proliferation occupied much of the subintimal synovium, but its border with subjacent joint capsule was generally abrupt (Fig. 2). Although the endothelium was well differentiated in most vascular channels, a few vascular spaces had papillary intimal invaginations that were lined by crowded and hypertrophied endothelial cells with large hyperchromic nuclei (Fig. 3).
A diagnosis of hemangiosarcoma, either primary or metastatic, was considered. No tumors were evident in heart or abdomen by ultrasonic examination. The affected limb was amputated 1 week after the initial biopsy procedure. The amputated left hind limb was dissected to determine the extent of the tumor. A 10 mm × 6 mm × 4 mm brown nodule, deep to the popliteal lymph node along the popliteal surface of the femur, contained saccular or cylindrical spaces, usually <1 mm in diameter, that were filled with clotted blood. Bluish discoloration, evident through the stifle joint capsule, especially around the medial femoral condyle, was attributed to the presence of blood-filled cavernous spaces in remaining synovial nodules. These nodules were yellow brown to red brown, up to 4 mm in diameter, and scattered through the synovial membrane, especially at sites distant from the arthrotomy incision, i.e., deep and lateral to the patella, and caudal to femoral condyles. Although hemarthrosis had been observed during arthrotomy 1 week previously, only scanty red-brown synovial fluid remained in the stifle joint of the amputated limb. The synovial membrane was discolored yellow brown to red brown, as were cruciate ligaments and menisci.
Histologically, the popliteal lymph node had sinus histiocytosis with erythrophagocytosis and hemosiderosis but no abnormal vascular channels. The nodule near the popliteal surface of the femur resembled the original synovial biopsy specimens and consisted of vascular channels lined by well-differentiated endothelial cells and separated by fibrous septa with light infiltration by mast cells and siderophages. Some vascular channels had 1 or 2 layers of fibroblast-like cells peripheral to the endothelium. Mitotic figures were absent in most fields (0 to 1 mitotic index). The larger vascular spaces contained poorly organized thrombi with necrosis of adjacent tissue.
In the remaining synovial membrane of the stifle, proliferation of synoviocytes and predominantly lymphoplasmacytic inflammation were attributed to the partial synoviectomy 1 week before amputation. Abnormal vascular channels, up to 8 mm in diameter, were mainly limited to the caudal aspect of the femorotibial joint. The vascular proliferation extended focally into adipose tissue of the femorotibial joint capsule and formed clusters of closely apposed cavernous blood-filled spaces (<500 μm in diameter) lined by a layer of well-differentiated endothelial cells. Neoplastic tissue was not detected in sections of femur, tibia, patella, or adjacent skeletal muscle.
Histologic findings were considered more consistent with hemangioma or vascular hamartoma than with hemangiosarcoma. Most of the tumor apparently had been removed during the initial arthrotomy procedure. Remaining neoplastic tissue was mainly in the caudal aspect of the joint and confined to synovial membrane, joint capsule, and immediately adjacent adipose tissue.
The dog recovered from amputation without complications. Physical examination with abdominal ultrasound and 3-view thoracic radiographs, performed 6 months later, revealed no evidence of recurrence or spread of the synovial tumor.
Synovial hemangioma is defined as a benign proliferation of blood vessels within the synovium of a joint or bursa.6 It is classified as one of the deep hemangiomas, which usually involve skeletal muscle, or, less commonly, synovium, bone, nerve, or lymph node.6 Since the first description in 1856,1 an estimated fewer than 200 cases of human synovial hemangioma have been reported.12 In a 20-year period at Mayo Clinic, synovial hemangioma accounted for only 11 of 95 “tumor-like joint conditions.”2 At the Armed Forces Institute of Pathology, 26 cases of synovial hemangioma were received for consultation between 1960 and 1985; archived records and specimens were available for 20 cases, forming the basis for one of the larger retrospective studies.4 In that study, the knee joint was involved in 12 cases; the predominant pattern in 10 cases was cavernous hemangioma. Thirteen patients were male. Patient age at presentation ranged from 9 to 49 years (mean, 25 years) with 1 month to 8 years' (mean, 2 years) duration of symptoms (usually pain and swelling). Symptoms were evident by 16 years of age in 12 of 20 patients. Other reports substantiate the predilection of human synovial hemangioma for the knee and for onset during adolescence or young adulthood,7,11–13 with only occasional reports in older people.4,10 Partly because of the youthful onset of most cases, synovial hemangioma is considered by some to be a vascular hamartoma or malformation rather than a true neoplasm.11–13 However, other pathologists do not attempt to distinguish between hemangioma and vascular hamartoma.4,6
Synovial hemangioma or vascular hamartoma is recognized in carpal and digital tendon sheaths of young horses, usually presenting by 2 or 3 years of age.8 This benign proliferation may invade adjacent tissue and recur after incomplete excision but does not have histologic atypia and does not metastasize.8 In human medicine, hemangiomas of tendon sheaths are usually classified separately from those of intra-articular synovium.4 Hemangioma of tendon sheaths or articular synovium is not a recognized entity in dogs. Furthermore, although hemangioma is a common canine cutaneous or subcutaneous tumor,5 dogs are not prone to develop juvenile hemangiomas or hamartomas in skin, subcutis, or deeper soft tissues. The dog of this report was 8 years old at presentation, with only 3 months' duration of lameness.
Recognition of focal papillary endothelial hyperplasia and nuclear atypia in this dog's tumor prompted consideration of hemangiosarcoma initially, but endothelial atypia without solid proliferation or invasiveness may be seen in human synovial hemangiomas and does not warrant a diagnosis of angiosarcoma.6 Most of the tumor in this dog was well differentiated without atypia or multilayering of endothelial cells. Additionally, the tumor was within the synovial membrane, with only limited invasion of the joint capsule.
A vascular tumor should be considered in the differential diagnosis for a dog with nontraumatic hemarthrosis and red synovial nodules. The dog of this report had no hemangiosarcoma in skin, bone, heart, or abdominal cavity, thus alleviating the initial concern that the synovial tumor was a metastatic hemangiosarcoma. Histologic features of the tumor were similar to those of human synovial hemangioma, which is almost always cured by complete resection and should be distinguished from angiomatosis, which invades multiple tissue planes, such as bone, muscle, and subcutis, and often recurs after excision.4 This dog had residual neoplastic tissue after the initial excision but only limited invasion of the stifle joint capsule without extension into skeletal muscle, bone, or subcutis, and the dog is clinically normal 7 months after amputation of the affected limb.
Footnotes
Acknowledgement
We thank Kenneth Devaney, MD, JD, for reviewing histologic sections.