
Abstract
Three independent, fatal outbreaks of Streptococcus canis infection occurred in a 2-year period in shelter cats. The outbreaks occurred in Northern California (Yolo County), Southern California (Kern County), and North Carolina (Guilford County). An estimation of the affected population is >150 cats among 3 affected shelters, with a mortality rate of up to 30%. Among 20 cats submitted for necropsy there were 2 distinct pathologic presentations. The first (shelters 1 and 2) was skin ulceration and chronic respiratory infection that progressed, in some cats, to necrotizing sinusitis and meningitis. The second (shelter 3) was rapid progression from necrotizing fasciitis with skin ulceration to toxic shock-like syndrome, sepsis, and death. S canis was the sole pathogen identified in most cases. Whether hypervirulent S canis strains exist is unknown; there is little understanding of how these bacteria cause invasive disease in cats.
Streptococcus canis, possessing the Lancefield group G antigen, is present in up to 10% of cultures from the nasal cavity of cats with chronic upper respiratory infections (URI) (M. Lappin, personal communication). S canis in cats has been associated with epidemics of arthritis,3 cervical lymphadenitis, urogenital infections, upper respiratory infections, and neonatal septicemia.2 Most of these reports reflect time-limited outbreaks of disease in young, intensively housed, closed-colony animals. In this report we describe 3 independent outbreaks, affecting more than 150 cats, of S canis infection. The cases were reported by referring veterinarians or staff from independent shelters that contacted the Shelter Medicine Program at UC Davis regarding increases in mortality among cats of all ages.
Shelter Outbreaks 1 and 2
Outbreak 1 occurred over a 2-month period at the Yolo County Animal Shelter in Northern California in a single building housing 40 kittens and cats. Approximately 25% of these animals developed ulcers/sinusitis or both. Outbreak 2 occurred in a shelter in Guilford County, North Carolina, in several buildings housing approximately 120 cats. The outbreak occurred over a 6-month period during which time approximately 30% of the cats were treated for upper respiratory infection, and up to 85% of these developed ulcers and/or sinusitis. In both shelters, dogs were housed separately but cared for by common staff.
Clinical signs reported in kittens and cats (age range 4 month to adult) from shelters 1 and 2 included skin ulceration of the face, feet or limbs, severe prolonged respiratory infection, and in some cases acute swelling along the nasal bridge (Fig. 1) and death. Animals of all ages were affected. Eleven cats from these 2 outbreaks (3 from shelter 1, 8 from shelter 2) were submitted for necropsy to the pathology service of the Veterinary Medical Teaching Hospital at the School of Veterinary Medicine, University of California Davis. All 11 cats had suppurative, necrotizing sinusitis (Fig. 3) and rhinitis. Necrosis with perforation of the nasal bone, where it overlies the frontal sinus, occurred in 5/11 cats (45%). Subsequent cellulitis and edema of the subcutaneous tissues overlying this region of osteolysis caused the nasal bridge swelling described clinically. In 4/11 cats (36%) there was extensive suppurative meningitis (Fig. 3). Skin ulceration was present in 9/11 cats (81%). The distal limbs were the most frequently affected sites (7/9, 77%) with 2 or more limbs affected in 4/9 cases (44%). The skin surrounding the regions of ulceration was typically thickened by edema, hemorrhage, and necrosis that extended within the fascia and subcutis up to 2 cm distal from overt sites of ulceration.
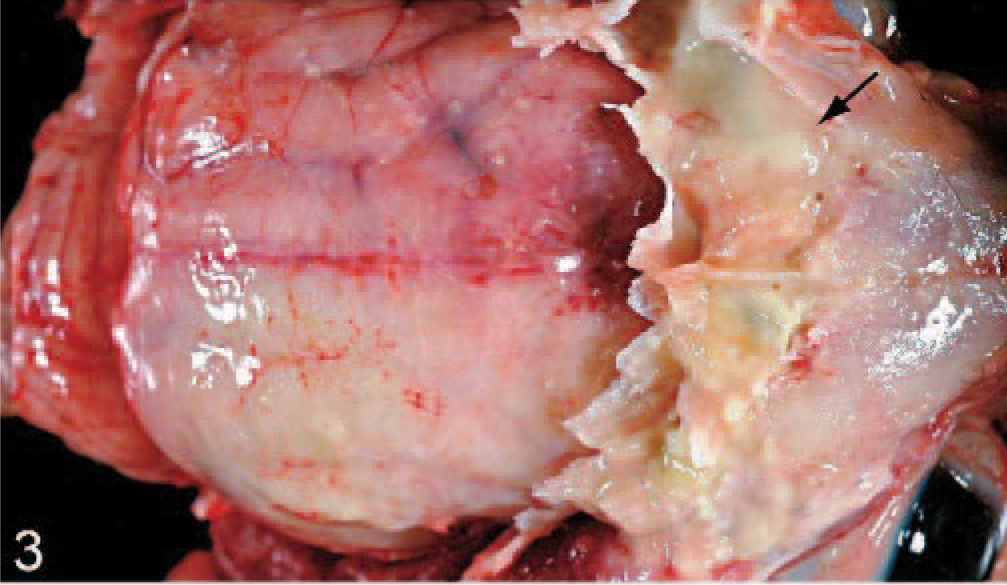
Head; cat 6, shelter 2. The calvarium and the distal portion of the nasal process of the frontal bone have been removed to reveal purulent material within the frontal sinus (arrow). An intact dura covers purulent material within the subdural space, most notably over the right cerebral cortex.

Cat 3, shelter 2. Swelling of the subcutaneous tissues overlying a perforated nasal bone.
Microbiological culture was performed on samples from the regions of skin ulceration (11/11), frontal sinus (11/11), and meninges (4/11). S canis, Biotype 1, was the sole bacterial pathogen isolated from the frontal sinus and meninges in all cases. Swabs or samples taken from regions of skin ulceration yielded either pure growth of S canis (3/11) or mixed growth including large numbers of S canis (8/11). Tests for other possible concurrent pathogens were performed on oropharyngeal samples and included cell culture and polymerase chain reaction (PCR) for feline herpesvirus (1/11 positive), cell culture for feline calicivirus (6/11 positive) and PCR for Chlamydophila (2/11 positive). Two cats were tested and negative for feline immunodeficiency virus and feline leukemia virus.
Histopathologic examination in each case included the rostral nasal region with ventral nasal conchae, ethmoidal conchae, cribriform plate, frontal bone, and frontal sinuses. In all sections there was marked expansion of the subepithelial connective tissue by large numbers of viable and degenerate neutrophils admixed with karyorrhectic debris, with fewer lymphocytes, plasma cells, and macrophages. Turbinate boney septae in all cats, and in some cats the nasal process of the frontal bone and/or cribriform plate, were regionally thin or perforated, with extensive osteoblastic and osteoclastic activity (Fig. 2). In cats with brain and meningeal involvement, the meninges overlying the olfactory tracts and the rostral cortex were markedly expanded by fibrin and neutrophils with lesser numbers of plasma cells and lymphocytes. Many vessels were dilated and filled with a combination of fibrin and dense colonies of bacteria (Fig. 4). Histopathologic examination of the skin lesions showed chronic, ulcerative dermatitis with regional neutrophilic cellulitis, fasciitis, and edema. Gram's stain of affected tissue revealed florid, dense gram-positive cocci within the areas of inflammation.
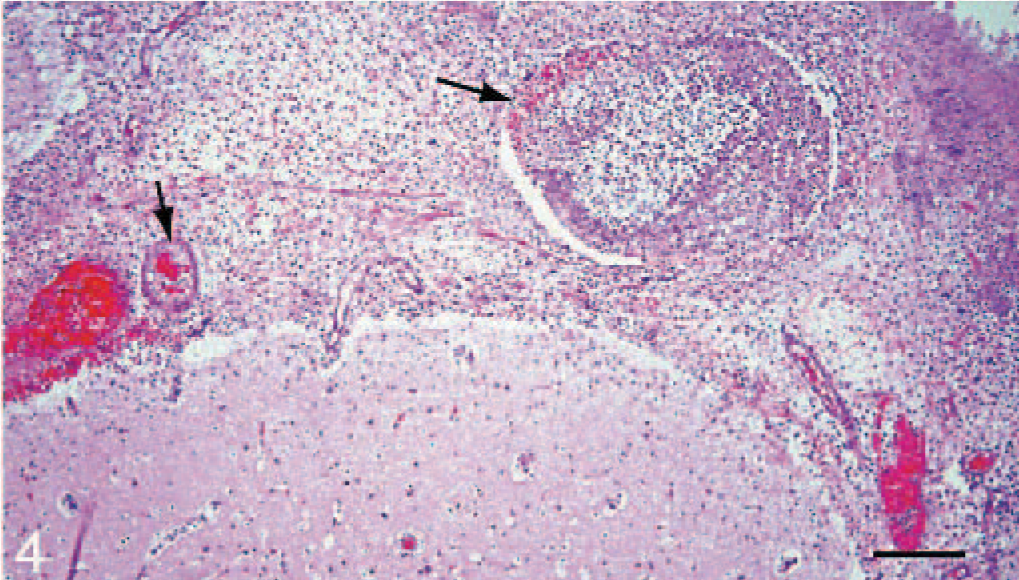
Brain, meninges; cat 6, shelter 2. The meninges are markedly expanded by a population of dense viable and degenerate neutrophils. Multiple vessels are dilated and contain thrombi (arrows) and coccoid bacteria. HE. Bar = 100 μm.
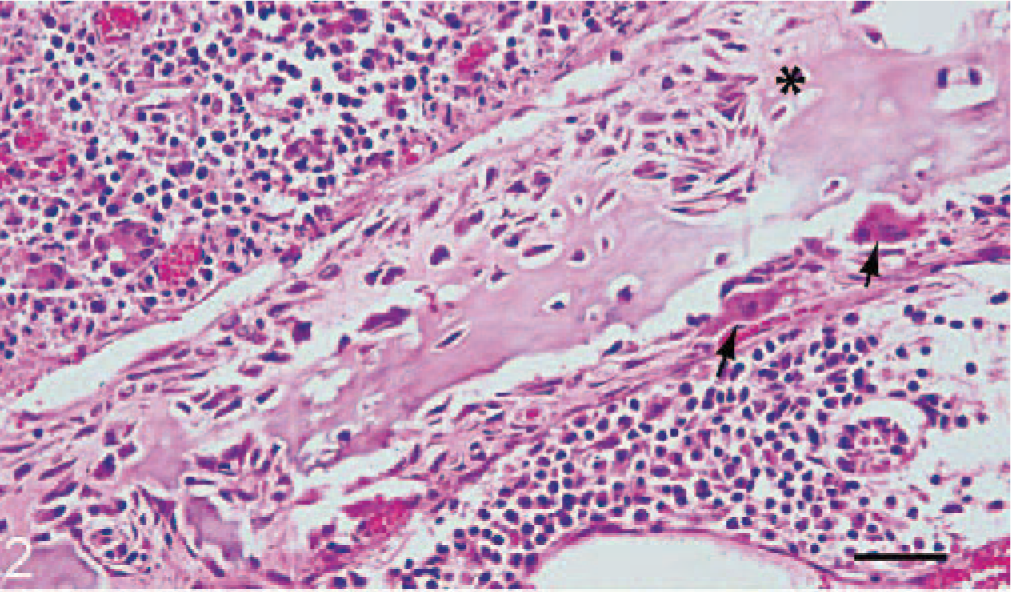
Nasal turbinate; cat 1, shelter 1. There is extensive osteoblastic (∗) and osteoclastic (arrows) remodeling of the nasal turbinate bone. Dense mixed inflammatory cells expand the subepithelium. HE. Bar = 50 μm.
Shelter Outbreak 3
Outbreak 3 occurred in a shelter in Kern County, Southern California, in a single room housing approximately 40 feral cats. The outbreak occurred over a 6-month period during which time approximately 30% of cats were affected. In 1 month's time, for example, 12 cats (of a population of 37) were found dead or moribund with ulceration and oozing of 1 or more paws. Death typically occurred within 4–6 days of introduction to the room. Full necropsy was performed on 9 cats submitted. Focal to multifocal subcutaneous swellings were present on all cats. These swellings were associated with ulceration (Fig. 5), edema, hemorrhage, necrosis, and rarely purulent exudate dissecting within subjacent fascia and subcutis up to 7 cm distal from overt sites of ulceration in 7/9 cats (78%). The distal limbs were the most frequently affected sites (8/9, 89%) and 2 or more limbs were affected in 7/9 cases (78%). The lips and or nasal plane were less frequently affected, and a single cat had ulceration limited to the lateral thoracic skin just ventral to the dorsal spinous process of the fourth thoracic vertebrae. Among those cats with distal limb lesions, ulcers centered on nail beds with nail sloughing and tissue necrosis that often spanned, within the adjacent deep dermal tissues, from the subungual region to the fatty/connective tissue of footpads (Fig. 6). Ulcers elsewhere (body wall, forelimb), were alopecic, up to 5 cm in diameter and were slightly raised, exudative, and erythematous.

Third phalanx, thoracic limb, parasagittal section; cat 3, shelter 3. The subcutis and fascia are edematous (∗) with focal areas of hemorrhage that extend into the footpad.

Skin, thoracic limb; cat 8, shelter 3. A poorly demarcated region of ulceration with exudation.
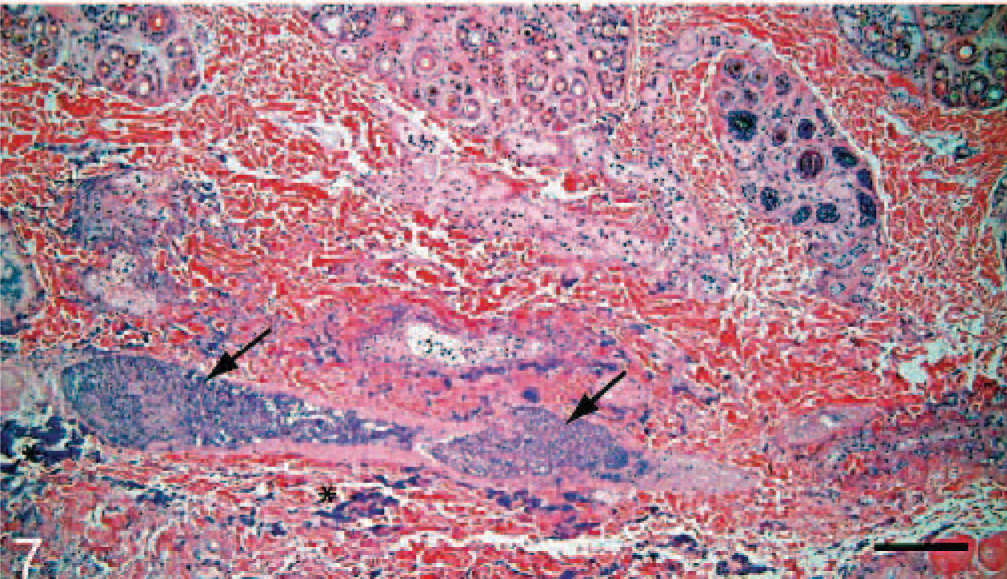
Microbiological culture was performed on samples from the spleen (7/9, 78%), liver (7/9, 78%), and regions of skin ulceration/fasciitis (9/9). S canis, Biotype 1 was the sole bacterial pathogen isolated from the spleen and liver in all cases tested. Swabs or samples taken from fascia, adjacent to ulcerated regions, yielded either pure growth of S canis (3/9, 33%) or mixed growth including large numbers of S canis (5/9, 55%). Histopathologic changes were limited to the skin, lips and nasal planum. There was a dense inflammatory infiltrate of viable and degenerate neutrophils admixed with karyorrhectic debris and dense colonies of gram-positive coccoid bacteria within the deep dermal tissues and extending along fascial planes (Fig. 7) associated with dense colonies of gram-positive coccoid bacteria (Fig. 8). Regionally, edema and hemorrhage separated collagen bundles within the overlying dermis and expanded connective tissue within the panniculus. Fibrin thrombi were sporadically present in arterioles and venules within the deep dermis. Periodically the inflammation extended into the superficial dermis and/or through the epidermis in regions of ulceration. Gram's stain of affected tissue revealed florid, dense gram-positive cocci within the areas of inflammation. In some cats, dense mats of bacteria were present at the periphery of lesions associated with inflammation.
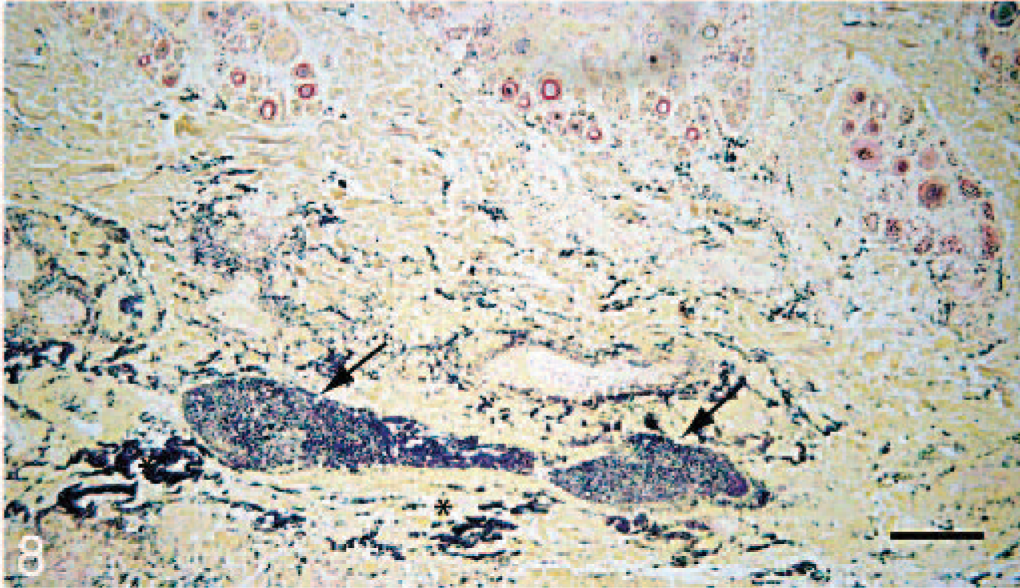
Skin, thoracic limb; cat 2, shelter 3. Dense clusters of gram-positive cocci distend vessels (arrowhead) and separate fibrovascular tissue within the deep dermis. Modified Brown and Brenn Gram's stain. Bar = 100 μm.
Skin, thoracic limb; cat 2, shelter 3. There is a bandlike region of inflammation, necrosis, and edema confined to the deep dermis (arrows). HE. Bar = 100 μm.
The disease caused by S canis infection in the 3 outbreaks described in this study had 2 distinct manifestations. In 1 clinical course, S canis was associated with skin ulceration, sinusitis, and meningitis. In humans, Streptocccus is a common organism isolated in cases of acute suppurative sinusitis with complications, 1 of which is meningitis.5,7 In these cats, meningitis was considered sequelae to frontal sinusitis based on histologic evidence of inflammation and boney remodeling within the cribriform and frontal bone plates. Although other pathogens were detected in the nasal cavity of some cats, none was detected consistently, and all were well within the limits of normal incidence for a shelter environment. It is, nonetheless, possible that historic viral and/or another infection predisposed these cats to Streptococcus colonization. Upper respiratory infection was endemic in both of these shelters, and affected cats may have served as a reservoir for S canis. Although animals were housed in single cages, fomite transmission could readily have occurred through staff handling and medication of cats.
In the second clinical course, restricted to the feral cat room of shelter 3, death occurred quickly in association with necrotizing fasciitis. Standard husbandry for this population of cats dictated that sick cats were not maintained and cats were euthanized after a 5–7 day holding period. Despite initial identification of the causative agent, complete depopulation, and careful cleaning of the facility, there were 2 subsequent recurrences in a 6-month period. The clinical and pathologic features were strikingly consistent with Streptococcus-associated human and canine cases of necrotizing fasciitis with toxic shock syndrome (TSS).6,8,9 In dogs, like cats, the causative organism is S canis.6 In humans, TSS is primarily caused by group A streptococci and necrotizing fasciitis is concurrent in 50% of patients.8 TSS with associated fasciitis kills 30–60% of patients within 96 hours, and nearly half of these patients have no defined portal of entry for the bacteria. In humans, fever, confusion, and increasing pain are the major symptoms;9 in feral cats these symptoms would have been masked or not easily assessable. The diagnosis of toxic shock, in human and in veterinary medicine, relies on the detection of a spectrum of clinical features including hypotension, organ systems failure, early onset of death, and the isolation of bacteria from a normally sterile site.8 In this case, 2/4 of these criteria were fulfilled; death occurred within 24 hours of skin involvement, and bacteria were isolated from both the liver and spleen of affected cats.
Factors other than Streptococcus colonization might have contributed to the emergence or sustentation of these three outbreaks. The management practices of the individual shelters, stress of captivity, and antibiotic choices and regimen could be confounding or contributing to the course or presentation in these cases. None of the 3 shelters described here reported remarkably different conditions prior to the outbreaks; e.g., no marked changes in husbandry had recently occurred, and although the shelters were crowded and some cats were sick with upper respiratory infection, this was not unusual. The management factors behind the emergence of unusually pathogenic strains of S canis in shelter cats remain unknown. Our ability to rule in or out concurrent disease relied on limited premortem information and on gross and histologic pathology; our results do not exclude the possible role of an immunosuppressive condition or pathologically silent viral disease that preceded Streptococcus infection.
Virulence of the specific Streptococcus isolated in these cases is likely to be an important ingredient in emergence and reemergence. Some investigators have attributed virulence, and more specifically fasciitis, to expression of bacterial enzymes such as hyaluronidase, which degrades the fascia.8 Development of TSS is dependent on the presence of superantigens (Sags) in streptococci. Recently, the presence of the Sag, smeZ, was detected in a human S canis isolate although examination of isolates from dogs with TSS or necrotizing fasciitis have failed to detect the presence of Sag genes.1,4,6 A complete understanding of how S canis causes invasive disease would include analysis of the genetic diversity among these isolated species. S canis, although typically considered a commensal and extracellular pathogen in cats, is capable of causing severe life-threatening invasive infections, such as necrotizing fasciitis, sinusitis, bacteremia, and toxic shock–like syndrome.