
Abstract
Mesenchymal hamartoma of the liver is a rare congenital disorder of biliary tract development. During the necropsy of a late-term equine fetus, a markedly enlarged liver of more than two times normal weight was found. Light microscopic review revealed that the normal hepatic parenchyma had been obliterated, replaced, and expanded by abnormal bile ducts surrounded by abundant, myxoid stroma. The lesion was diagnosed as a mesenchymal hamartoma. Small portions of the liver had bridging septa of fibrosis and proliferations of small-caliber abnormal bile ducts, resembling another congenital biliary abnormality termed congenital hepatic fibrosis.
Mesenchymal hamartomas are most often identified as single or multiple discrete masses, although they rarely can occupy most of the liver and enlarge it considerably. They are characterized by a myxoid stroma with fibroblasts, bile ductules, vascular structures, and only islands of hepatocytes. 7 Epithelial-lined and nonepithelial-lined cystic spaces may be present. Mesenchymal hamartoma is the second most common benign hepatic tumor in children 7 but has never been reported in veterinary species. Although a similar congenital lesion of the liver, a mixed hamartoma, composed of hepatocellular and biliary elements, has been described once in a late-term equine fetus, mesenchymal hamartoma has not been previously diagnosed in an animal. 6
This case occurred in a late-term female Arabian fetus submitted to the California Animal Health and Food Safety Laboratory System at The University of California, Davis. The foal was initially moving her ears and eyes as her head was delivered but was found to be not breathing approximately 10 to 15 minutes after the onset of delivery.
The mare was 8 years old, and this was her first foal. The mare received annual vaccinations and was reported to be on a normal diet, with supplemented grain; a vitamin supplement that contained vitamins A, B12, and D; and another supplement that contained biotin. There was no history of previous drug exposure, except for phenylbutazone approximately 1 month before parturition, because of a leg laceration. She had no contact with other horses during her pregnancy. Serologic titers for leptospirosis, equine herpesvirus-1, equine viral arteritis virus, and equine quantitative immunoglobulin G were negative. Liver levels of arsenic, cadmium, copper, iron, lead, manganese, mercury, molybdenum, selenium, and zinc revealed no evidence of intoxication. The liver contained low iron (12.5 ppm; normal, 100–300 ppm), zinc (8.7 ppm; normal, 40–125 ppm), copper (2.4 ppm; normal, 4–7.5 ppm), and selenium (0.073 ppm; normal, 0.3–1.0 ppm) concentrations. This was likely because of the extensive fibrosis and the loss of normal hepatocytes in the liver, as described below.
Gross examination revealed that the fetus had moderate subcutaneous edema in the head and the neck. The abdomen was distended because of a markedly enlarged liver, which was more than twice normal size (∼10% of body weight). The liver was diffusely enlarged, tan, and firm. It was moderately resistant to cutting and had an accentuated reticular pattern. There were no lesions present on the placental membranes, and there was no clear indication that the foal had taken a breath after birth.
Sections of brain, lung, heart, liver, kidney, spleen, thymus, lymph node, adrenal gland, skeletal muscle, tongue, stomach, small intestine, and placenta were fixed in 10% neutral buffered formalin, processed, and embedded in paraffin according to accepted histologic technique. Significant histologic lesions were confined to the liver, which was stained with hematoxylin and eosin (HE), periodic acid-Schiff (PAS) and alcian blue.
Histologically, in the most severely affected areas, there was diffuse obliteration of normal hepatic parenchyma by the presence of broad areas of abnormal, branching, irregularly shaped, small-caliber bile ducts separated by an abundant myxomatous extracellular matrix (Fig. 1). The stroma was moderately cellular, with pale basophilic myxoid extracellular matrix separating the mesenchymal cells. The extracellular matrix was PAS negative, but alcian blue positive, illustrating the myxomatous nature of the matrix. In these areas, hepatocytes were absent or limited to small islands that composed no more than approximately 4% of the total surface area of the section. Most of the hepatocytes contained multiple clear, cytoplasmic vacuoles, typical of lipid (Fig. 2). The abnormal bile ducts had an extensive series of interconnections, but the diameter of the ductular structures was fairly uniform, and there was no evidence of cystic dilatation. The ducts were typically lined by single-cell-thick biliary epithelium. Biliary epithelial cells were moderately pleomorphic, with variation in nuclear size and cell size, and ranged from cuboidal to squamous. The lumen of the ducts frequently contained eosinophilic amorphous debris. The interface between the abnormal ductular structures and the hepatocytes was characterized by a subtle grading from apparent biliary epithelium lining the ducts to areas with cells resembling hepatocytes lining ducts and forming acini (Fig. 2). No portal tracts were identified, but there were structures that contained veins and arteries surrounded by connective tissue distributed throughout the mass.
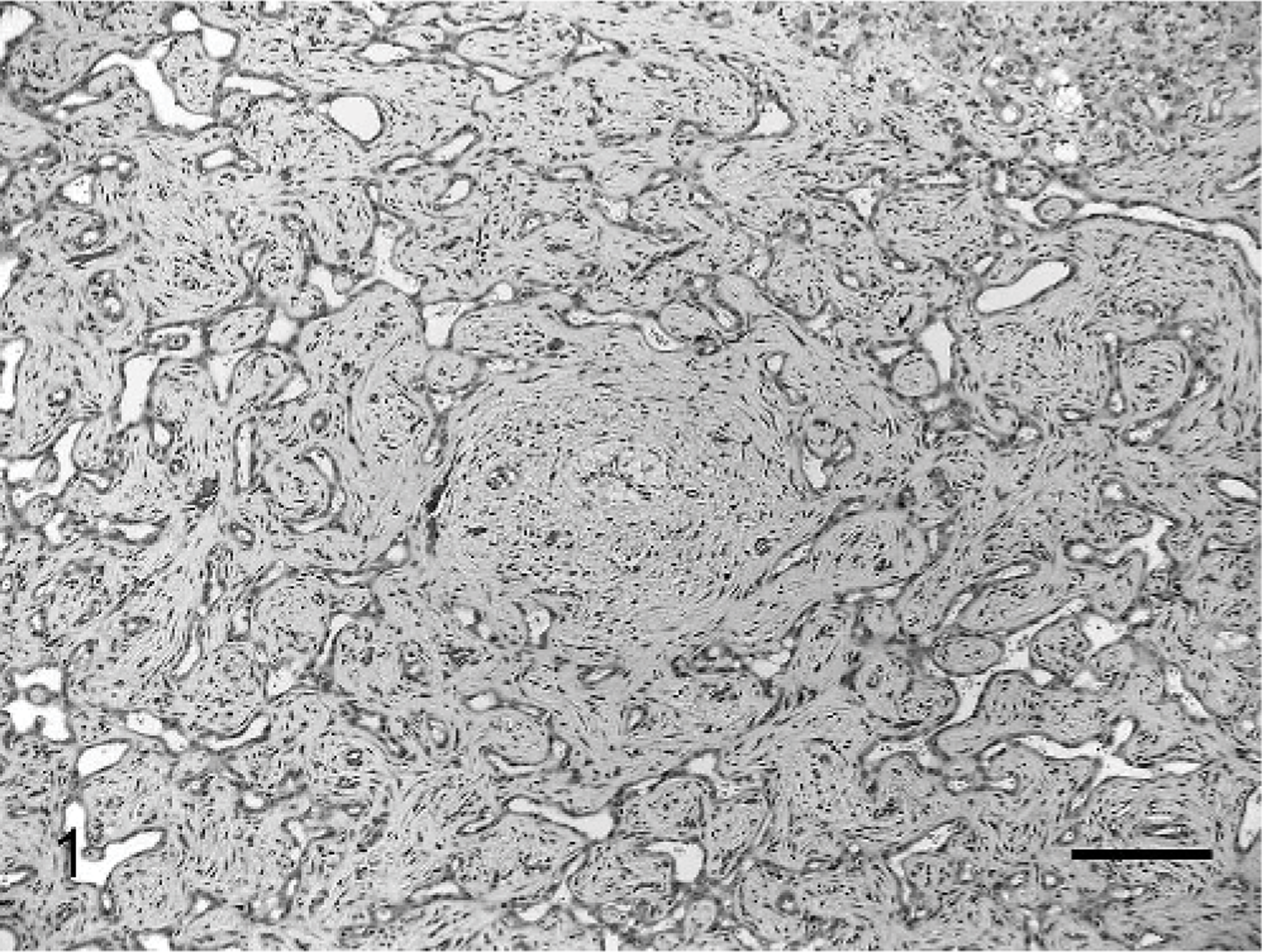
Liver; equine. Proliferated, irregularly shaped, small-caliber bile ducts separated by an abundant myxomatous extracellular matrix, making up the majority of the hamartoma. HE. Bar = 140 microns.
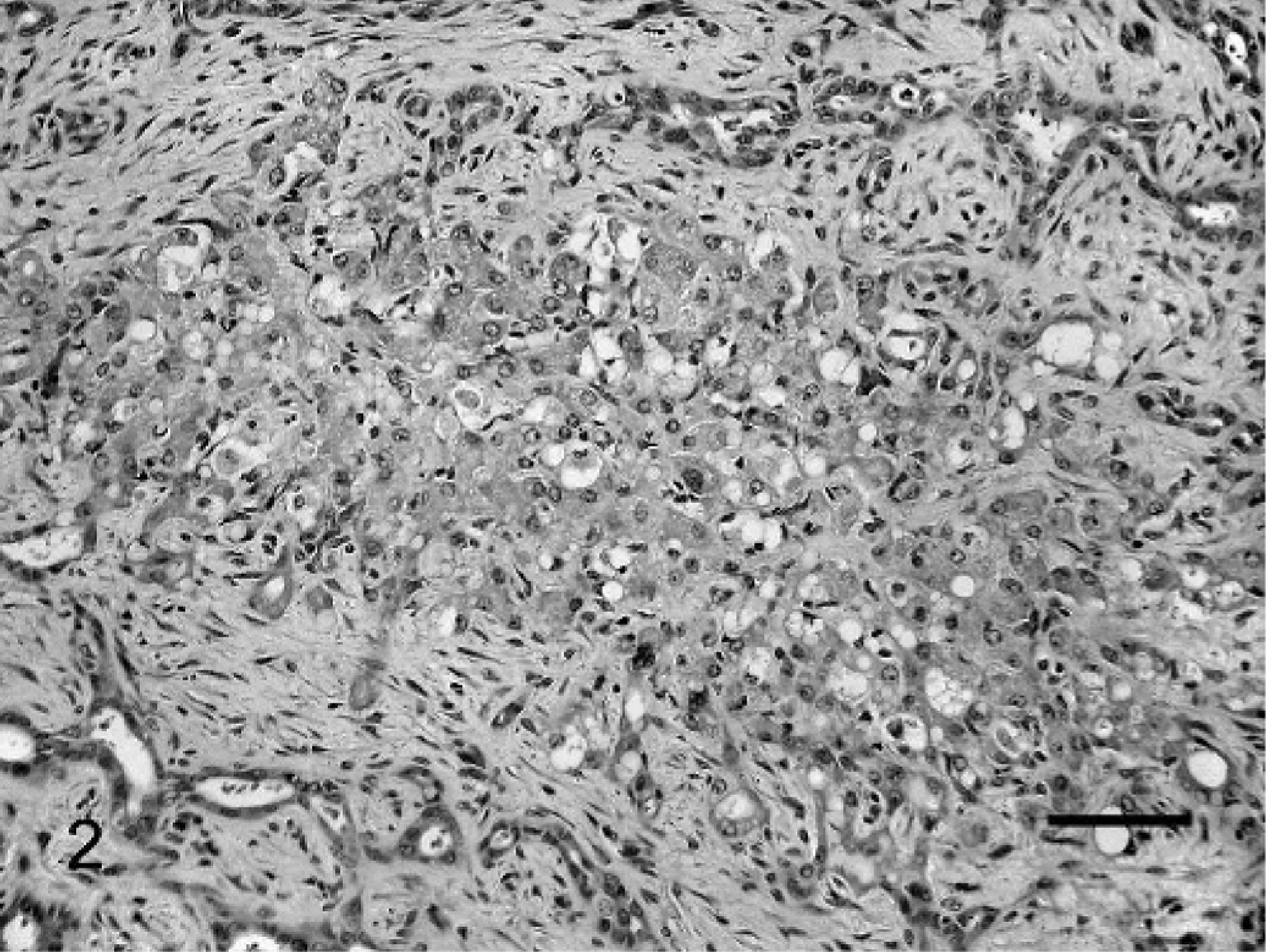
Liver; equine. Discrete islands of hepatocytes found throughout the more abnormal regions of the hamartoma, containing multiple clear cytoplasmic vacuoles. HE. Bar = 70 microns.
In the less severely affected areas, there were thick anastomosing septa of abnormal bile ducts and associated mesenchymal matrix, as described above. There were no normal portal tracts identified, because there were no normal bile ducts formed. The portal vein and the hepatic arteries could be identified as distinct structures enveloped in connective tissue. There were islands and sheets of normal-appearing hepatocytes, but there was no developed lobular architecture. Hepatocytes comprised approximately 50% of these areas, and the remainder was composed of the abnormal septa (Fig. 3). There was no evidence of inflammation, and no infectious agent was identified.
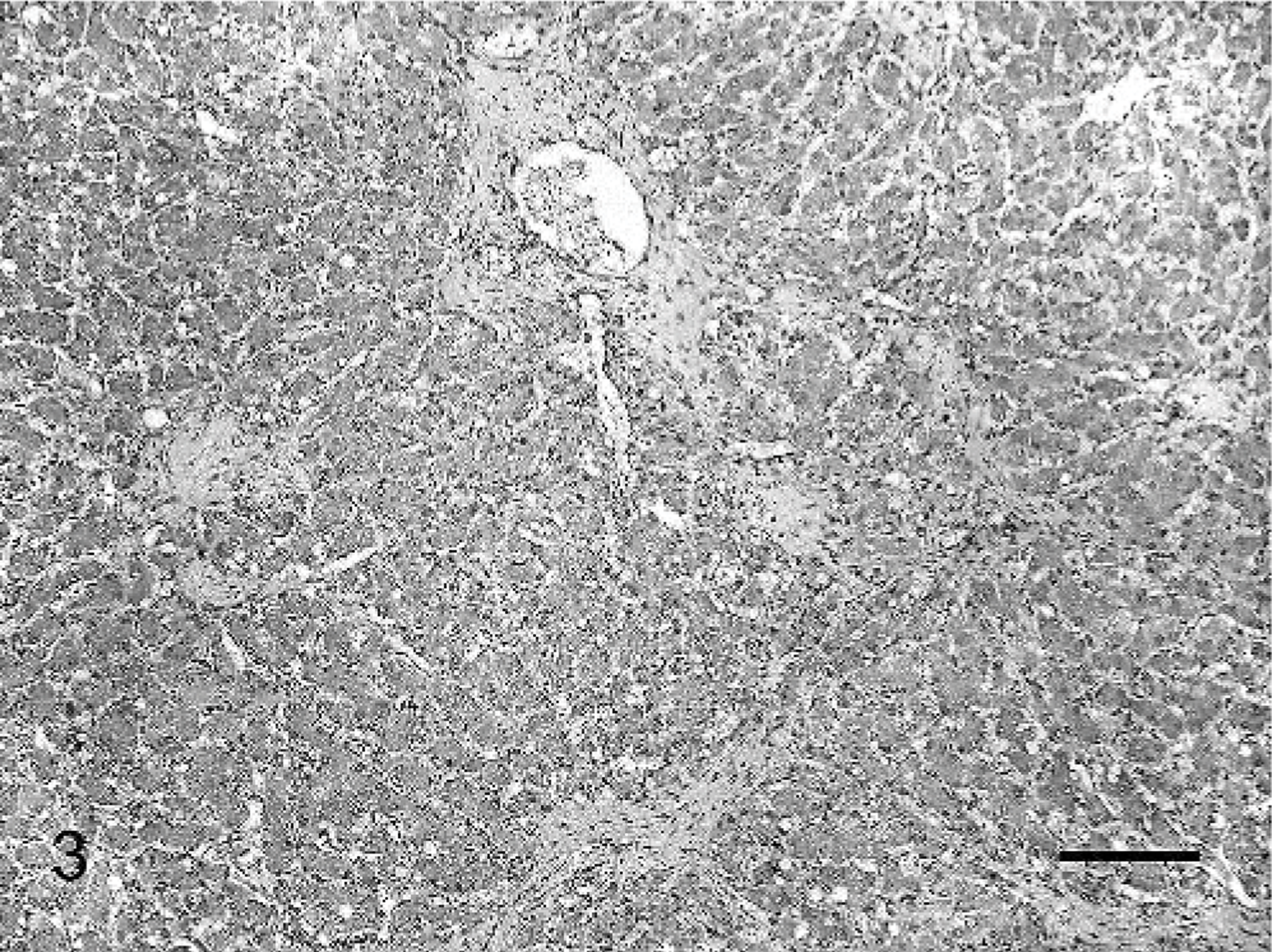
Liver; equine. Less affected areas of the hamartoma, containing more normal-appearing areas of hepatic parenchyma, comprising approximately 50% of the section. HE. Bar = 350 microns.
The large proportion of the liver in this case had lesions that resembled mesenchymal hamartoma, although in other smaller areas there were lesions similar to congenital hepatic fibrosis. Mesenchymal hamartomas are composed of a myxoid stroma with fibroblasts, bile ductules, vascular structures, and islands of hepatocytes. 7 Epithelial-lined and nonepithelial-lined cystic spaces may be present. It has been suggested that cyst expansion is largely responsible for postnatal tumor growth, which would explain the absence of cystic spaces in this case, because the animal died during the birth process. Congenital hepatic fibrosis is a rare heritable disorder of the intrahepatic bile ducts that is caused by a ductal-plate malformation. 2, 5 It is histologically characterized by variably thick septa of collagenous stroma that contains a proliferation of small-caliber bile ducts that bridge portal areas and is usually evident early in life because of impaired hepatic function or portal hypertension. 1 Congenital hepatic fibrosis is uncommon in animals, but has been reported in related Swiss Freiberger horses from Switzerland, as well as in cats, piglets, and calves. 1, 4, 8, 9 Congenital hepatic fibrosis is usually associated with polycystic kidney disease in humans, 3 and there were no renal lesions present in this equine fetus. Hepatic lesions can be present with or without renal pathology in both humans and animals, including the previous report of congenital hepatic fibrosis in Swiss Freiberger foals. 4
The extensive involvement of the liver, the marked increase in liver volume, and the loose alcian blue-positive myxoid stroma seen in this case is more similar to descriptions of mesenchymal hamartoma than the descriptions of congenital hepatic fibrosis. Ductal-plate malformation is responsible for the development of mesenchymal hamartoma and congenital hepatic fibrosis, which explains the similarities between each of the disorders. 2, 7
This is the first case report of mesenchymal hamartoma of the liver in the veterinary literature to our knowledge.
Footnotes
Acknowledgements
The authors would like to thank Sandra Horton for her assistance with special histochemical staining. The authors would also like to thank Valeer Desmet, MD, for a review of the case and helpful suggestions.