
Abstract
Mycobacterium haemophilum, a nontuberculous mycobacterium, is a pathogen in immunocompromised human patients. We report a case of M haemophilum-induced granuloma in the spinal cord of an American Bison (Bison bison). M haemophilum infection was diagnosed by sequencing a portion of the 16 S ribosomal DNA and comparing the amplicon sequence with sequences in GenBank.
A 16-year-old intact female American Bison (Bison bison) was observed with ataxia and hind limb paresis. The bison was euthanatized and submitted for necropsy. On gross examination, in the caudal lumbar region of the spinal cord there was a 1.5 cm × 1 cm, well-delineated, pale tan, firm intradural mass. The mass was located on the ventral aspect of the spinal cord, and it largely replaced and compressed the spinal cord in that region (Fig. 1). Segments of the spinal cord and the mass were fixed in 10% neutral buffered formalin for 24 hours. The fixed tissue was processed by routine methods for paraffin embedding, and 4-μm sections were stained with Ziehl-Neelsen staining and hematoxylin and eosin.
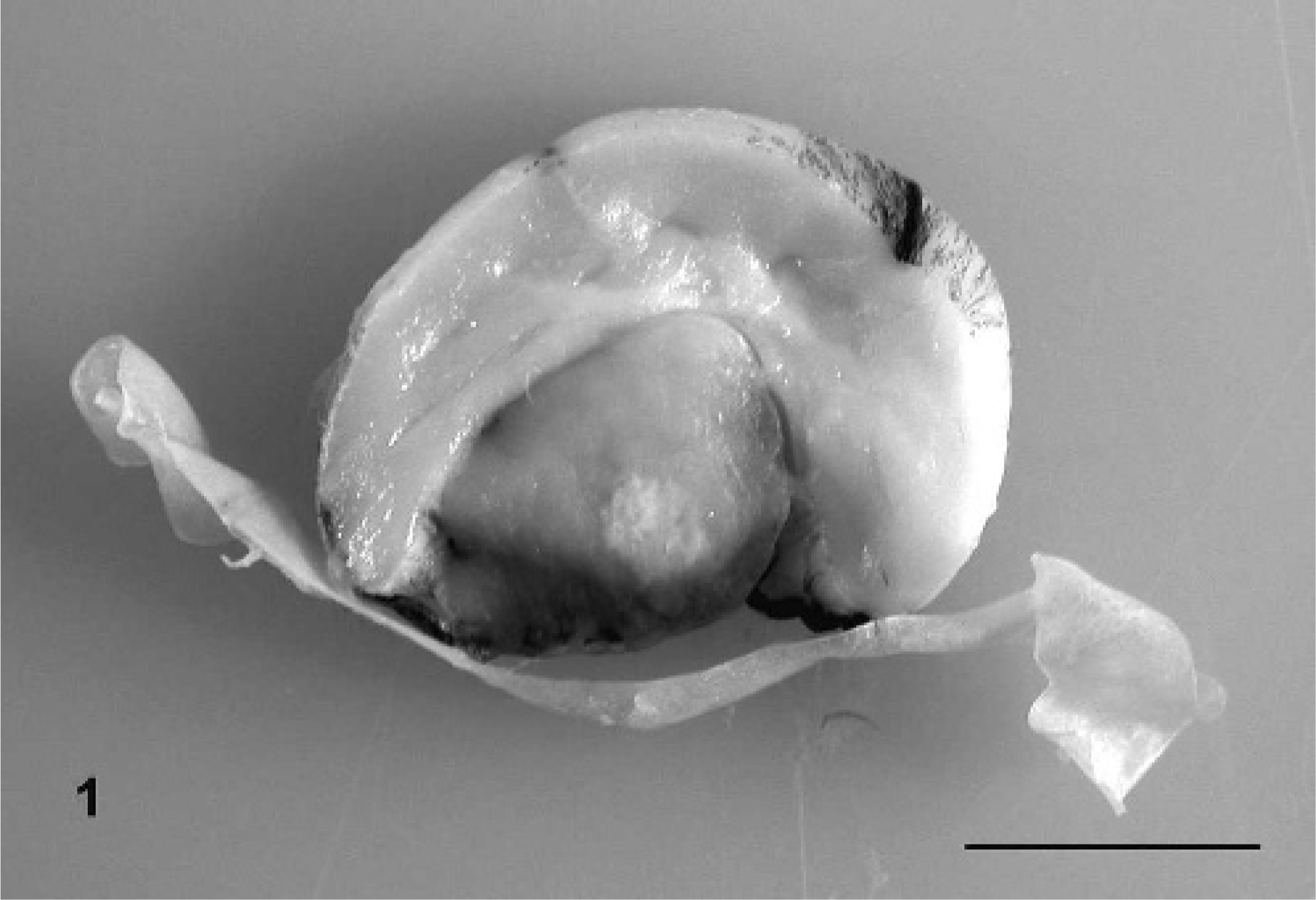
Cross-section of the lumbar spinal cord in a bison. A well-delineated and expansile intradural mass with severe compression of the spinal cord. Bar = 1 cm.
Microscopically, the spinal cord was compressed and replaced by a well-delineated, expansile, partially encapsulated granuloma. The granuloma was composed of sheets of epithelioid macrophages with interspersed neutrophils and lesser numbers of lymphocytes; the sheets surrounded a large central necrotic area with mineralization. The macrophages had distended cytoplasm containing myriad acid fast bacilli (Ziehl-Neelsen acid fast staining) (Fig. 2). The granuloma was surrounded by a thin fibrous capsule. The adjoining white matter of the spinal cord contained numerous blood vessels with prominent endothelial cells, dilated myelin sheaths, and swollen hypereosinophilic axons (axonal degeneration).
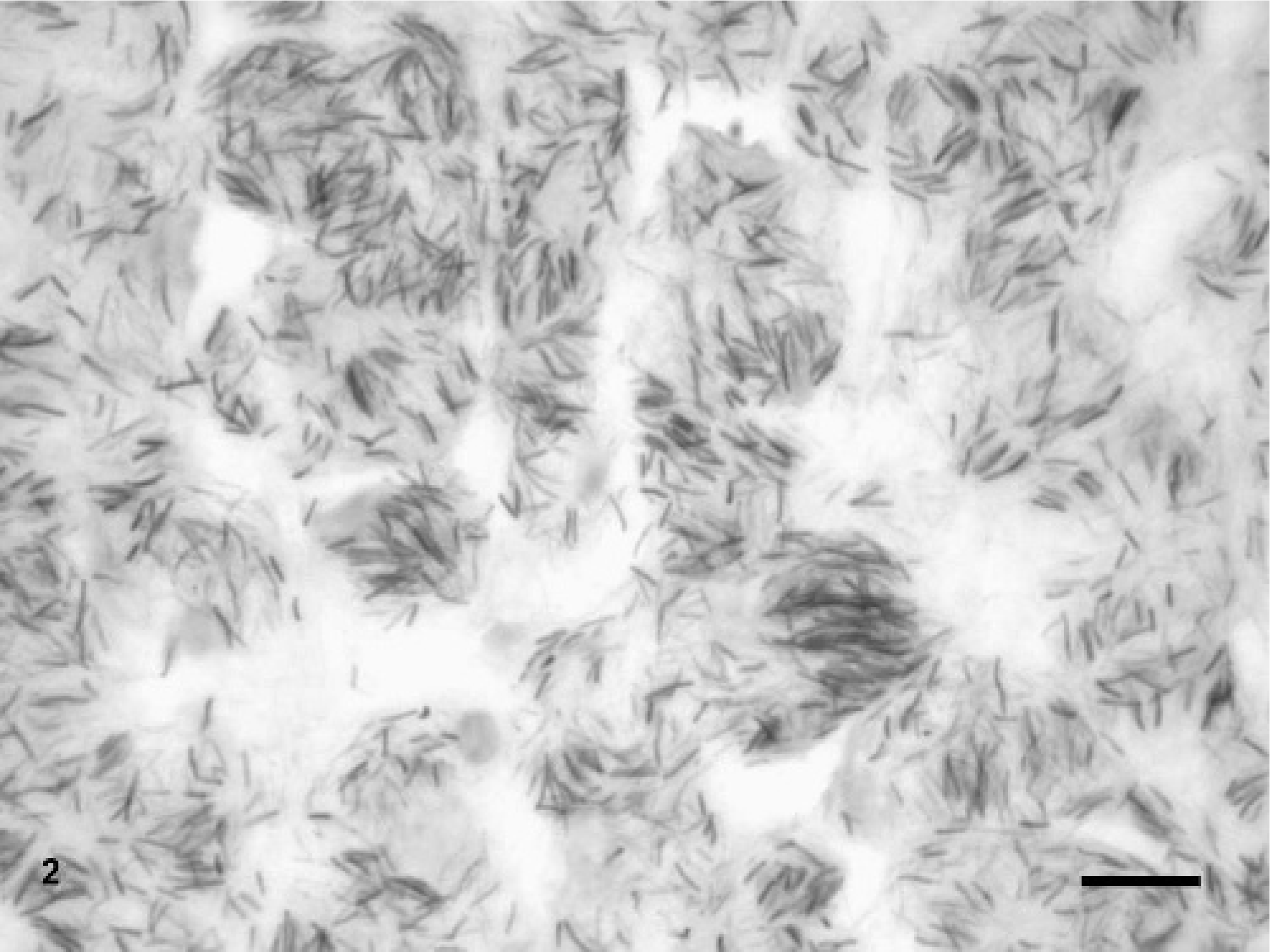
Lumbar spinal cord mass in a bison. Numerous acid-fast bacilli are present within epitheloid macrophages. Ziehl-Neelsen stain. Bar = 20 μm.
For polymerase chain reaction, five 10-micron sections were cut from a paraffin block containing the granulomatous spinal cord lesion that had been fixed in formalin for 24 hours. DNA was extracted from these cut sections using a commercial kit (Qiamp DNA Mini-kit; Qiagen) according to the manufacturer's instructions, with the following variations: a sterile, disposable plastic needle was used to scrape melted paraffin from the sides of the tube and mix it with the ATL lysis buffer after a few minutes at 60°C in the first step. After overnight incubation at 60°C with lysis buffer and 40 μl of 20 mg/ml proteinase K, the upper melted paraffin layer was removed as much as possible using a pipette tip. After the Buffer AL and ethanol steps, the tube was placed in a freezer at -20°C for 30 minutes. This caused the remaining wax to adhere to the sides of the tube so that the mixture could be pipetted into the Qiagen spin column without wax.
Initially, the extracted DNA from this block was used as a template for polymerase chain reaction (PCR) amplification using Mycobacterium avium complex-specific primers as previously described. 9 Extracted DNA from M avium–positive and M avium–negative blocks was used as a control. The bison sample was negative for M avium complex by this method.
Extracted DNA from the block then was amplified using Mycobacterium genus-specific 16 S rRNA primers as previously described. 4 The primers FO16 S (5′GATAAGCCTGGGAAACTGGGTC3′) and RO16 S (5′TTCTCCACCTACCGTCAATCCG3′) were used to amplify a 344-bp fragment of the 5′ region (nucleotides 134–477) of mycobacterial 16 S rRNA. The PCR conditions entailed 5 minutes of denaturing at 94°C, followed by 35 amplification cycles consisting of 1 minute of denaturing at 94°C, 1 minute of annealing at 58°C, and 1 minute of extension at 72°C, with a final extension cycle of 7 minutes at 72°C.
The PCR amplicon was visualized on a 1.5% agarose gel containing ethidium bromide, excised using a sterile scalpel blade under UV illumination, and purified using a Freeze ‘n’ Squeeze kit (BioRAD) according to the manufacturer's directions. The amplicon DNA was sequenced directly on both strands by Amplicon Express (Pullman, WA) using the Perkin Elmer Applied Biosystems Prism Dye Terminator Kit, with analysis on an ABI 373 DNA Sequencer. Forward and reverse sequences were aligned using a Clustal W program online. 14 GenBank search for similarities was then accomplished using the NCBI BLAST program online. 8
The closest sequence identity was a >99% (343/344 bp) match with Mycobacterium haemophilum (GenBank accession numbers AF547932.1, AY215264.1, X88923.1, and U06638.1) The most closely related (337/344 bp or less) were members of the M avium complex: Mycobacterium kansasii, Mycobacterium visibilis, and Mycobacterium szulgai. The sequence was quite significantly different from Mycobacterium tuberculosis (331/344 bp identity).
M haemophilum is a nontuberculous mycobacterium that causes lymphadenitis in children, as well as skin, bone, joint, and pulmonary infections in immunocompromised adult humans. 7, 10 The organism first was isolated from subcutaneous abscesses in a human patient with Hodgkin disease, and, more recently, infections have been diagnosed in human patients with AIDS or organ transplants. 7, 12 M haemophilum is a fastidious organism that is slow growing, requires heme-supplemented culture media, and grows optimally at 30°C to 32°C, as opposed to 37°C, which is the optimum temperature for most other pathogenic mycobacteria. 11 These cultural requirements could lead to underdiagnoses if routine mycobacterial isolation techniques alone are relied upon. Very few incidents of M haemophilum infection in animals have been reported; incidents include a case of pulmonary mycobacteriosis in a royal python, 5 zebrafish infections, 6 and experimentally infected immunosuppressed mice. 1
M haemophilum infection was confirmed directly from fixed tissues because these were the only samples available. Since this species cannot be cultivated on routine mycobacterial culture media, PCR with DNA sequencing is a reliable alternative. PCR can reduce the turnaround time for mycobacterial diagnosis, and the risk of zoonotic infection is reduced when formalinized tissue is used.
Mycobacterium bovis and Mycobacterium avium paratuberculosis have been reported as endemic infections in bison. 2, 13 Mycobacterium avium paratuberculosis infection in this case seemed unlikely, since infection with this organism in bison is reported to involve only the intestinal tract and mesenteric lymph nodes. 2 Infection with M bovis would be more likely to involve extraintestinal tissues. Bison infected with M bovis have tuberculous lesions that usually are confined to lymph nodes of the head and neck, pulmonary involvement, and, occasionally, generalized tuberculosis involving thoracic and abdominal viscera. 13 The main diagnostic priority for this animal was to rule out infection with mycobacteria of the M tuberculosis complex for herd and public health reasons. 3 This was accomplished quickly by confirming a negative result by PCR using M tuberculosis complex–specific primers. Sequencing was desirable in order to establish the species identity and to corroborate the negative M tuberculosis complex PCR result. M haemophilum was an interesting finding, since it is not often found in animals and is likely due to an immunocompromised status in this bison.