
Abstract
Feline physeal dysplasia typically presents as unilateral or bilateral, atraumatic, slipped capital femoral epiphysis. The femoral physeal lesion consists of retention of a cartilaginous physis beyond the expected age of closure, with disorganization of the chondrocytes and subsequent slippage. in this article, we describe two cats with feline physeal dysplasia and slipped capital femoral epiphysis that died of unrelated causes (cardiomyopathy and lymphosarcoma). At necropsy, additional sites were found to have retained physes with similar abnormal arrangement of chondrocytes. This confirms that physeal dysplasia in cats is a widespread multicentric disorder of chondrocytes that precedes the development of slipped capital femoral epiphysis.
Feline physeal dysplasia is a condition of young, predominantly male, frequently overweight cats, in which one or both femoral heads atraumatically separates from the femoral neck along an abnormal physis. 3, 5, 6, 9 Histologic examination of the surgically removed femoral head confirms the diagnosis by demonstrating retained physeal cartilage with irregular clusters of chondrocytes. 3 However, because this condition is not fatal, the histopathology of the other physes in affected cats has not been described. In this article, we demonstrate that the retention of an open physis and the disorganization of the chondrocytes is a widespread, multicentric lesion that precedes the atraumatic separation.
Cat No. 1 was a 4-year-old, 5.6-kg, neutered male, domestic shorthair cat that presented to a local veterinarian with a sudden onset of nonweight-bearing lameness in the left front limb and a greater than 1-year history of lameness in the left hind limb.
Pelvic radiographs showed evidence of degenerative joint disease in both coxofemoral joints and suspected bilateral, nonhealing fractures of the femoral necks. The cause of the left front limb lameness could not be identified. The owner elected conservative treatment with prednisone, and the cat initially improved. However, the left front limb lameness continued to recur.
Approximately 1 month later, the cat presented to the local veterinarian after suspected electrocution. The owner reported that the cat became acutely paraparetic/paraplegic, very agitated and painful, and then bit through an electrical cord. Thoracic radiographs revealed an enlarged heart and pulmonary edema. The owners elected euthanasia. The postmortem diagnosis was left ventricular endocardial fibrosis 13 with multiple mural and iliac thrombi. A 3-cm-long piece of plastic-coated electric cord was present in the stomach.
At necropsy, the left femoral head was separated from the neck and was attached by a fibrous connective tissue band to the trochanteric fossa. There was a line of separation along the physis of the right femoral head but little displacement (Fig. 1). Sections of the proximal and distal femur, tibia, radius, and proximal humerus were examined histologically. Both femoral heads were separated through the physis with bony and fibrous proliferation along the joint margins. The chondrocytes on either side of the fracture were in irregular clusters separated by an extensive extracellular matrix. Chondrocytes within these clusters were similar in size and shape to those of the reserve zone. The articular cartilage of both femoral heads was fibrillated with multifocal erosions. The proximal humeral physis was still present and was up to 1.5 mm thick (Fig. 2). Chondrocytes were arranged in similar irregular clusters and were separated by an abundant matrix (Fig. 3). The distal humerus, tibia, radius, and distal femur were within normal limits for a 4-year-old cat, with no cartilaginous physis.
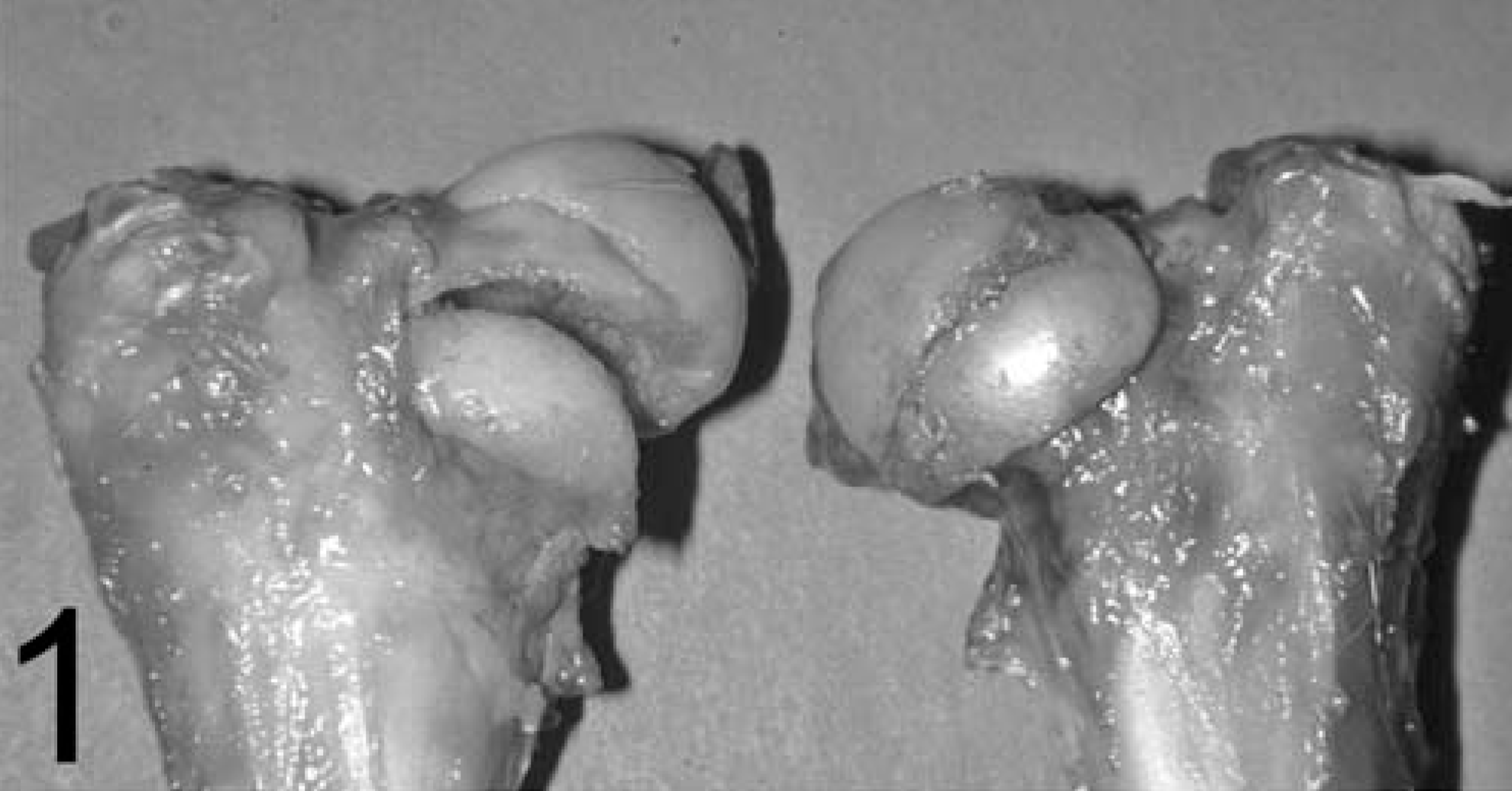
Femoral heads; cat No. 1. Note the separation of the left femoral capital epiphysis through the physis. There is a line of separation but little displacement of the right femoral capital epiphysis.
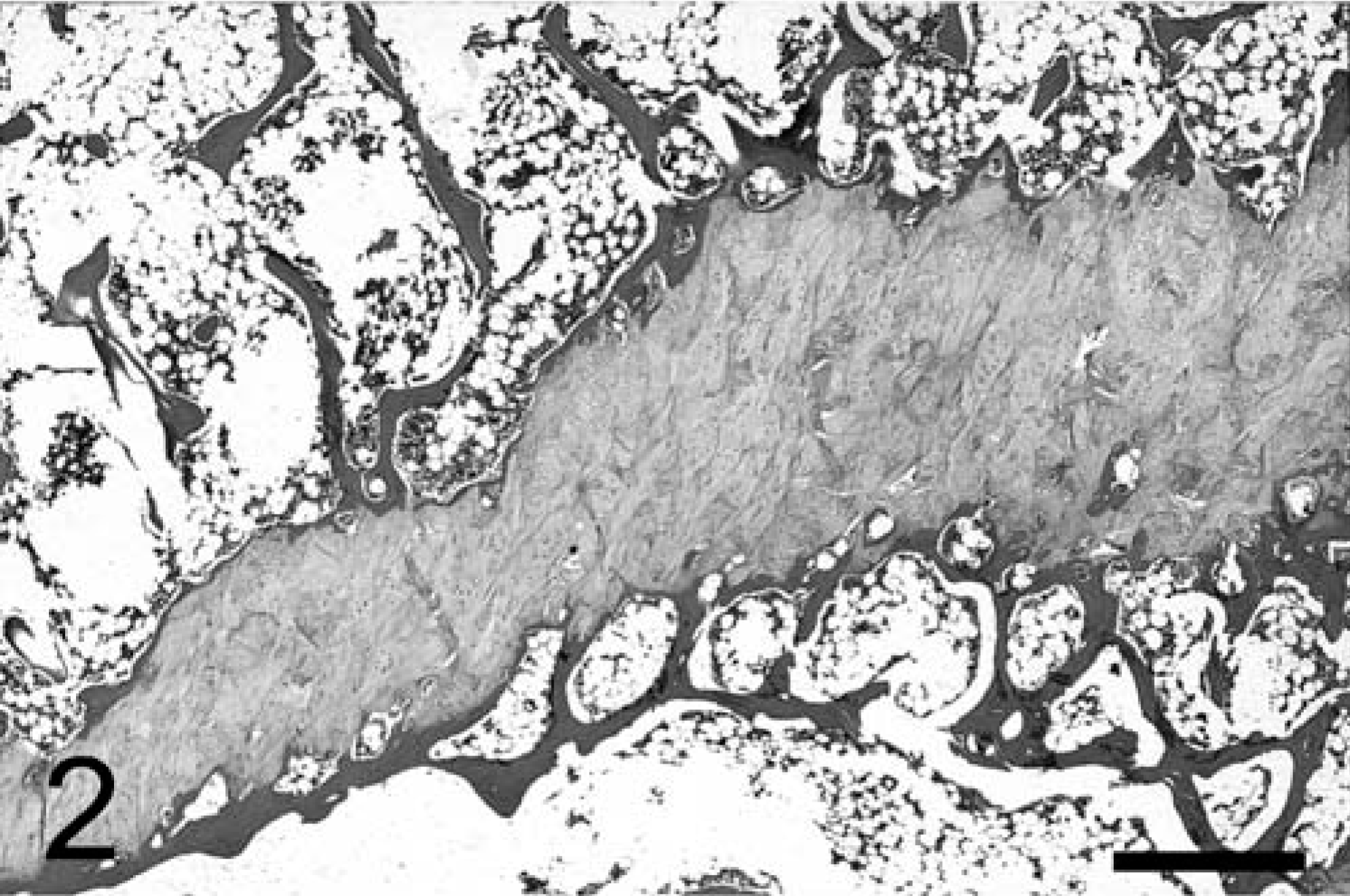
Proximal humerus; cat No. 1. There is an irregular cartilaginous (open) physis present. HE. Bar = 1,000 µm.
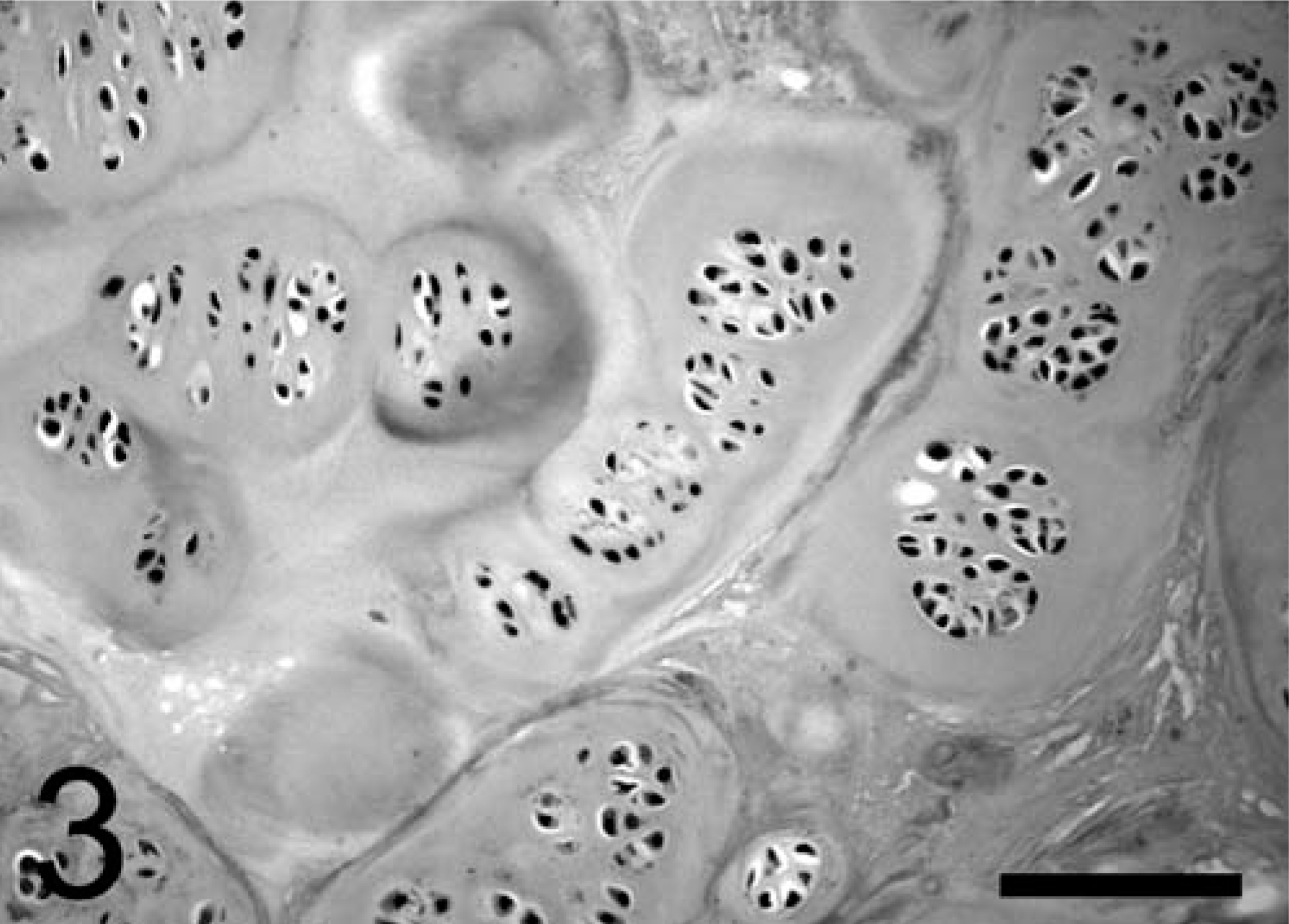
Proximal humeral physis; cat No. 1. Chondrocytes are arranged in irregular clusters separated by an abundant extracellular matrix. HE. Bar = 100 µm.
Cat No. 2 was an adult, 3.6-kg, neutered male, domestic shorthair cat, which presented to the Veterinary Hospital of the University of Pennsylvania Emergency Service with an approximately 1- to 2-week history of lethargy and anorexia. Although the exact age of the cat was unknown, it had been adopted as an adult and kept for at least 1.5 years by the owner. Clinical findings included icterus, hyperthermia (105.2°F), and severe anemia (hematocrit 12%). The owner elected euthanasia. Lymphosarcoma was the postmortem diagnosis.
At necropsy, the left femoral head was partially separated from the metaphysis with a small band of fibrous tissue bridging the epiphysis and the trochanteric fossa. The right femoral head was intact with a prominent femoral physis along the craniolateral aspect of the femoral head. A longitudinal section through the right femur demonstrated a grossly visible distal femoral physis. The proximal and distal portions of both femurs and humeri were examined histologically. The left proximal femur demonstrated similar physeal changes to those seen in the proximal femoral heads of cat No. 1, consistent with physeal dysplasia and slipped capital femoral epiphysis. The right proximal and distal femoral physes were also present and showed similar changes to those seen in the humerus of cat No. 1, consistent with physeal dysplasia. There was no evidence of slippage of the right femoral epiphysis. The proximal and distal humeri and right distal femur were within normal limits for an adult cat, with no detectable physis.
The clinical, radiographic, and pathologic features of feline physeal dysplasia with slipped capital epiphysis are well-described. 3, 5, 6, 9 In all reports, the majority of cats are young (but beyond the age of proximal femoral physeal closure, 34 to 44 weeks 12 ), predominantly male, and often overweight. The cats rarely have any history of trauma. These findings are similar to the human syndrome of slipped capital femoral epiphysis (SCFE), which is also typically atraumatic and shows a propensity for overweight male adolescents. Although early gonadectomy slightly delays physeal closure, 11 several findings argue against the role of neutering in the development of feline physeal dysplasia. The first is the occurrence of the lesion in intact male and female cats. 3, 5 Although these are a minority, the large number of neutered males may represent the preponderance of neutered cats in the indoor pet cat population, combined with a true male predisposition. The second factor is the age of the affected animals. Most are well beyond the age of physeal closure (proximal femur 34–44 weeks, proximal humerus 52–62 weeks, distal femur 54–76 weeks). 10– 12 For example, one cat in this report was 4 years old. The third factor is the similarity of the feline condition to that in humans, 1, 2, 8 a species in which prepubertal gonadectomy is rarely performed.
The histopathologic findings reported for humans and cats are remarkably similar. 1 Both demonstrate an overly wide physis; in cats, the width is more than twice that of the normal cat physis. 3 Normal linear chondrocyte arrangement is replaced by irregular chondrocyte islands embedded in an abundant extracellular matrix. The cleavage line and site of slippage is typically in the center of the physis and surrounded by a zone of chondronecrosis. In some cases, there is granulation tissue and early callus formation surrounding the fracture site. 3
A similar condition has been described in two young, overweight, neutered male Shetland sheepdogs. 4 Both had a chronic history of severe hindlimb lameness and no known history of trauma. Bilateral femoral head and neck excision in both of these dogs revealed separation of the femoral capital epiphyses. The histopathologic findings were similar to those presented above and are distinctly different from those reported with traumatic physeal fracture (Salter-Harris type I), in which the normal columnar arrangement of chondrocytes on either side of the fracture remains. 7
A radiographic study of physeal fractures in adult cats reported the presence of multiple open growth plates (distal femoral, proximal tibial) in cats with slipped capital femoral epiphysis. 10 In the two cats in this study, we confirm those findings and report an abnormal arrangement of chondrocytes within all of the open physes. This confirms that the dysplasia affects multiple physes, and that the abnormal arrangement of chondrocytes in the fractured capital femoral physis is present before slippage. Therefore, the histologic changes are not a reaction to the epiphyseal separation. The open humeral physis in cat No. 1 is unlikely to have been the cause of the left forelimb lameness because it should not have been painful without separation or slippage. We theorize that lameness in this cat may have instead been related to the cardiomyopathy causing intermittent thromboemboli and ischemia.
This article presents two cases of slipped capital femoral epiphysis in cats with concurrent distal femoral and humeral physeal dysplasia. Radiographic, gross necropsy, and histopathologic findings are all comparable to those previously reported for slipped capital femoral epiphysis in cats and with the findings in humans with SCFE. The documentation of concurrent of distal femoral and humeral physeal dysplasia and the presence of capital femoral physeal dysplasia without slippage confirms that slippage of the capital femoral epiphysis in cats is secondary to an underlying physeal dysplasia.