
Abstract
An adult, captive-born female capybara died of systemic thrombosis and hemoperitoneum associated with placental subinvolution. Grossly, the uterus was enlarged, segmentally thickened, and associated with a large blood clot in the abdominal cavity. There was hemometra and a large ovoid mass in each uterine horn weakly adhered to the endometrium, and the right uterine horn wall had a small perforation over the mass. The mesometrial veins were markedly dilated due to thrombosis and occasionally perforated. Histologically, the uterine masses consisted of partly necrotic placental and subplacental tissue. The uterine wall surrounding the masses had full-thickness coagulative necrosis of the myometrium and diffuse endometrial ulceration with abundant syncytiotrophoblast-like cells within capillaries. Vascular lesions in the uterus and mesometrium consisted of mural invasion by cytotrophoblast and syncytiotrophoblast-like cells, thrombosis, fibrinoid necrosis, and/or heterophilic vasculitis. This is the first report of placental subinvolution in capybaras or any rodent species, to the authors' knowledge.
Placental subinvolution has been described in the bitch and is characterized by longer than normal persistence and deeper than normal penetration of trophoblast-like cells in the uterine wall, with vaginal bleeding that lasts for weeks or months after parturition. 1 Subinvolution of the uteroplacental arteries in the human placental bed with perivascular and intravascular trophoblasts is also an important cause of postpartum bleeding in women. 3, 4 This report describes sub-involution of placental sites in a captive capybara (Hydrochaeris hydrochaeris) complicated with systemic thrombosis and hemoperitoneum.
An adult, captive-born female capybara presented with lethargy shortly before death. Keepers indicated she had bred over 1 year before presentation. The capybara herd at Africam Safari (Puebla, México), with more than 40 animals at the time of presentation of this female, is housed with South American camelids and a variety of ruminants in a 10-acre outdoor enclosure at the wild-animal park. At necropsy, this capybara was in an adequate body condition and had mild icterus. There was a large blood clot just ventral to the uterine horns (Fig. 1). The uterus was markedly enlarged (Fig. 1), similar to a control pregnant capybara that died of trauma. The wall of both uterine horns was diffusely and trans-murally reddened and had segmental thickening with prominent longitudinal folds (Fig. 1), unlike the control uterus, which was thinner and without folds. The uterine and vaginal lumen contained a moderate amount of bloody exudate (Fig. 2). The right and left uterine horns each had a mass in the lumen weakly adhered to the endometrium, 8 × 6 × 4 cm and 5 × 3.5 × 3 cm, respectively (Fig. 2). Both masses were friable, red to brownish, and oozed a reddish exudate on the cut surfaces; the mass in the left uterine horn had a well-circumscribed whitish tissue band of medium consistency at the attachment site. The uterine horn walls surrounding these masses were thinner than normal and lacked the longitudinal folds found in the adjacent thickened uterine wall (Fig. 1). There was a perforation less than 1 mm in diameter in the wall of the right horn overlying the mass. The mesometrial veins were markedly dilated by thrombi and tortuous, especially at the uterine border (Fig. 3); few of the affected veins had perforations less than 1 mm in diameter. These uterine and mesometrial lesions were most severe in the right uterine horn. There were numerous cyst-like structures filled with clear fluid, up to 1 cm in diameter, in the serosal surface of the left uterine horn (Figs. 1 and 2). Urine was reddish. Other gross findings consisted of severe right-sided dilated cardiomyopathy, mild hydropericardium, mild gastric luminal hemorrhage, red discoloration of intestinal contents in the jejunum and ileum, and right persistent pupillary membrane with diffuse cataracts. A postmortem urinalysis revealed hematuria (10–12 red blood cells/hpf), pyuria (15–20 white blood cells/hpf), severe bacteruria, proteinuria (3+ reaction), bilirubinuria, hemoglobinuria, and numerous amorphous and triple phosphate crystals. Aerobic culture of the liver yielded a light growth of Klebsiella sp.
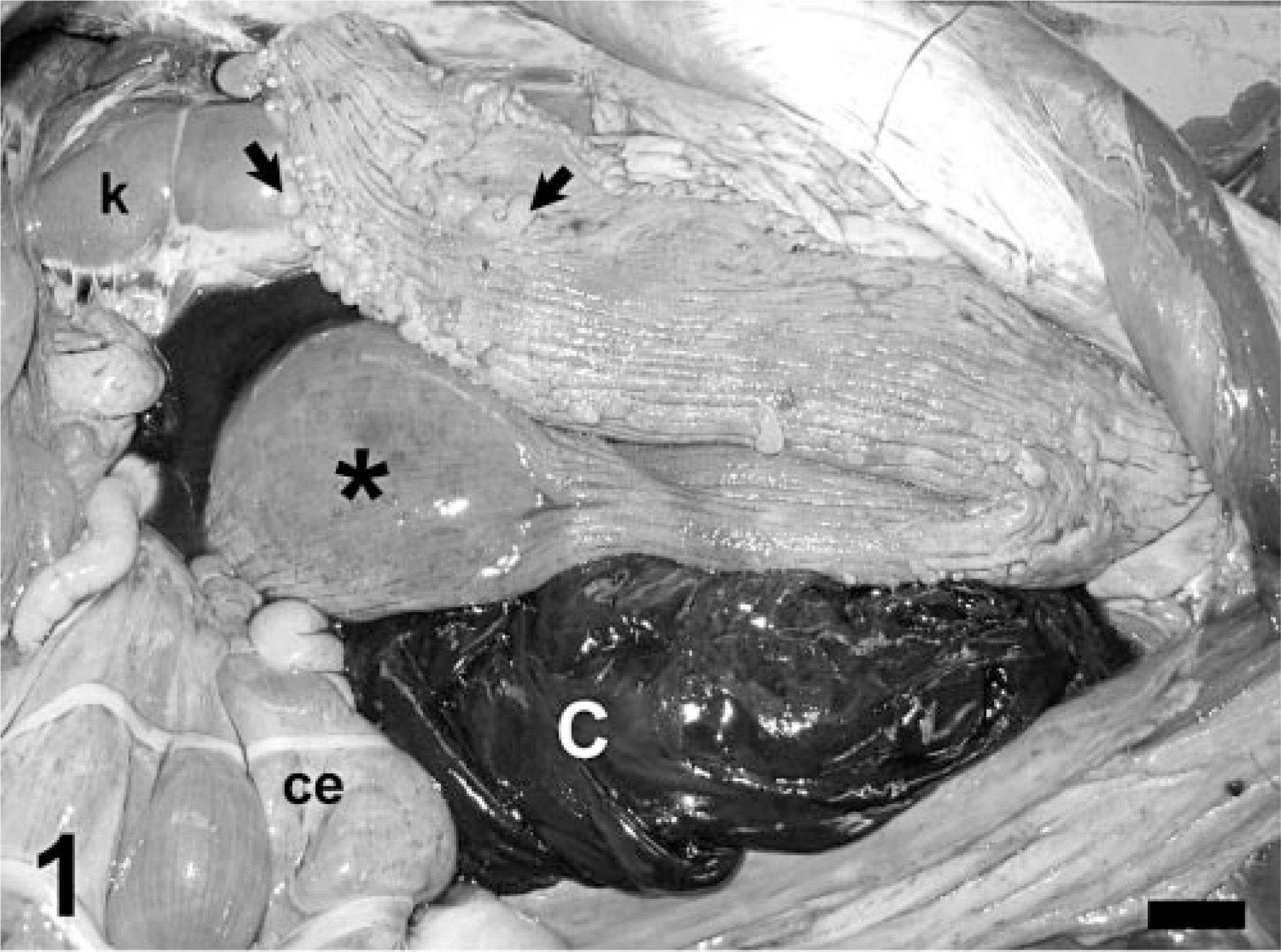
Abdominal cavity; capybara. Note the presence of a large blood clot (c) just ventral to the right uterine horn. The uterus is thickened with prominent longitudinal folds, but there is segmental thinning of the right uterine horn (asterisk), and cystlike lesions in the uterine serosal surface (arrows), interpreted as remnants of the Mullerian ducts. Ce = cecum, k = kidney. Bar = 2 cm.
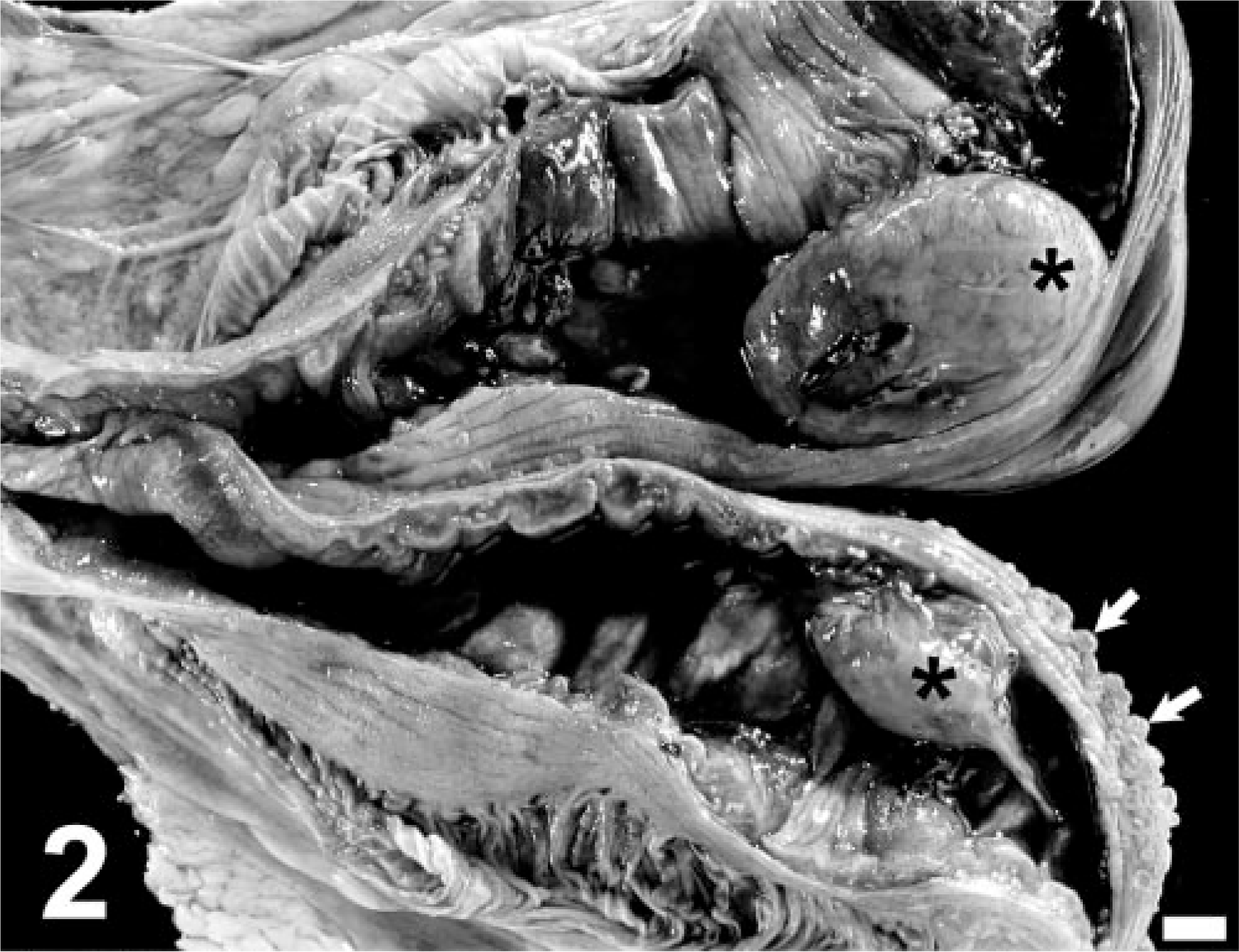
Uterus; capybara. Note the presence of fluid (un-clotted blood) in the lumen of the uterus, as well as two ovoid masses (asterisks), one in each uterine horn, corresponding to subinvoluted placentae. The uterine wall is thickened, except in areas surrounding the masses, and its serosal surface contains cystlike lesions, interpreted as remnants of Mullerian ducts (arrows). Bar = 1 cm.
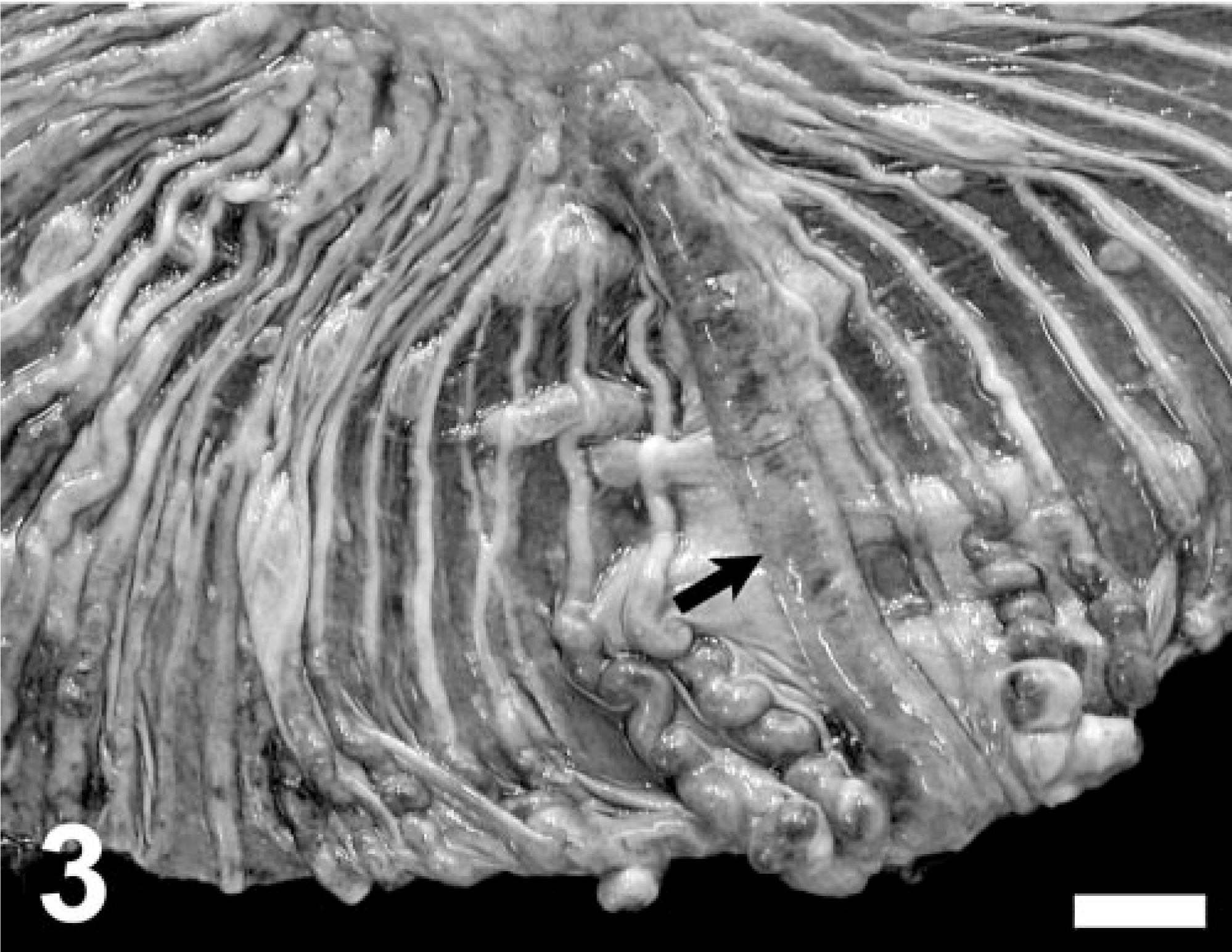
Mesometrium; capybara. Note segmentally or diffusely (arrow) dilated and tortuous mesometrial veins. Bar = 1 cm.
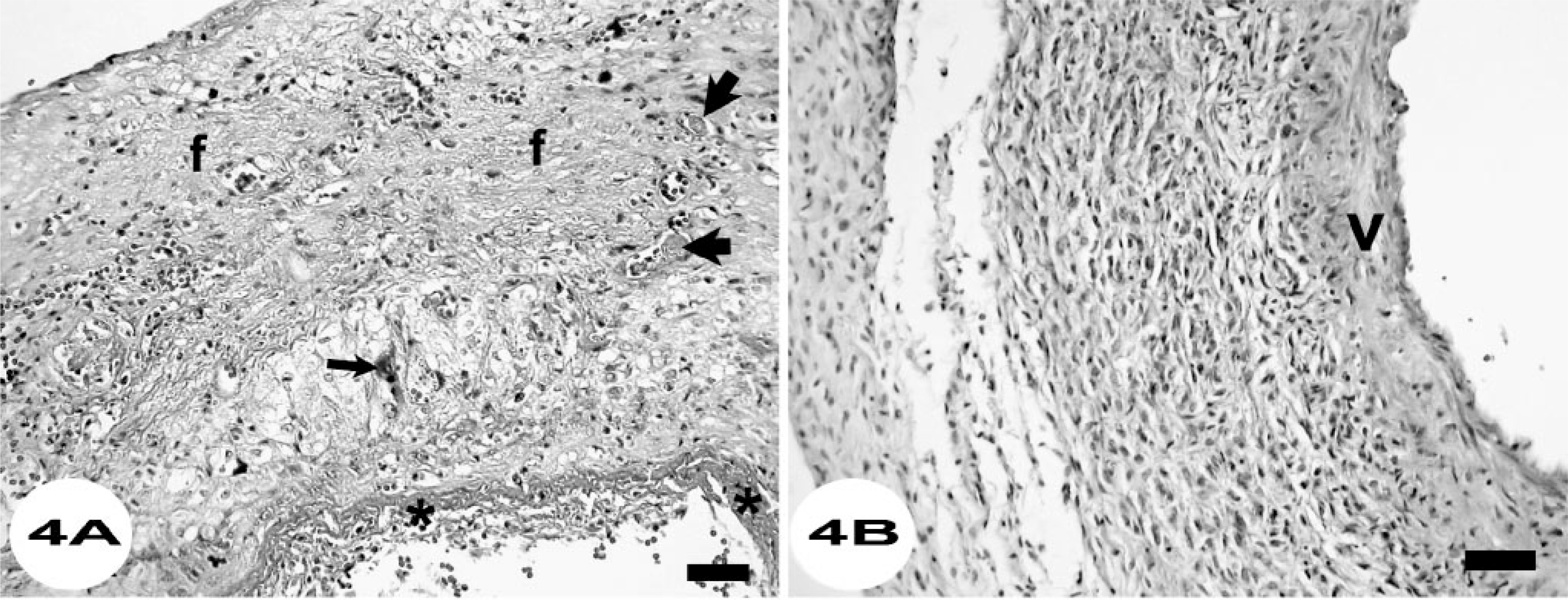
Histologically, the larger uterine mass consisted of almost completely necrotic tissue with islands of cytotrophoblast-like cells palisading around vessels and multifocal mineralization and chronic hemorrhage; the viable areas were similar to subplacental tissue. 5 The smaller uterine mass consisted of well-differentiated placental tissue with large areas of coagulative and lytic necrosis, thrombosis, multifocal mineralization, and occasional foci of chronic hemorrhage. The mesometrial vein lesions consisted of severe thrombosis with transmural, segmental, or diffuse fibrinoid necrosis (Fig. 4a) and heterophilic vasculitis; these veins were surrounded by palisades of cells with vacuolated cytoplasm and usually round to oval vesicular nuclei. In the most severely affected veins, necrosis extended into the adjacent mesometrial tissue, where it was accompanied by acute hemorrhage, fibrin deposition, and multifocal loss of the mesothelial lining. Cytotrophoblast- and syncytiotrophoblast-like cells were observed in the wall of mesometrial veins (Fig. 4a) and mesometrial connective tissue, unlike a control pregnant capybara used for comparison (Fig. 4b). The mesometrium was infiltrated diffusely by moderate numbers of heterophils. Occasional veins had moderate segmental medial hypertrophy. Throughout the wall of the uterus, similar lesions were seen in veins and arteries, but cyto- and syncytiotrophoblast-like cells were more numerous. Large syncytiotrophoblast-like cells invaded the lumen of capillaries, most frequently in sections close to the masses described grossly, and were often necrotic. In these areas, there was multifocal to diffuse, coagulative, and lytic necrosis of the myometrium with thrombosis and multifocal acute hemorrhage (Fig. 5); necrosis often extended into the uterine serosal surface. The endometrium overlying these necrotizing lesions was diffusely ulcerated, infiltrated with trophoblast-like cells and heterophils and suffused with extravasated erythrocytes. These lesions decreased in severity in sections more distant to the masses described grossly, in which myometrial necrosis was minimal and trophoblast-like cells were less frequently found within capillaries of the uterine wall (Fig. 6). In areas with minimal necrosis, the myometrium was multifocally infiltrated with macrophages, heterophils, and lymphocytes and was suffused with extravasated erythrocytes and proteinaceous fluid. The endometrium in these sections had occasional erosions and small ulcers, thrombosis of small vessels, moderate cystic dilatation of endometrial glands, and low numbers of cyto- and syncytiotrophoblast-like cells. The uterine serosal surface was also infiltrated multifocally with trophoblast-like cells. The cysts described grossly in the left uterine horn wall were lined by a single layer of flattened cells, occasionally had eosinophilic acellular contents, and were present in the serosal surface, with a few extending into the adjacent myometrium. Numerous capillaries and small vessels in the spleen, intestine, and lungs had fibrin thrombi. Other remarkable microscopic findings included moderate to severe lymphoplasmacytic anterior uveitis with cataracts, moderate acute intralobular hemorrhage in the pancreas, and mild centroacinar hepatocellular lipidosis.
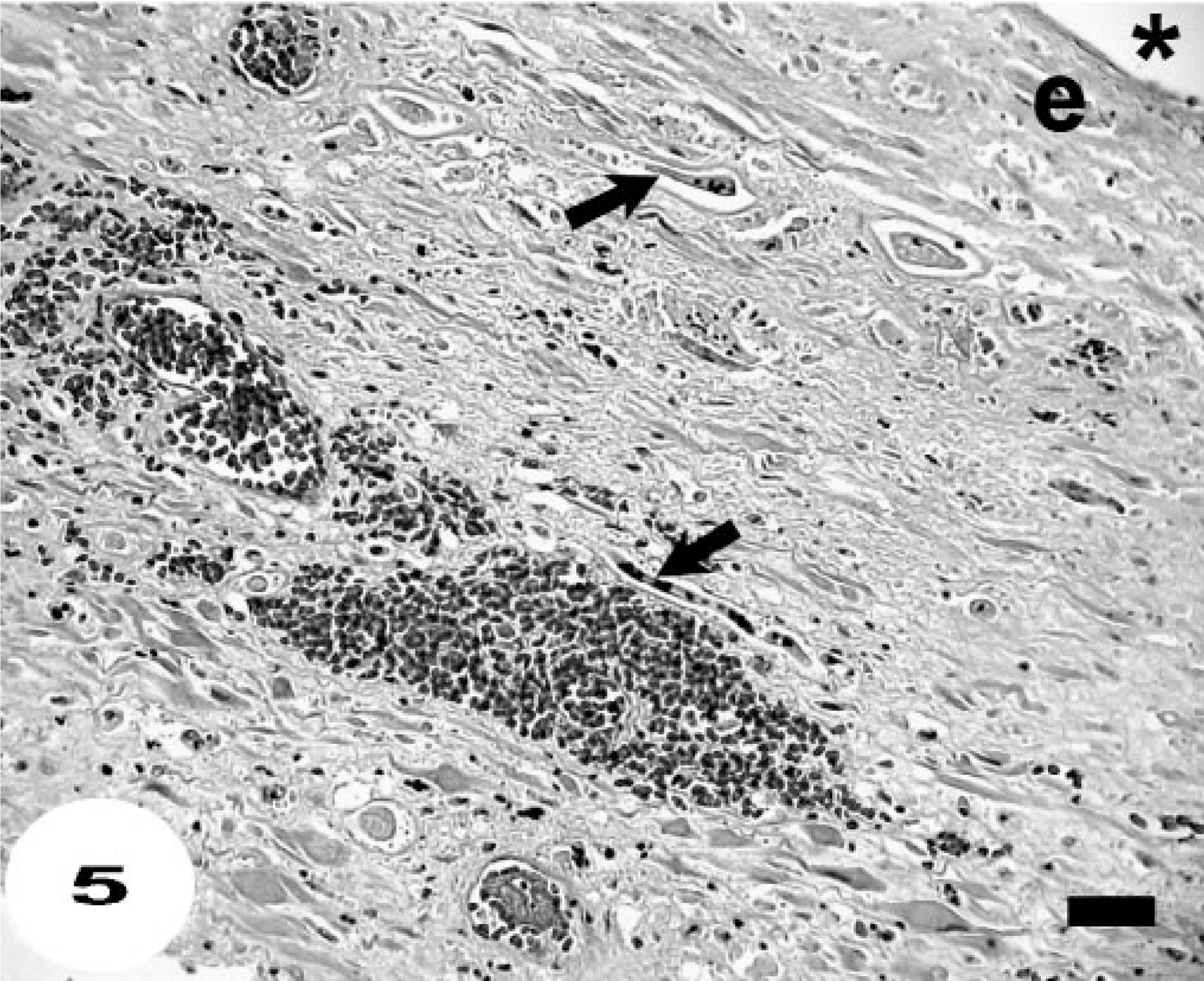
Uterine horn; capybara. Note diffuse coagulative and lytic necrosis of the myometrium associated with syncytiotrophoblast-like cells (arrows) within structures interpreted as necrotic capillaries, hemorrhage, and thrombosis. The overlying endometrium is necrotic and ulcerated. ∗ = uterine lumen. HE. Bar = 70 μm.
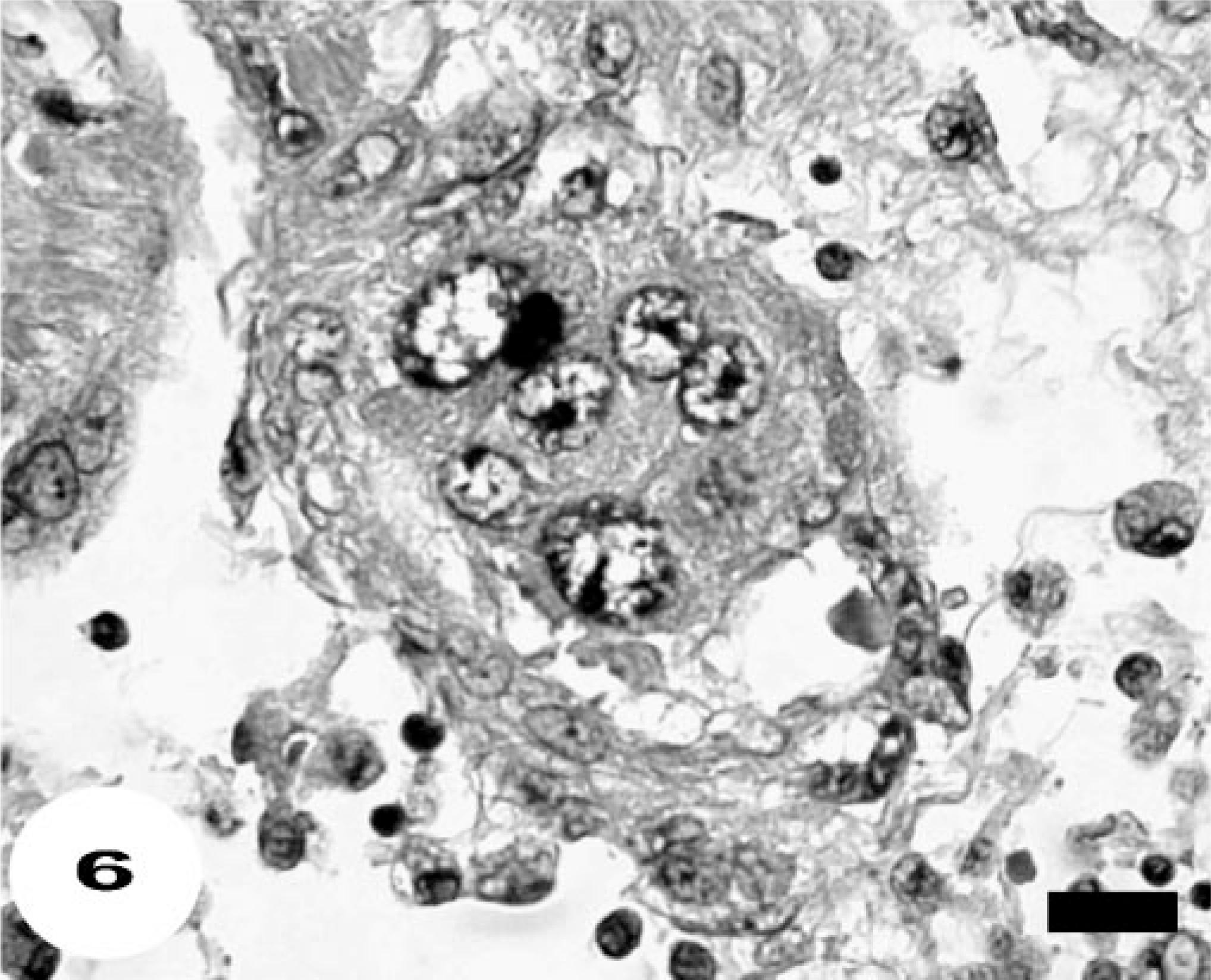
Myometrium; capybara. Note the presence of a syncytiotrophoblast-like cell invading the wall and lumen of a capillary with endothelial hypertrophy and perivascular infiltrates of macrophages, heterophils, and lymphocytes. HE. Bar = 20 μm.
The pathologic findings in this capybara are consistent with placental subinvolution. Based on microscopic evidence of thrombosis in several tissues, death was attributed to probable disseminated intravascular coagulation, likely precipitated in part by massive invasion of vessels by syncytiotrophoblast-like cells and marked widespread vascular lesions. The small perforations in the periplacental necrotic uterine wall and mesometrial veins likely caused hemoperitoneum because the large blood clot was closely associated with the uterine horns. The light growth of Klebsiella sp. obtained from the liver suggests that terminal bacteremia is a possible factor contributing to the death of this capybara, and the necrotic uterine wall may be a likely source of this process. If present, bacteremia may have contributed to systemic thrombosis.
There was no invasion of the endometrium by the masses grossly and they were attached weakly to the endometrium, similar to normal capybara placentae. Extensive myometrial necrosis with endometrial ulceration of the uterine wall surrounding the subinvoluted placental sites was attributed to ischemia due to the vascular lesions. The mass in the left uterine horn was consistent histologically with partly necrotic, well-differentiated placental tissue; 5 as compared with a normal capybara placenta, it was similar in shape and slightly smaller, and had a similar band of whitish tissue at the attachment site. The mass in the right uterine horn was mostly necrotic and similar in shape but larger in size to a normal capybara placenta; in viable areas, it was histologically similar to subplacental tissue. 5 A control gravid uterus from a capybara that died of trauma had discoid placentae in the range 6.5–7 × 6.5–7 × 4–4.5 cm in size for fetuses weighing 130–140 g; the placentae were weakly adhered to the underlying endometrium. Histologically, trophoblasts located deeper surrounded the myometrial arteries and rarely invaded their muscular tunic; no trophoblasts were found in the mesometrial tissues, unlike the lesions in the capybara of this report. In golden hamsters, giant trophoblasts can transmurally invade the uterus and be found within mesometrial vessels and persist for up to 3 weeks postpartum. 6 According to keepers, this capybara's last litter was over 1 year earlier, but this was difficult to confirm based on the animal identification records and the size of the enclosure and capybara herd. It is considered possible that this animal may have had a more recent litter that led to the lesions of this report. This is the first report of placental subinvolution in a capybara or any rodent species to the authors' knowledge. Placental subinvolution in this capybara was more severe than is described in the bitch, 1, 2 perhaps due to a more invasive behavior of trophoblasts, and was accompanied by myometrial to full-thickness ischemic necrosis of the uterine wall surrounding the subinvoluted placental sites. The collagenous response in the endometrium of placental sites described in the bitch 2 was not observed in the capybara of this report.
The cysts on the serosal surface of the uterus were interpreted as remnants of the Mullerian ducts and therefore an incidental finding, but they also could be lymphatics dilated due to obstruction from concurrent uterine lesions.