
Abstract
Splenic laceration is a rare yet often underreported complication of colonoscopy that is infrequently discussed with the patient during the consent process. Most cases present within 48 h after the inciting colonoscopy; a delayed presentation is rare. We present a case of splenic laceration with hemoperitoneum that manifested 5 days after the initial colonoscopy. The patient was treated conservatively. Traditionally perceived risk factors such as intra-abdominal adhesions, splenomegaly, anticoagulation use, biopsy, polypectomy, a technically challenging procedure, and anesthesia assistance have not been clearly shown to increase the incidence of splenic injury following a colonoscopy. Since the risk factors of splenic injury remain unclear, the clinical presentation is nonspecific, and the consequences can be serious, the endoscopist should make an effort to inform the patient of this rare complication before the procedure.
Introduction
Colonoscopy is a widely adopted tool for colorectal cancer screening.1,2 Although it is generally a safe procedure, it does carry a small risk of complications. Two of the most frequently reported complications are bleeding and perforation, with an incidence of 0.17-0.53% and 0.046-0.25%, respectively.3,4 Less common complications include pneumomediastinum, pneumothorax, volvulus, hernia incarceration, retroperitoneal abscess, retroperitoneal emphysema, appendicitis, septicemia, and splenic laceration, not all of which are routinely disclosed to the patient during the consent process.5,6 Splenic injury (SI) is an infrequent complication of colonoscopy that is often underrecognized and underreported, yet can lead to significant morbidity and mortality.1,5 It was first documented in 1974 and since then, only over 100 cases have been indexed in the world literature.4,7 Due to its rarity, our knowledge about its occurrence has been limited to case reports and case series. Most cases of SI manifest within 48 h after the inciting colonoscopy; a delayed presentation is rare.6,8 We report a delayed presentation of splenic laceration post-colonoscopy that was managed conservatively. This case also highlights the fact that this complication may be far more common than reported as many patients may not develop symptoms significant enough to warrant medical attention.
Case presentation
A 63-year-old female with a medical history of type II diabetes mellitus, hypertension, seizure disorder, gastroesophageal reflux disease, gout, and vitamin D deficiency presented to the emergency department (ED) with a 2-day history of worsening abdominal pain. The patient described the pain as crampy and worse on the left side. She had undergone an outpatient colonoscopy 5 days prior to evaluate a recent history of weight loss. The colonoscopy was not reported to be difficult, and only diverticulosis was found. There were no other intraoperative events. The patient denied trauma following the procedure. She reported dizziness but not nausea, vomiting, change in bowel habits, hematochezia, melena, fever, or chills. A physical examination revealed diffuse abdominal tenderness that was worse in the left upper and lower quadrants. There was no guarding. Her vital signs were stable: the blood pressure was 163/67, heart rate was 93, respiration was 15, and temperature was 36.7°C.
Laboratory studies revealed a hemoglobin (Hgb) of 9.1 g/dL, down from a baseline of 11.5 g/dL. Her white cell count was 6.8 K/μL and creatinine was 0.58 mg/L. Other studies including the liver enzymes, bilirubin, lipase, albumin, coagulation profile, and urine analysis were unremarkable. An upright chest X-ray showed no free air under the diaphragm. A contrast-enhanced computed tomography (CT) of the abdomen and pelvis was performed which demonstrated a 1.2 cm posterior inferior splenic laceration with a 7.6 × 3.4 cm subcapsular splenic hematoma and a moderate hemoperitoneum (Figure 1). Incidentally, radiographic changes of chronic pancreatitis were also identified, including pancreatic atrophy, diffuse pancreatic calcifications, and pancreatic duct dilatation. This was likely related to the patient’s history of alcohol abuse.
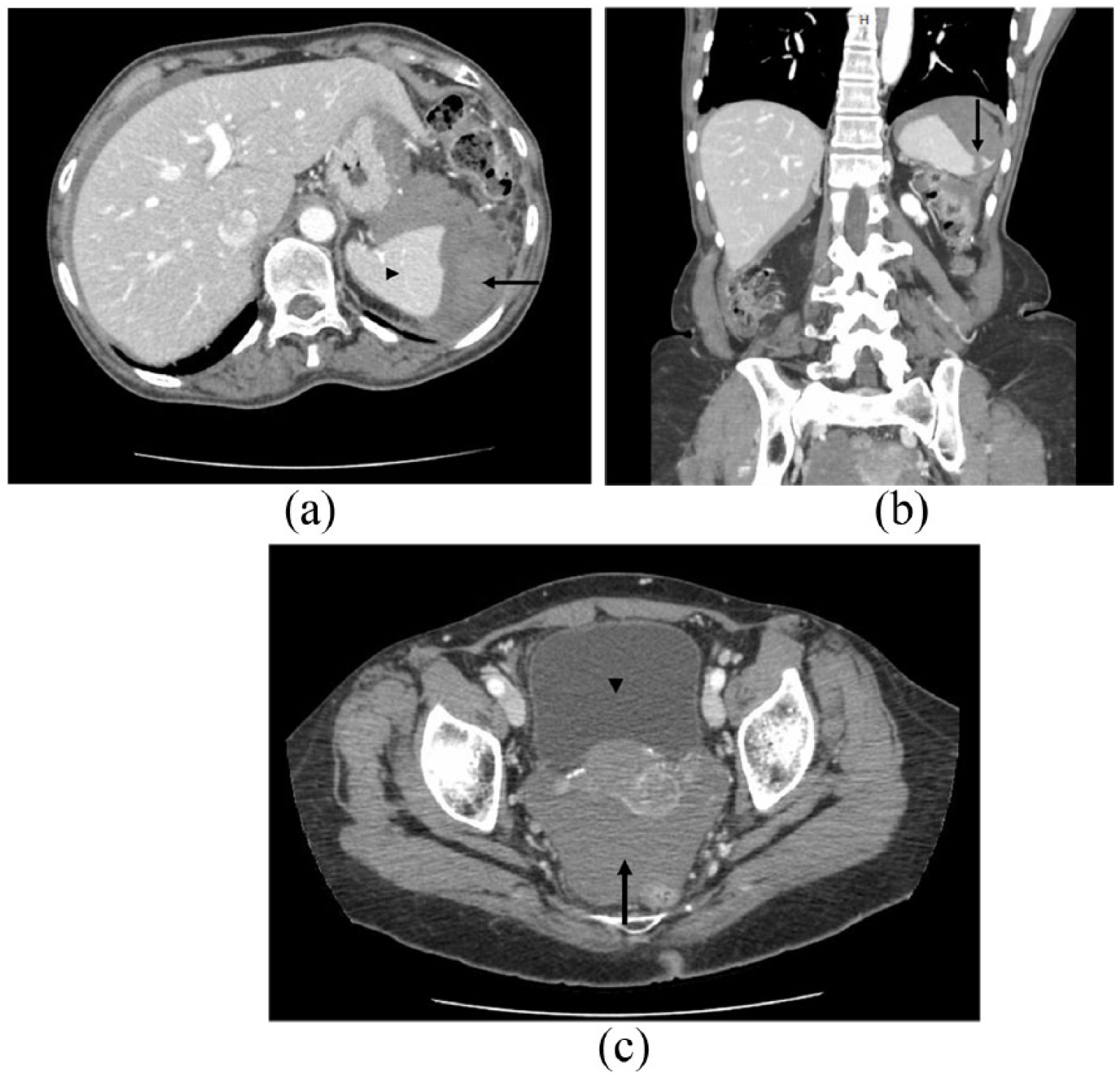
(a) Subcapsular splenic hematoma. The spleen (arrowhead) is displaced by high-density fluid (Hounsfield unit of 69, arrow) consistent with a loculated hematoma underneath the splenic capsule. (b) Splenic laceration. There is a linear defect in the spleen (arrow) measuring 1.2 cm in depth representing a splenic laceration. (c) Hemoperitoneum. There is free fluid (arrow) in the peritoneal cavity that displays a Hounsfield unit of 65 consistent with blood, in contrast to the fluid content of the bladder (arrowhead) which has a Hounsfield unit of 15.
The differential diagnoses prior to the diagnostic CT included colonic perforation, diverticulitis, and acute pancreatitis. Since the patient had stable hemodynamics, a conservative approach was employed. She received fluid resuscitation and was admitted to the surgical step-down unit for observation. Her symptoms improved significantly over the next 2 days and her Hgb and vital signs remained largely unchanged. She was discharged home on day 3 of the hospitalization.
The patient was evaluated 2 weeks after discharge in the clinic setting. Her abdominal pain had completely resolved and her Hgb was restored to 12.4 g/dL. An upper abdominal ultrasound was performed 1 month post-discharge and revealed resolution of the hemoperitoneum and a reduction in the size of the splenic hematoma (4.3 × 3.2 cm).
Discussion
SI is a rare complication of colonoscopy.1,4 It is thought to be underrecognized and underreported, and thus, its exact incidence is not known.1,5 The most extensive study to date of over 3 million patients suggested an incidence of 0.0045%, which was higher than previously estimated.1,4,7,9 It has a mortality of 5% and can lead to significant morbidity given that the majority of patients require a splenectomy.1,2 More than 80% of the patients present within 48 h after the inciting colonoscopy; however, symptom onset can be delayed up to 8 days.6,8 The most frequent symptoms include abdominal pain, referred pain to the left shoulder (Kehr’s sign), and hypotension.2,5 These can be nonspecific however, so a high index of clinical suspicion is essential for the diagnosis. In fact, post-procedural abdominal pain is often attributed to air insufflation, and a small splenic laceration presenting in this manner could be missed.
The gold standard for diagnosis is a contrast-enhanced CT, which not only evaluates the extent of the SI but also identifies active extravasation and other intra-abdominal pathologies.10–12 It additionally has a sensitivity and specificity higher than non-contrast CT and ultrasound, exceeding 95% in several studies.10,11 If the patient is unable to tolerate CT due to hemodynamic compromise, a bedside ultrasound can be considered.1,2,10–12 The American Association for the Surgery of Trauma divides the severity of SI into five levels.1,12,13 Injuries grade III and above are likely to fail non-operative management. However, this scheme applies to traumatic SIs only and has no proven validity or predictability for colonoscopy-related SIs.5,13 In this scenario, hemodynamic instability has been determined to be the best indicator for surgical intervention.1,13 Additional indications for surgery may include a hemoperitoneum which predicts progression to shock, and persistent symptoms despite initial conservative management.13,14 Studies have shown that more than 75% of known SI cases required splenectomy as the definitive treatment. 2 Splenic artery embolization can also be considered in patients with active bleeding but stable hemodynamics. 13
The mechanisms of SI during a colonoscopy are thought to be due to excessive traction on the splenocolic ligament by the scope as well as direct trauma to the spleen during the scope insertion, leading to splenic capsule avulsion. 1 It has been proposed that adhesions from a prior surgery and chronic inflammation due to pancreatitis, diverticulosis, or inflammatory bowel disease can decrease the mobility between the spleen and the colon, thus predisposing a patient to SI.5,6 However, such an association has not been clearly established in the literature.1,2,5,6 In fact, most studies have shown that the larger proportion of patients who experienced SI post-colonoscopy did not have adhesions during laparotomy.2,5,7 Our patient was incidentally found to have chronic pancreatitis on CT, but it was unclear whether this was a risk factor for her SI. Similarly, there have been no clear correlations found between the incidence of SI and older age, anticoagulation use, splenomegaly, biopsy, polypectomy, or a technically difficult colonoscopy.1,2,5–7 The only association noted was with the female gender (78%). It is, therefore, challenging to predict which patients are at risk of developing SI during a colonoscopy. Anesthesia assistance during colonoscopy has also been proposed to increase the risk of SI due to an impaired sensation and expression of pain by the patient, although two major studies have proved this to be false.4,15 Anesthesia was not found to increase the risk of perforation, bleeding, or SI, although it did increase the risk of aspiration pneumonia during colonoscopy. Procedural factors such as the slide-by advancement, hooking at the splenic flexure to straighten the sigmoid loop, creating an alpha loop, applying external pressure to the left hypogastrium, and supine positioning may all exacerbate the tension on the splenocolic ligament and predispose the patient to SI.1,5 However, since most colonoscopy reports do not contain information on the maneuvers performed intraoperatively, it would be difficult to establish these maneuvers as the cause of SI.
Given that SI due to colonoscopy can be fatal and there are no clearly defined risk factors to predict its onset, all patients should be informed of this serious albeit rare complication. From our own institutional experience, SI was not routinely discussed with the patient during the consent process. There have been lawsuits reported in Italy involving SI post-colonoscopy.16,17 For both the patient’s understanding of the inherent risks of a minimally invasive procedure and medicolegal obligations, the endoscopist should make an effort to discuss this rare but potentially fatal complication with his or her patient.
Conclusion
SI is an infrequent yet underrecognized complication of colonoscopy. The presentation may be nonspecific, and the risk factors remain elusive. A physician’s clinical acumen is key in formulating the diagnosis. Patients undergoing colonoscopy should be informed about this rare but severe complication given its unpredictable nature and potential medicolegal consequences.
Footnotes
Acknowledgements
We thank Dr. Claudia Lapidus for providing radiological review of this case.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from New York Presbyterian-Brooklyn Methodist Hospital
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.