
Abstract
A 3- to 4-month-old female Golden Retriever dog presented with right hind limb enlargement. Physical examination of the limb and radiographic findings initially included soft tissue swelling with elongation, bowing, and cortical irregularity of the femur and tibia. During a period of approximately 7 months, pathology in the limb progressed to include tarsal laxity, muscle atrophy, avulsion of the gastrocnemius muscle, and luxation of the patella. During surgical intervention to shorten the limb and repair the patellar luxation, a large soft tissue cyst was identified along the caudal aspect of the femur and stifle. The limb was later amputated, and a final diagnosis of malignant peripheral nerve sheath (PNS) tumor of the sciatic nerve and surrounding soft tissues was made. The unilateral limb enlargement in this dog appears to have been because of the development and progression of a malignant PNS tumor. The presentation and associated pathologic changes in the limb are unusual for canine PNS tumor but have similarities with neurofibromatosis in the limbs of humans.
There are no previous reports of an association between peripheral nerve sheath (PNS) tumors or soft tissue sarcomas and the presentation of unilateral limb enlargement in dogs. Both tumor types have been described frequently in many veterinary species 2, 5, 15, 16, 19 including dogs, but the presentation of limb enlargement is rarely reported. 12 In dogs, benign PNS tumors have been designated neurofibroma and Schwannoma, and malignant PNS tumors include neurofibrosarcoma and malignant Schwannoma, 5, 19 but these designations are often unclear in veterinary species. Categorization is clouded by the entity termed canine hemangiopericytoma, which has different gross and histologic characteristics from the human tumor with the same name 6 and in veterinary species is believed to be a variant of a PNS tumor. 5 Adding to the diagnostic dilemma, perineurial origin in canine tumors is difficult to identify because epithelial membrane antigen immunohistochemical methods do not label canine peripheral nerve and no reliable marker for perineurial cells exists for veterinary species. Furthermore, the lack of a perineurial marker makes distinction between neurofibroma and Schwannoma difficult and distinction of these tumors in the veterinary literature has often been based purely on histologic architecture. 5, 19
A female Golden Retriever was adopted as an apparently normal, 2- to 3-month-old puppy. She was first presented to the referring veterinarian with a history of an enlarged right hind limb, noticed within the first few weeks of adoption. Initial physical exam findings included nonpainful right hind limb swelling from midfemur to metatarsus with full range of motion in all joints. Radiographic findings included increased length of the right leg as compared with the left and irregular contour of the right femur and tibia. There was no bone lysis and no known history of trauma. The dog returned at approximately 6 months of age for an ovariohysterectomy, and follow-up radiographs of her pelvis and hind limbs revealed unresolved abnormalities of the right hind limb. A veterinary radiologist interpreted the changes as right acetabular, femoral, and tibial/fibular fractures, most likely resulting from previous trauma. The dog developed intermittent toe touching to non–weight-bearing lameness in the right hind limb until her referral to the University of Wisconsin Veterinary Medical Teaching Hospital, at approximately 10 months of age. On physical exam, there was right hind limb soft tissue swelling, laxity in the right tarsal joint, the femur and tibia of the right leg appeared abnormally long, and there was muscle atrophy of the right hind limb. Radiographic measurements revealed that the right femur and tibia were significantly longer than the left (lateral views were measured as right femur, 21.5 cm; left femur, 19.2 cm; right tibia, 21.4 cm; left tibia, 17.0 cm). The diameter of the medullary canals of these bones was also increased. Additional radiographic findings included midshaft cranial bowing and mild medial deviation of the right femur, decreased opacity of the entire medullary canal, thinning and irregularity of the lateral cortex from the midshaft distally to the physis, lateral subluxation of the right coxofemoral joint, and acetabular remodeling. Distal displacement and fragmentation of the fabella were suggestive of avulsion of the right gastrocnemius muscle, and the right patella had a grade 4 medial luxation (Fig. 1a, b). The right tibia had similar bowing and changes in cortical and medullary opacity to the femur, and the soft tissues around the right tibia were thickened (Fig. 1c, d). A selective angiogram of the right femoral artery revealed increased soft tissue contrast uptake around the right proximal tibia and distal femur, interpreted as possible arteriovenous fistulas in the area of the stifle. Surgical intervention to shorten the right hind limb included ostectomy of the femur, tibia, and fibulae, followed by bone plating, and at the same time the patellar luxation was repaired. Findings during surgery included a greater than normal amount of subcutaneous adipose and a large cystic structure located on the caudolateral aspect of the cranial one third of the femur, close to the periosteum. The cyst extended to the soft tissue behind the stifle joint and proximal lateral tibia, where it was partially dissected. The cyst and the bone slabs were submitted for histopathology. The bone had thin, irregular cortices, the cyst had a prominent vascular component, and no neoplastic cells were identified. Four weeks later the dog presented with a fracture at the base of the right femoral neck above the proximal end of the femoral plate. The femoral head was displaced cranially. The right hind limb was amputated, and postsurgical dissection revealed adherent, red-brown, friable tissue surrounding the proximal portion of the sciatic nerve and a 2.5 × 3.0 cm cystic space along the caudolateral femur filled with red-brown, gelatinous material. The common peroneal and tibial portions of the sciatic nerve were expanded markedly from the amputation site distally to the level of the caudal stifle (a length of 8.0 cm). Histopathology of amputated tissues revealed a wide variety of lesions. Along the midshaft of the tibia, the point at which the tibia showed greatest gross abnormality, there were poorly circumscribed areas of malignant spindle cell proliferation within tendons and tendon sheaths, the gastrocnemius, and surrounding adipose. The spindle cells had moderate anisokaryosis, binucleation, and there were 10 mitoses per ten 40× fields. The adjacent bone was remodeled, and there was fibrosis around large medullary blood vessels. Sections from other locations along the femur and tibia revealed disruption and scalloping of the outer cortical bone and mild expansion and extension of periosteum into the bone and around penetrating blood vessels. The soft tissue cyst was similar to that described previously after the ostectomy. Both the peroneal and tibial portions of the sciatic nerve were expanded evenly within an intact nerve sheath. The nerves contained a loose arrangement of small spindle cells with pale eosinophilic, trailing cytoplasm. The cells were widely separated, and infrequently scattered among them were axons and moderate numbers of blood vessels (Fig. 2a). A Bielschowsky silver stain highlighted swelling and segmentation in the axons, and Luxol fast blue staining was minimal. S-100 immunohistochemistry was weakly, multifocally positive, and the spindle cells were vimentin positive. Trichrome staining for collagen was weak within the nerve, in sharp contrast to the dark blue staining of the sheath and connective tissue around blood vessels. A few small adjacent nerve branches revealed hypercellularity and nerve sheath expansion by small spindle cells. The spindle cells in the sciatic nerve had a benign appearance, but in multiple soft tissue locations along the limb, they had malignant features. Three weeks after the limb amputation, a 13.0 × 10.0 × 20.0 cm soft tissue mass that enveloped a portion of the right ischium had developed at the amputation site. The mass was composed of spindle cells with malignant features as described previously, and the mitotic rate was up to 47 per ten 40× fields (Fig. 2b). Excision of the mass with subtotal pelvectomy was performed after this diagnosis.
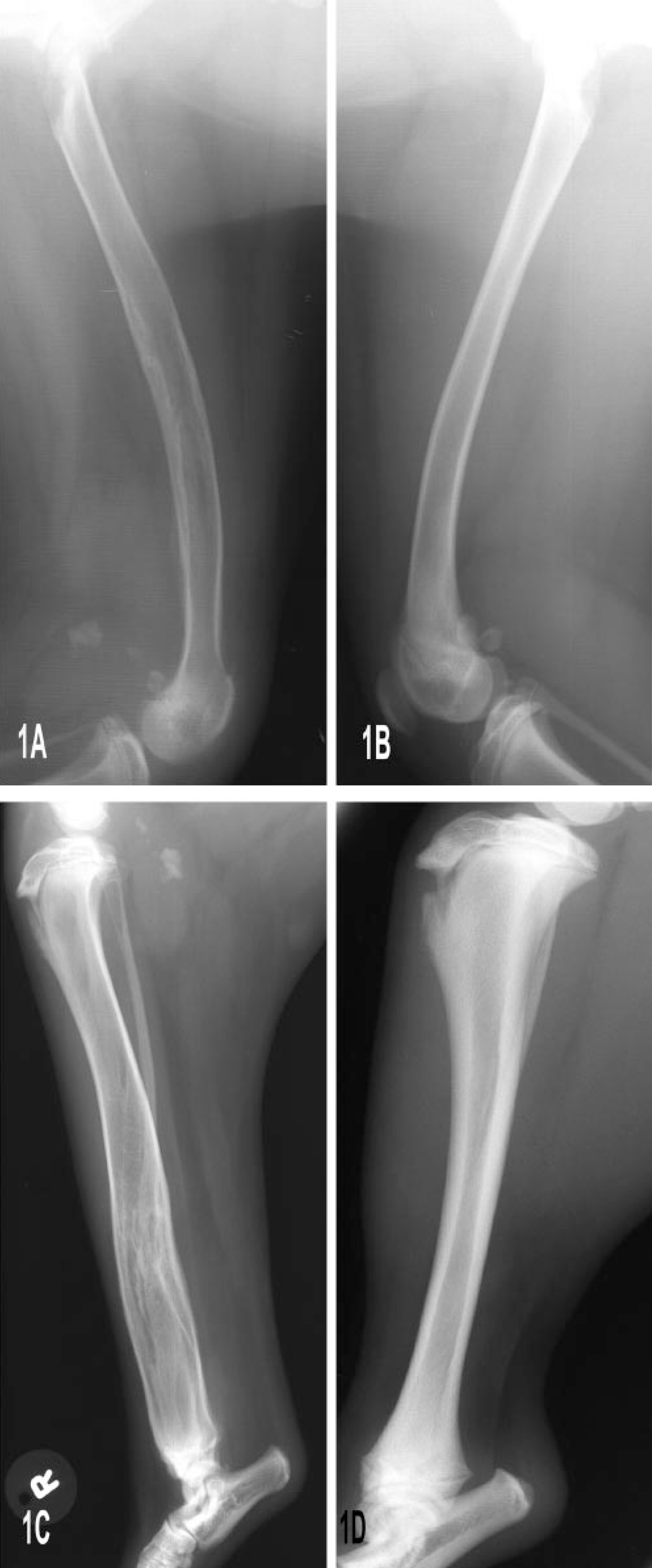
Hind limbs; Golden Retriever dog. Radiographs showing the described alterations in the length, contour, and density of the abnormal (right) femur
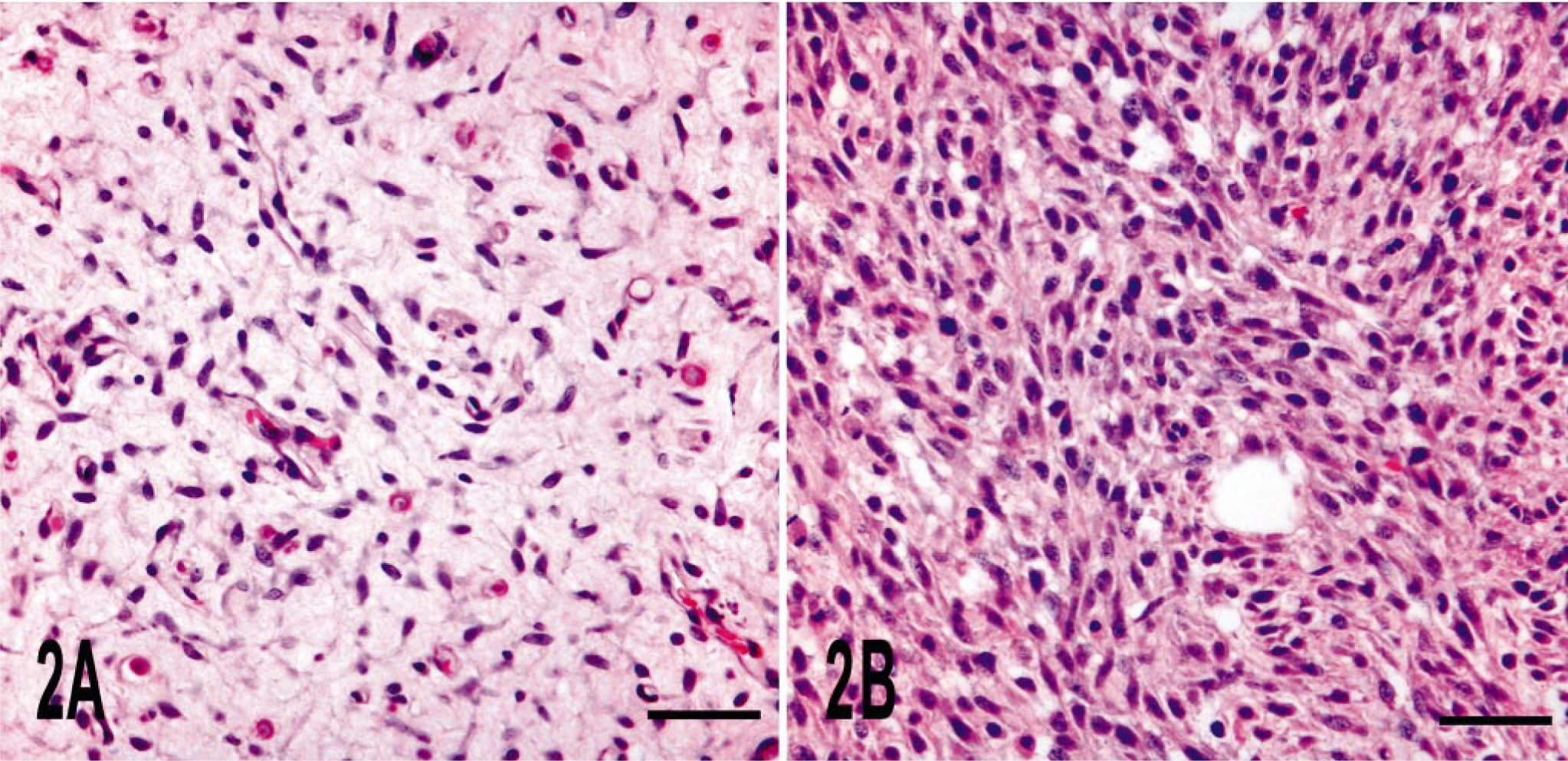
Right hind limb soft tissue sections; Golden Retriever dog. The sciatic nerve is infiltrated by a hypocellular well-differentiated spindle cell neoplasm
Initial tissue sections revealed a benign PNS tumor in the sciatic nerve. However, in later resections, a diffusely infiltrative malignant neoplasm was identified in distal limb tendons and in soft tissues around the hip. Although a transition site between the two forms was not found, and in the more malignant tissue from the last resection nerves containing malignant cells were not identified, we believe rapid malignant progression of an initially benign PNS tumor occurred in this dog. Single limb enlargement has not been reported in association with peripheral nerve or soft tissue neoplasia (or both) in dogs, and the addition of the bone, vascular, and soft tissue abnormalities in this dog make it all the more unusual. Descriptions that bear the greatest similarity to this dog are of humans with neurofibromatosis. 4, 9, 10, 13, 14, 17, 20 Malignant PNS tumors arising from neurofibromas in humans with neurofibromatosis have been well described. 21 Among the musculoskeletal abnormalities reported in humans with neurofibromatosis is a triad of limb pathology that includes enlargement of a limb or limb part, recurrent subperiosteal hemorrhages, and subsequent cyst formation. 11 An association between some of the skeletal manifestations associated with neurofibromatosis type 1 and loss of function of the NF1 gene has been described recently. 8 Other human syndromes associated with limb or digit hypertrophy include Klippel-Trenaunay-Weber syndrome, 7, 14 Proteus syndrome, 14 lipofibromatous hamartoma, 1, 3, 4 and macrodystrophia lipomatosa. 14, 18 Increased fibroadipose tissue is a feature of the latter two syndromes that was also found in this dog. These human syndromes have similarities to the dog described in this report and provide documented associations between limb overgrowth, peripheral nerve tumors, and soft tissue pathology not currently found in the veterinary literature.
Footnotes
Acknowledgements
We would like to thank Dr. Reza Hafez for pathology consultation, Lona Barsness and Kermit Groothius for preparation of histologic sections, and Anne Slattery for immunohistochemistry technical support.