
Abstract
Dilated cardiomyopathy (DCM), characterized by chamber dilatation and myocardial systolic and diastolic dysfunction, is one of the most common heart diseases in dogs. The clinical diagnosis is based on findings on echocardiographic and Doppler examinations, with the active exclusion of other acquired or congenital heart diseases. However, the echocardiographic criteria for the diagnosis of DCM are not wholly specific for the disease, and histologic examination may be necessary for final diagnosis. Review of reports on histologic findings in dogs with clinically diagnosed DCM reveals two histologically distinct forms of DCM: 1) cardiomyopathy of Boxers and Doberman Pinschers, corresponding to the “fatty infiltration-degenerative” type and 2) the form seen in many giant, large-, and medium-sized breeds, including some Boxers and Doberman Pinschers, classified as the “attenuated wavy fiber” type of DCM. The histologic changes of the attenuated wavy fiber type of DCM may precede clinical and echocardiographic signs of heart disease, thus indicating an early stage of DCM.
The classification of cardiomyopathies introduced by the World Health Organization is based on pathophysiology or, where possible, on etiologic or pathogenetic factors. Dilated cardiomyopathy (DCM) is characterized by chamber dilatation and predominantly systolic and, to a lesser degree, diastolic dysfunction. 66 DCM was first reported in dogs in 1970, as congestive heart failure (CHF) in conjunction with dilatation of the cardiac chambers and absence of other clinically important cardiovascular disease by Ettinger, Bolton and Lord. 28 DCM has been recognized in many breeds 85 but seems to be more prevalent in certain breeds such as English Cocker Spaniels, 78 Doberman Pinschers, 14 Boxers, 35 Newfoundlands, 23 , 84 and Irish Wolfhounds. 95
Gross pathology examination of dogs with DCM generally shows dilatation of all four cardiac chambers or predominant dilatation of the left cardiac chambers. There appears to be at least two histologically distinct forms of canine DCM: 1) the cardiomyopathy of Boxers 35 and of Doberman Pinschers, 14 , 15 , 30 , 36 corresponding to the “fatty infiltration–degenerative” type of DCM and 2) the form detected in many giant, large-, and medium-sized breeds (including some Boxers and Doberman Pinschers), which can be classified as the “attenuated wavy fiber” type of DCM. 1 , 21 , 69 , 77 , 82 , 83 , 88 , 96 Presumably, specific histologic myocardial changes reflect specific disease processes. Aiming for a histologic confirmation and classification of clinical cases of DCM is essential for increasing our knowledge of the disease.
Etiology and Pathogenesis
The etiology is generally not established in the individual case of DCM in dogs. However, several causes have been proposed, including genetic factors, nutritional deficiencies, metabolic disorders, immunologic abnormalities, infectious diseases, and drug-, toxin-, and tachycardia-induced myocardial hypokinesis.
DCM is considered to be hereditary in approximately 20–35% of human patients. 56 , 74 Canine DCM has been suspected to be an inherited disease because of its prevalence in certain breeds and in specific families of dogs. 76 An autosomal dominant mode of transmission has been reported in the Irish Wolfhound, 18 Newfoundlands, 24 and Doberman Pinschers. 54 In the juvenile Portugese Water Dog, an autosomal recessive transmission has been documented. 1 , 21 , 77
The role of cytoskeletal proteins has been investigated in the development of DCM, and the dystrophin gene has been identified as being responsible for X-linked DCM. 89 Canine X-linked muscular dystrophy may cause severe cardiac involvement, 91 and deletion of the entire dystrophin gene has been demonstrated in German Shorthaired Pointers with skeletal myopathy and DCM. 70 Mutations in the actin gene have been associated with DCM in humans. 63 However, molecular analysis of the cardiac actin gene in 16 Doberman Pinschers with DCM did not reveal any abnormalities. 55
Nutritional abnormalities causing myocardial hypokinesis, i.e., carnitine or taurine deficiencies (or both), have been described in humans, 65 dogs, 38–41 , 43 and cats. 64 Metabolic disorders associated with DCM include hypothyroidism, diabetes mellitus, and pheochromocytoma. 4 , 76 , 98
Immunologic processes have been suspected to be involved in the pathogenesis of DCM because auto-antibodies have been detected against several cardiac structures, such as the ß-adrenergic receptor, 47 the mitochondria, 45 , 72 , 73 and the myosin heavy chains, 13 both in humans and in experimental animals. However, many of these antibodies do not seem to be specific for DCM because they are also detected in myocarditis, hypertrophic cardiomyopathy, and hypertensive heart disease. 5 Inflammatory response to infectious agents, such as viruses, 2 , 12 , 17 , 58 bacteria, 46 , 79 and protozoa, 6 , 7 has been proposed to be involved in the pathogenesis of myocarditis and DCM.
Cardiotoxicity may be caused by doxorubicin and other antineoplastic agents, ethanol, cobalt, lead, catecholamines, histamine, methylxanthines, and vitamin D. 93 Studies on naturally occurring tachycardia as well as experimentally induced tachycardia report development of chamber dilatation and CHF. 3 , 34 , 60 , 97
Clinical Findings
Overt DCM, i.e., dogs with DCM exhibiting signs of CHF or arrhythmias, is preceded by a preclinical stage of various lengths. Clinical signs in dogs with DCM include dyspnea, cough, depression, exercise intolerance, inappetence, syncope, weight loss, abdominal distention, and polydipsia. The clinical examination commonly reveal tachypnea, dyspnea, tachycardia, arrhythmia, a low-intensity systolic murmur in some dogs, weak femoral arterial pulses, ascites, and weight loss. 76 , 85 Most dogs with DCM show abnormalities on electrocardiogram recordings, such as atrial fibrillation or ventricular arrhythmias. Radiographic findings in dogs with DCM include cardiomegaly with prominence of the left atrium, pulmonary venous congestion, and interstitial or alveolar pulmonary edema. These changes are diagnostic of left-sided or biventricular CHF and not specific for DCM. The diagnosis of DCM is usually based on echocardiographic findings of myocardial hypokinesia and chamber dilatation, with the active exclusion of other significant congenital and acquired heart disease. The sensitivity of standard clinical and echocardiographic criteria was found to be 93% in one study, when final diagnosis is based on postmortem findings. 82 Differential diagnoses included arteriosclerosis, myocardial infarcts, endocardiosis, and myocarditis.
Survival and Prognosis
Survival times in dogs with DCM vary from days to several years. Attempts to correlate different clinical and echocardiographic parameters with prognosis have been made. In one study of 189 dogs with DCM, only 3 of 27 tested variables were shown to influence survival, i.e., young age at onset of clinical disease, dyspnea, and ascites. 86 Another study of 37 dogs identified pleural effusion and pulmonary edema as independent prognostic indicators for dogs with DCM. 57 Neither of these studies found breed or parameters of systolic function to be significant prognostic factors in DCM. Survival rate at 1 year varied between 3 and 54% in different studies. 9 , 10 , 16 , 29 , 50 , 57 , 80 , 86 , 87 , 95 The wide variation in survival times may partly depend on different functional classes of CHF in different studies. Medical treatment, especially the use of angiotensin-converting enzyme inhibitors and ß-blocking agents, varied considerably between different studies, which also may be a source of variation in survival times. However, the exceptionally low survival rate at 1 year of Doberman Pinschers (3%) may indicate that the fatty infiltration–degenerative type of DCM carries a worse prognosis compared with the attenuated wavy fiber type of DCM.
Gross Pathology and Histopathology
Gross pathology examination of the heart of dogs with DCM generally reveals marked dilatation of all four chambers or predominantly the left chambers. In one study, dilatation of all four chambers was found in 85% of dogs with DCM. 85 Myocardial eccentric hypertrophy, rather than true dilatation, is evident by increased heart weight to body weight ratio, together with a decreased ratio of the left ventricular thickness to chamber diameter. 76 , 85 The term hypertrophy implies a pathologic process where the weight of the organ is increased because of an increase in cell size rather than in cell number. In myocardial eccentric hypertrophy, the sarcomeres are increased in numbers in series rather than parallel, as in concentric hypertrophy. Myocardial eccentric hypertrophy is commonly caused by volume overload. 44
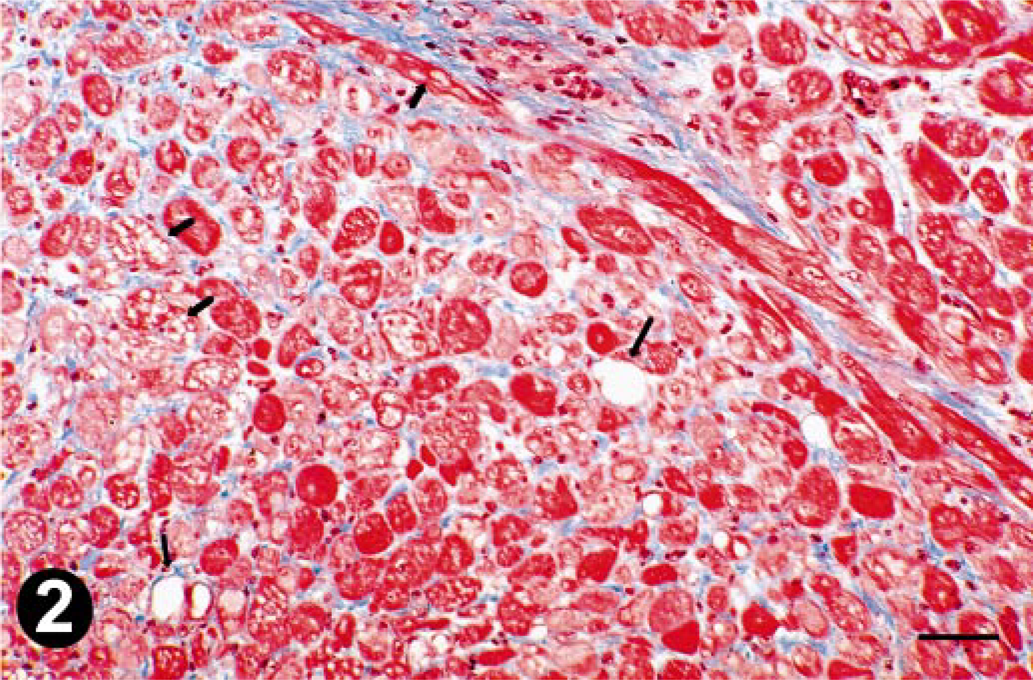
In the literature, there appear to be two histologically distinct forms of canine DCM: the attenuated wavy fiber type seen in many giant, large-, and medium-sized dogs, and the fatty infiltration–degenerative type of DCM seen in mainly Boxers and Doberman Pinschers (Table 1). Some other studies report nonspecific findings, such as necrosis, infarcts, fibrosis, vacuolization of myocytes, and hyperplasia of arteries. 33 , 51 , 78 , 94
Classification of canine DCM in different studies in chronological order, based on the reported histopathologic characteristics.
— = information not available.
The attenuated wavy fiber type of DCM
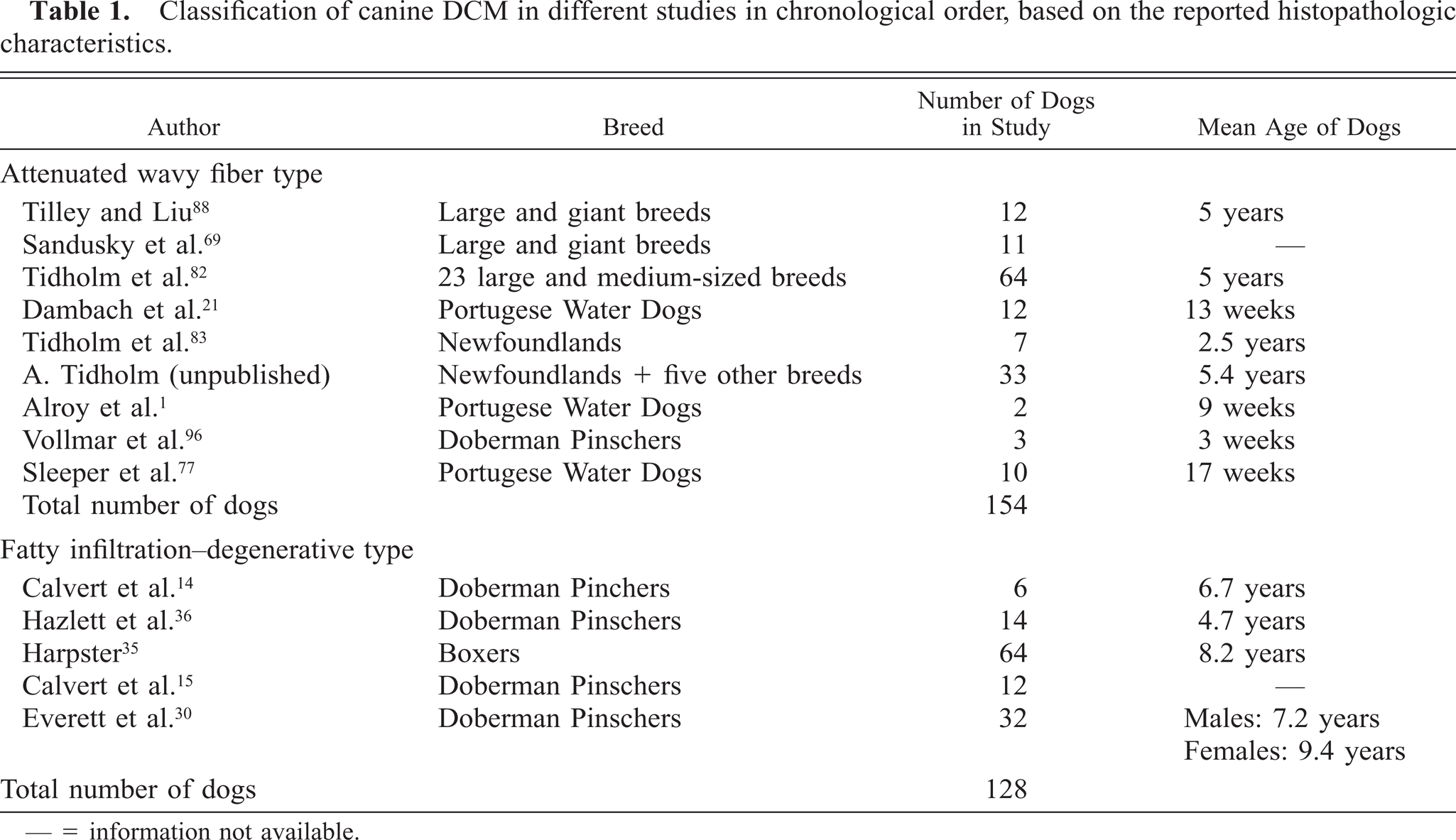
It has been described in dogs, 1 , 48 , 69 , 77 , 82 , 83 , 88 , 96 cats, 49 and human patients (Fig. 1). 22 , 71 Atrophy, or attenuation, of myofibers without a wavy appearance has been reported in several additional studies in human patients with DCM. 25 , 32 , 37 , 61 , 62 , 67 , 90 Myofiber atrophy is a common response to processes that prevent normal contractile activity and to various pathologic stimuli. 19 Atrophy of cardiac myocytes has been shown to occur after prolonged mechanical support using left ventricular assist device systems 42 and after heterotopic isotransplantation. 68 Wavy myocardial fibers, especially when associated with focal edema, are characteristic signs of acute myocardial ischemia in humans 26 and in dogs, 26 , 27 but have also been described in human patients with DCM. 52 , 59
Left ventricular myocardium of a dog with attenuated wavy fiber type of DCM. The myofibers are thinner than normal and have a wavy appearance. Masson's trichrome. Bar = 20 µm.
The myocardial lesions associated with the attenuated wavy fiber type of DCM consist of myocardial cells <6 µm in diameter (normal myofiber diameter ranges from 10 to 20 µm 92 ) with a wavy appearance, comprising at least half of the thickness of the myocardial specimens from the upper and lower portions of the left ventricular wall. The myocytes are separated by a clear space generally free from cellular infiltrates, suggestive of edematous fluid. In many cases, there is also a diffuse infiltration of subendocardial fibrosis (Fig. 1). It is suggested that myocardial specimens should be taken from the proximal (1–1.5 cm distal to the base of the atrioventricular valves), distal (1–1.5 cm proximal to the apex), and middle (midway between the proximal and the distal specimens) portions of the lateral wall of the left ventricle, lateral wall of the right ventricle, and interventricular septum, and from the papillary muscles of the left ventricle. Three slides from each of the 10 specimens should be evaluated for the presence of attenuated wavy fibers. 82 , 83
Unfortunately, myocardial biopsy specimens collected in vivo from the right ventricle may not be sufficient for identifying dogs with attenuated wavy fibers because the abnormal myofibers were most abundant in the lateral wall of the left ventricle. 83 Detection of attenuated wavy fibers in the myocardium of dogs has been shown to have a high sensitivity (98%) for DCM. The specificity of this finding was found to be 100% because attenuated wavy fibers were not found in 147 necropsied dogs with other heart diseases, such as chronic valvular disease, congenital heart disease, myocardial infarcts, myocarditis or endocarditis, although the majority of these hearts were dilated. 82
In a subsequent study, attenuated wavy fibers were detected in Newfoundlands from a kennel with a known predisposition to DCM, but without clinical or echocardiographic evidence of heart disease. 83 These findings suggest that development of attenuated wavy fibers is not a response to chamber dilatation and stretching of the myocytes, as has been proposed. 71 To the contrary, attenuated wavy fibers may represent an early pathologic change in the myocardium of dogs with DCM.
The fatty infiltration–degenerative type of DCM
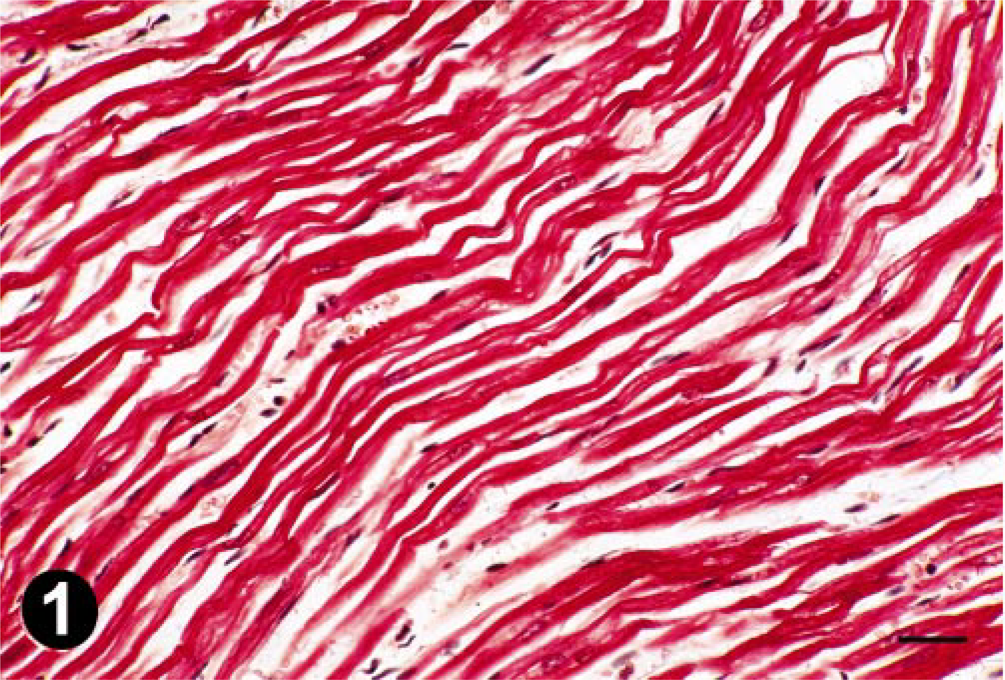
It was first described as “boxer cardiomyopathy” in 64 Boxers by Harpster 35 in 1983 (Fig. 2). The myocardial lesions associated with the fatty infiltration–degenerative type of DCM include myocytolysis, myofiber degeneration, vacuolization, and myocyte atrophy with extensive fibrosis and fatty infiltration replacing myofibers (Fig. 2). Similar myocardial lesions were first described by Calvert et al. in 1982 14 and later by the same and by other authors in a total of 64 Doberman Pinschers with clinically diagnosed DCM. 15 , 30 , 36 In one of the reports by Everett et al. the myocardial lesions have been described extensively, characterized by myofiber degeneration and atrophy, and replacement of myocardium by dense bundles of collagen and clusters of adipocytes. 30 The lesions have been compared to arrhythmogenic right ventricular cardiomyopathy (ARVC) in dogs 31 , 53 , 75 and in humans. 8 , 81 However, the myocardial changes in ARVC are usually confined to the right ventricle and profound to the extent that they are evident already on gross pathology examination. Myocyte transdifferentiation of myocytes to adipocytes was suggested as a possible mechanism for ARVC in a recent report. 20
Left ventricular myocardium of a dog with fatty infiltration–degenerative type of DCM. Vacuolar degeneration of myofibers (small arrows), atrophic myofibers, lipid deposits (large arrows), and cords of collagen (blue staining) are evident. Masson's trichrome. Bar = 20 µm.
Discussion
The attenuated wavy fiber type of DCM seems to be the most prevalent form of DCM because many more breeds are afflicted with this disease compared with the fatty infiltration–degenerative type of DCM. However, there are to date relatively few authors (Table 1) who have reported on this histopathologic finding. There may be many reasons for this lack of reporting. In the hitherto largest study of dogs with the attenuated wavy fiber form of DCM, as many as 27 slides from nine different locations in the ventricles were evaluated for presence of attenuated wavy fibers. Although, in many dogs, attenuated wavy fibers were found in the majority of the specimens, the abnormal fibers were most abundant in the lateral wall of the left ventricle. 83 By examining only a limited number of myocardial specimens, presence of attenuated wavy fibers may indeed be missed.
The technical process for preparation of the slides from the specimens may influence the morphology. The technique used for dehydration of the specimens may vary. The slicing technique may produce artificial waviness of the myofibers. There may be a question of whether the waviness may be an artifact in vitro, not present in vivo. The cause for this may be a disruption of collagen tethers aligning the cardiomyocytes that occurs in the remodeling process involved in dilatation. The artifact may reflect the loss of volume distention after death and fragmentation of collagen tethers that maintain alignment (J. Turk, personal communication). However, this supposed artifact only seems to occur in hearts where dilatation is due to DCM and not in hearts where dilatation is due to chronic valvular disease or congenital heart disease. 82 Also, attenuated wavy fibers have been found in myocardium of dogs where no dilatation is present. 83 Wavy myocardial fibers (not attenuated) have also been described in human patients and in dogs with acute myocardial ischemia. 26 , 27
Fibro-fatty replacement of myocardial tissue is thought to be a consequence of myocyte loss due to different causes, such as myocarditis or other noxious stimuli. Fatty infiltration of the myocardium is reported to be a major finding in ethanol-induced cardiomyopathy. 22 A number of antineoplastic agents, such as doxorubicin and cyclophosphamide, may cause extensive myocyte vacuolization. 93
The characteristic histologic findings presumably reflect specific disease processes, rather than being the end result of many different pathologic processes. As the very structure of the myocytes is distorted in the attenuated wavy fiber type of DCM, the cause may be a defect in the cytoskeletal proteins. It has been suggested that DCM in human patients should be termed “cytoskeletalopathy” due to mutations found in dystrophin, actin, and desmin. 11 The cytoskeletal proteins transmits the contractile force to adjacent sarcomeres and myocytes. Such an impairment will prevent normal contractility and, thus may cause myocyte atrophy.
In conclusion, there appears to be at least two histologically distinct forms of idiopathic canine DCM, presumably reflecting different disease processes. Histologic classification of canine DCM is therefore essential for scientific studies of the disease.