
Abstract
An adult quarter horse mare was presented with acute colic and fever. Physical examination and abdominocentesis showed septic peritonitis, and the mare was euthanatized. Necropsy and histopathologic examination revealed a focal partial perforation of the right ventral colon, which contained a single bot fly larva, identified as a third-instar larva of Gasterophilus intestinalis. This larva was embedded deep within the muscularis and the submucosa. Although bot fly larvae are known to attach to aberrant sites within the digestive tract, this is the first known report of deep penetration of the colon by a gasterophilus larva, with the resulting leakage of intestinal content leading to septic peritonitis.
Bot fly larvae of the genus Gasterophilus commonly infect horses throughout the world. The second- and third-stage larvae are normally found attached to the mucosa of the stomach (typically, G. intestinalis), duodenum (G. nasalis, G. haemorrhoidalis), or rectum (G. haemorrhoidalis, G. inermis), where they cause focal superficial mucosal ulceration. 2 There is little evidence of significant adverse health effects of gasterophilus infection, except for a few reports of gastric perforation and secondary peritonitis. 1 , 3
A 12-year-old quarter horse–pregnant broodmare was admitted to the equine clinic of the University of Montreal's veterinary teaching hospital with colic and fever of about 12-hour duration. The mare had a history of weight loss during the previous month, along with recurrent mild to moderate abdominal pain for the last 10 days and a 2-day episode of diarrhea occurring 7 days previously. At admission, the mare was sweating, depressed, and unresponsive. Heart rate was 100 beats/minute, respiratory rate 60 breaths/minute, and rectal temperature 39.6 C. Mucous membranes were dark red, capillary refill time was greater than 4 seconds, and dehydration was estimated at 10%. Nasogastric intubation yielded 5 L of gastric fluid and abundant foul-smelling gas. Transabdominal ultrasound revealed an abnormally large amount of free fluid between the ventral body wall and the viscera. Complete blood count, serum biochemistry, and arterial blood gas analyses revealed hyperfibrinogenaemia (6 g/liter), hypercreatinaemia (282 mmol/liter), and metabolic acidosis (bicarbonates, 16.2 mmol/liter). Abdominocentesis yielded turbid fibrinous sero-hemorrhagic fluid with 28.109 white blood cells/liter (neutrophils 98%), 45 g/liter total proteins, and numerous erythrocytes. Because of financial constraints and the guarded prognosis, the mare was euthanatized.
On necropsy, there was an abdominal effusion with several liters of turbid sero-hemorrhagic fluid containing fibrin. The abdominal serosa was multifocally congested, with petechiae and ecchymoses. In the stomach about 30 bot fly larvae were attached to the mucosa along the margo plicatus. There were extensive fibrinous adhesions between the base of the caecum and the proximal right ventral colon; these adhesions formed a cavity containing dark brown fibrinonecrotic material and lined by abundant fibrin. The wall of the right ventral colon in this area was markedly thickened with submucosal edema over an area about 20 cm in diameter. In the center of this area was a 5-mm-diameter circular perforation of the mucosa, exposing a 2- to 3-cm submucosal cavity containing fibrinonecrotic material, ingesta, and a single yellowish bot fly larva, 15 mm long, with its anterior end firmly embedded in the deep tissue (Fig. 1). It was identified according to Zumpt 4 as a third-instar larva of G. intestinalis by the presence of saddlelike excisions on its mouth parts and of two rows of blunt-ended spines per segment, interrupted dorsally on the 11th segment (Fig. 2).
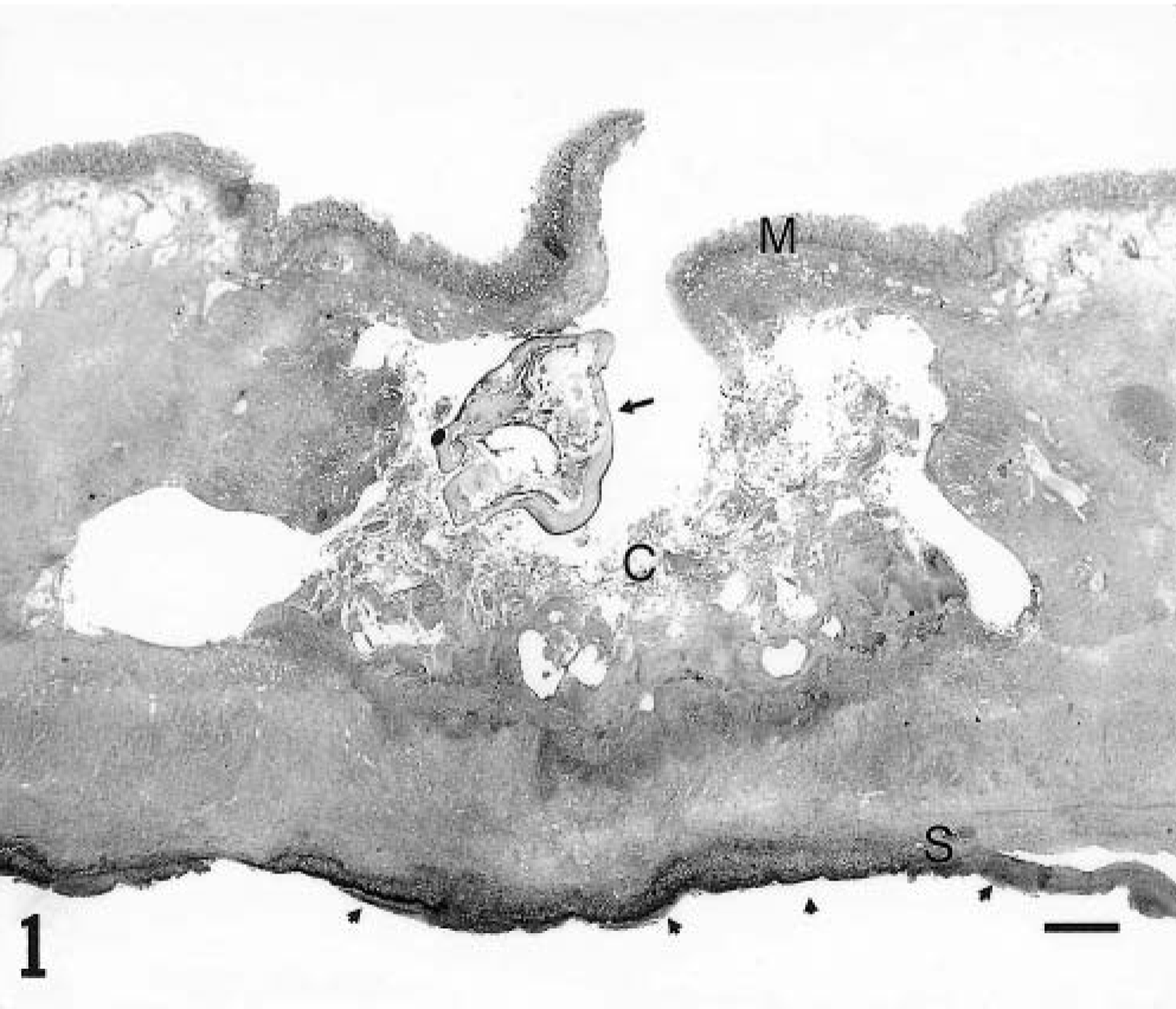
Colon; horse. The mucosa (M) is interrupted focally, and there is formation of a submucosal cavity (C) containing a gasterophilus larva (arrow) and necrotic debris. The serosa (S) underlying that cavity is covered by a thick layer of inflammatory cells and fibrin (arrowheads). Haematoxylin-phloxin-saffron stain. Bar = 2 mm.
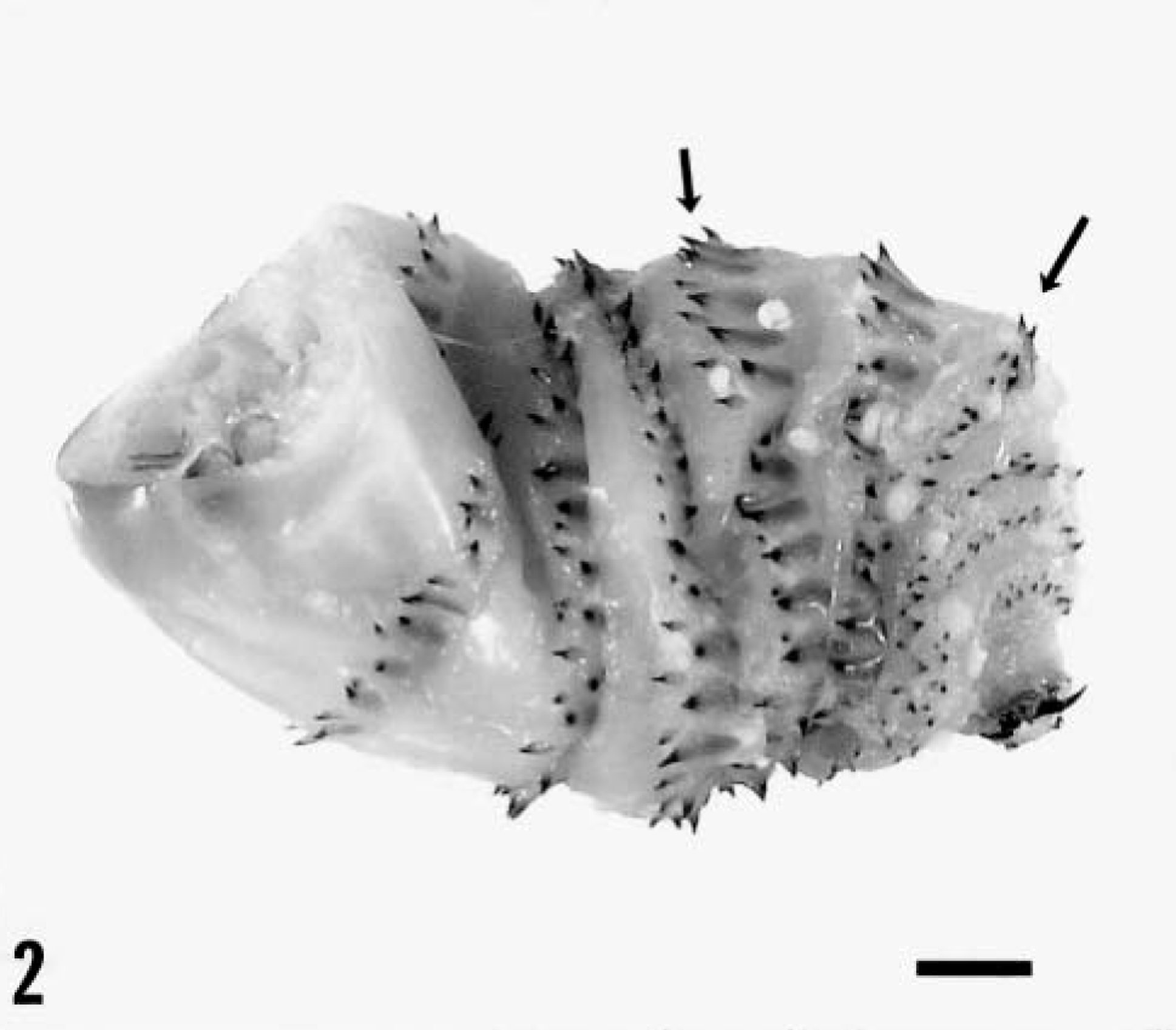
Photograph of the gasterophilus larva after extraction from the tissue. The two rows of spines per segment are visible (arrows). Bar = 1.5 mm.
Histologically, the tissue around the submucosal cavity was markedly edematous and infiltrated with macrophages and neutrophils. Deep in the cavity, there was a wide band of infiltration by neutrophils, often degenerate, which replaced the smooth muscle and extended to the serosa. The surface of the serosa was covered by a layer of fibrin containing degenerate neutrophils and macrophages, bacterial colonies, and some vegetal matter.
Histologic examination of the small and large intestines away from the perforation revealed a mild, diffuse infiltration of the mucosa and submucosa by eosinophils. Examination of other tissues showed generalized vascular congestion and a few microvascular bacterial emboli in the lung and the kidney.
To our knowledge this is the first report of deep penetration of a gasterophilus larva in the colon of a horse, with resultant peritonitis. Gasterophilus larvae can occasionally be found attached to various aberrant sites throughout the intestinal tract, presumably after premature detachment from their upper gastrointestinal predilection sites; for instance, G. haemorrhoidalis can reattach temporarily in the rectum. However, gasterophilus larvae usually cause only superficial ulceration and do not penetrate deep within the tissue. 2 One possible exception is G. inermis, which can insert up to half its body in a pitlike lesion, 2 but this does not usually lead to mural necrosis and peritonitis. The reason for the deep submucosal penetration of the G. intestinalis larva in the present case is unclear. The fairly thin and loosely attached mucosa of the large colon might render this site prone to deeper penetration. The presence of a preexisting eosinophilic colitis, although mild, might have increased the acute tissue reaction and damage after mucosal attachment by the parasite and led to secondary infiltration by colonic ingesta. The inflammation caused by invading colonic bacteria and foreign matter was probably the main factor leading to deep colitis, and the resultant loss of deep tissue integrity finally led to septic peritonitis.
Although the pathogenicity of gasterophilus infection is low, this case shows that atypical migrations or host reactions (or both) are possible, and underscores the importance of preventive antiparasitic treatment.