
Abstract
Tumors of the perianal area of dogs are common and include multiple tumor types. Whereas perianal adenomas occur often, adenocarcinomas of the apocrine glands of the anal sac occur less frequently. A review of the literature revealed no reports of squamous cell carcinomas arising from the epithelial lining of the anal sac. Squamous cell carcinomas originating from the lining of the anal sac were diagnosed in five dogs. Microscopically, the tumors consisted of variably sized invasive nests and cords of epithelial cells displaying squamous differentiation. Four of the five dogs were euthanatized because of problems associated with local infiltration by the tumors. In the fifth dog, there was no evidence of tumor 7 months after surgical removal, but further follow up was not available.
The perianal region of dogs contains multiple structures and glands, some of which are unique to the area. Anal sacs or perianal sinuses are paired, lateral, cutaneous, anal diverticula lined by a cornified, stratified squamous epithelium. Anal sacs are present in carnivores and many rodents. Dogs have apocrine tubular anal sac glands that open into the anal sacs. Sebaceous glands in the region are typical but may not be associated with hairs. Canine perianal or circumanal glands are nonpatent masses of parenchymal cells. They are sometimes referred to as hepatoid glands because of their histologic resemblance to hepatocytes. These glands are thought to be nonsecretory, abortive or modified sebaceous glands. 1
Although almost any tumor can occasionally affect the perianal region, the vast majority of tumors in this region arise from one of the glands mentioned above. Perianal adenomas comprise more than 80% of all perianal tumors and are the third most common tumor in male dogs. 7 Adenocarcinomas of anal sac apocrine glands are reported most often in female dogs and are aggressive tumors that often have associated hypercalcemia. 5
Squamous cell carcinoma occurs most frequently in sun-damaged, lightly pigmented skin and is the second most common malignant skin tumor in dogs. 3 Subungual squamous cell carcinoma has been reported to affect multiple digits of large-breed black dogs. 4 Squamous cell carcinomas are also the second most common malignant tumor of the oral cavity of dogs, where tumors of the caudal tongue and tonsil have high metastatic potential. 8 This report describes squamous cell carcinomas arising from the stratified squamous epithelial lining of the anal sac in five dogs.
Between 1 January 1990 and 30 June 2001, formalin-fixed tissues from the five dogs in this report were received by the Animal Reference Pathology Division of ARUP Laboratories in Salt Lake City, Utah. These dogs had a history of tumors involving the anal sac. Tissues were embedded in paraffin and hematoxylin and eosin–stained slides were prepared and evaluated by Animal Reference Pathology pathologists.
Dog No. 1, a 6.5-year-old spayed female Akita, was presented with a serosanguinous discharge from the duct of the left anal sac. During the next 9 days, cellulitis, which was nonresponsive to antibiotics and corticosteroids, developed. The perianal mass continued to increase in size. A biopsy was performed to differentiate between resistant infection and neoplasia. Microscopic examination of the tissue revealed squamous cell carcinoma with associated pyogranulomatous inflammation. The patient was referred to a surgeon who gave an unfavorable prognosis, and the owner elected euthanasia.
Dog No. 2, a 14-year-old female Cocker Spaniel–Poodle Cross, was presented with a mass in the area of the right anal sac. The right anal sac was surgically excised, and a diagnosis of squamous cell carcinoma was made. One and a half months after surgery two 1-cm tumors developed at one end of the incision line. Surgical removal was recommended but was not done. Four months after surgery there was evidence of stricture formation in the area, resulting in blockage of the bowel. One month later the owner elected euthanasia.
Dog No. 3, a 7-year-old spayed female Beagle, was presented with a 1-cm mass in the area of the left anal sac. The mass was removed and histologically diagnosed as a squamous cell carcinoma arising from the epithelial lining of the anal sac (Figs. 1, 2). Two months after surgery, a small nodule was noted in the area. This small nodule persisted without any change. Seven months after surgery, a radiograph of the pelvis was normal, and there was no clinical evidence of tumor recurrence.
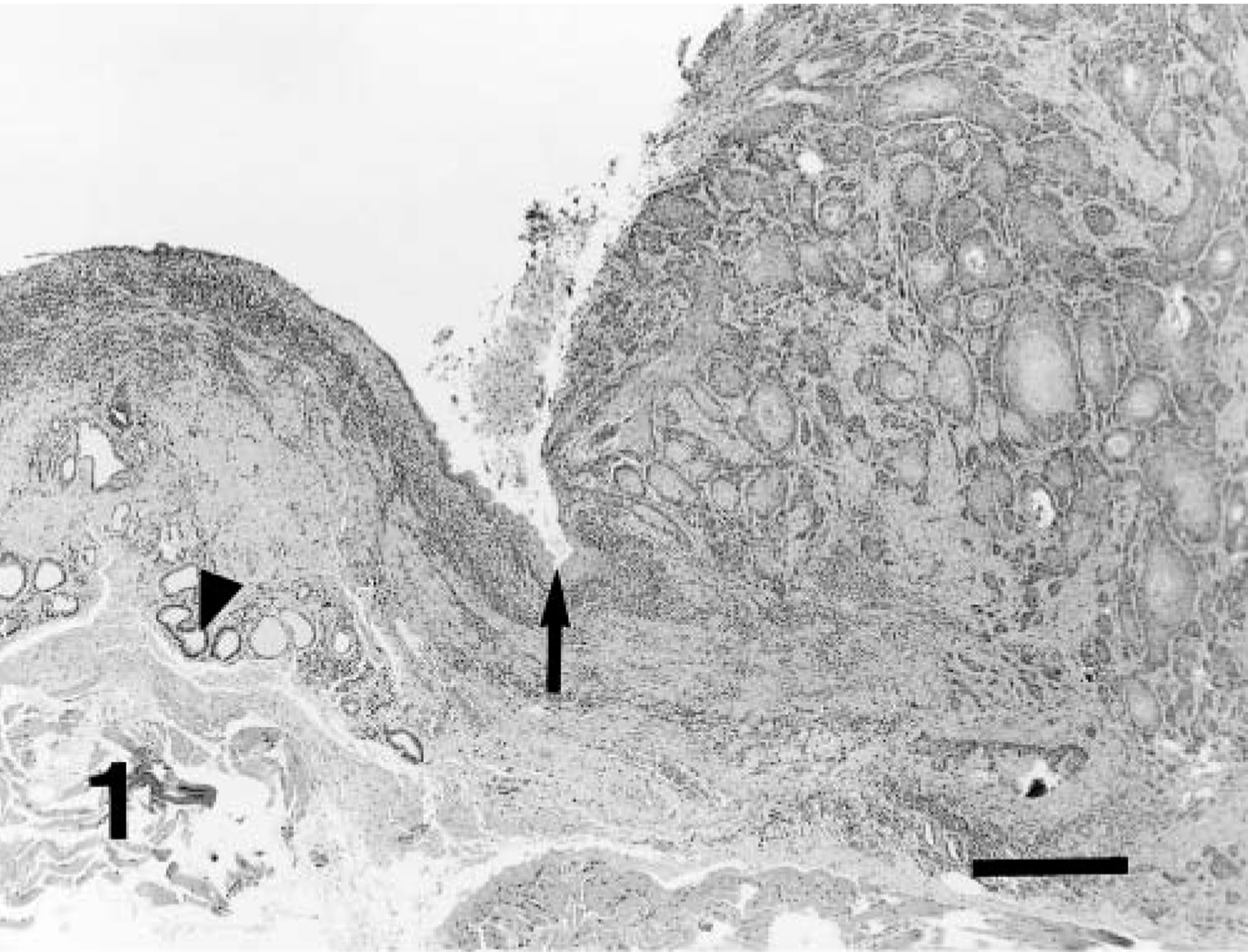
Squamous cell carcinoma of anal sac; dog No. 3. Section of anal sac demonstrating transition of lining from normal stratified squamous epithelium to squamous cell carcinoma (arrow). Note the apocrine anal sac glands at periphery (arrowhead). HE. Bar = 360 μm.
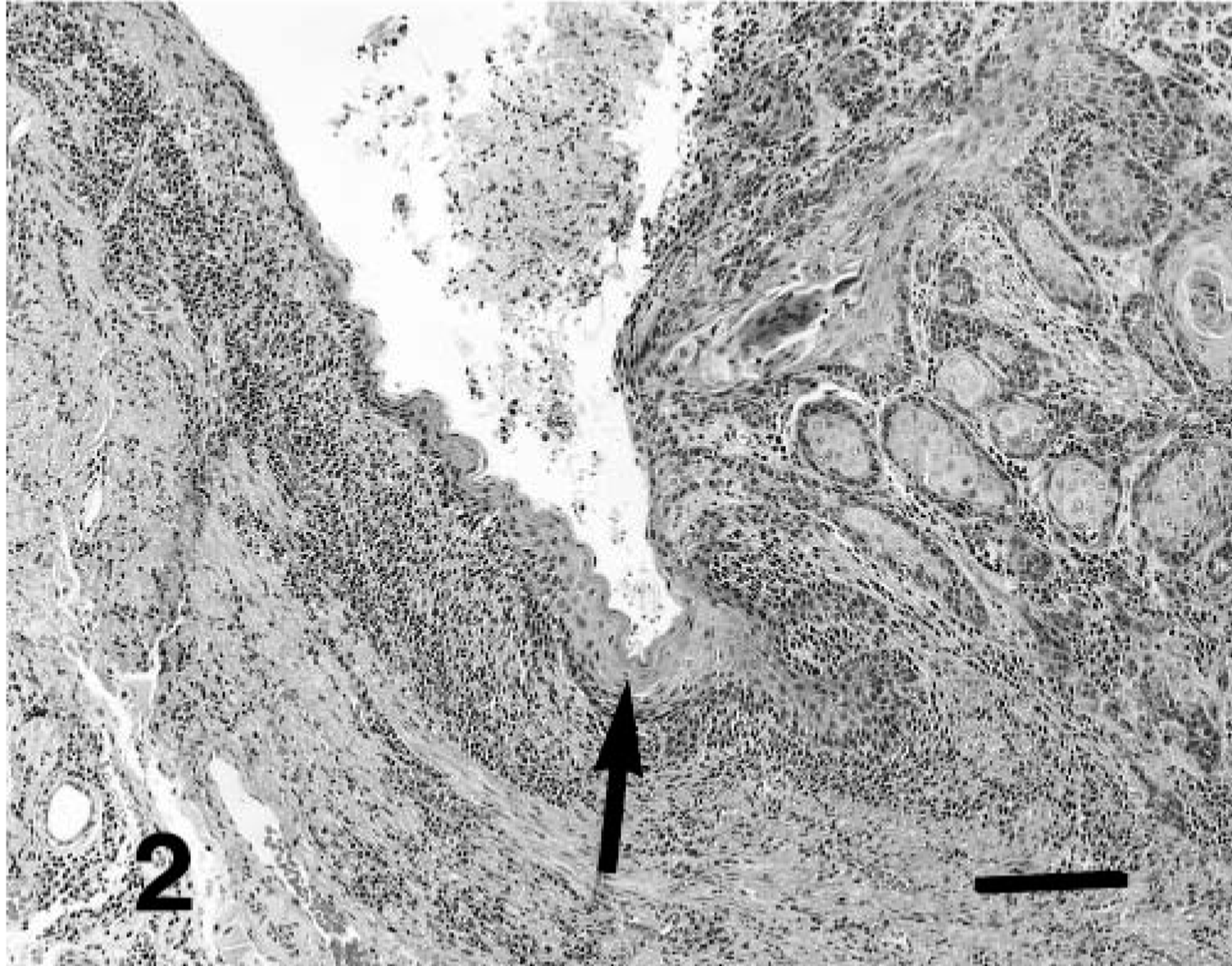
Squamous cell carcinoma of anal sac; dog No. 3. Higher magnification of Fig. 1 demonstrating transition of lining of anal sac from normal stratified squamous epithelium to squamous cell carcinoma (arrow). HE. Bar = 140 μm.
Dog No. 4, a 12.5-year-old spayed female Shetland Sheepdog, was presented with a hemorrhagic discharge from the left anal sac. Tissue in the area was thick and firm. There was no response to antibiotic treatment. The left anal sac was removed 2.5 months after initial presentation, and squamous cell carcinoma was diagnosed (Fig. 3). A mass with associated discharge was again present in the area 1.5 months later. Cytologic examination was consistent with recurrent squamous cell carcinoma. The recurrent mass demonstrated aggressive growth, doubling in size in 1 week, eventually reaching a size of 4 cm. The owner declined referral for further treatment. Three weeks after presentation for recurrence, the owner elected euthanasia.
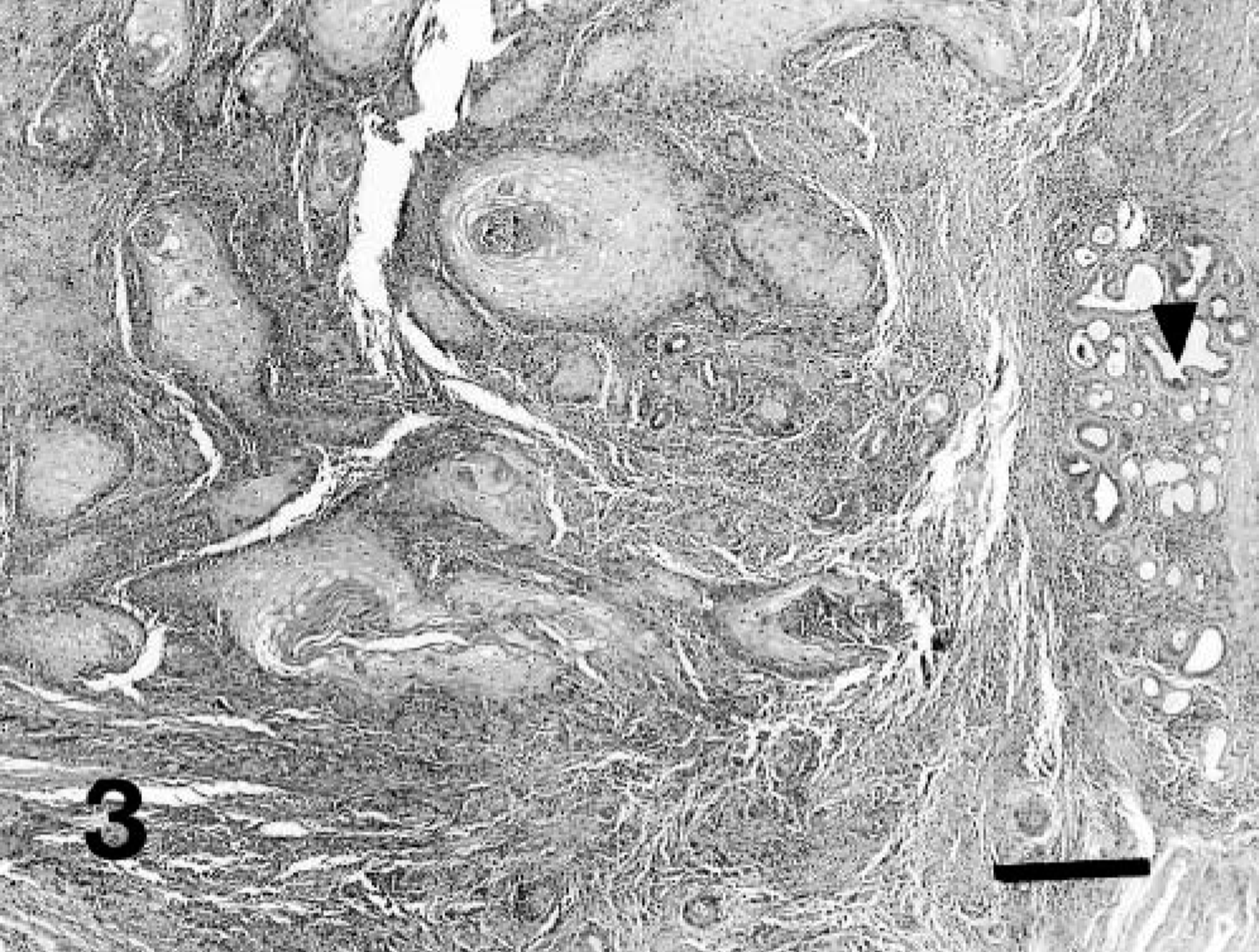
Squamous cell carcinoma of anal sac; dog No. 4. Section demonstrating invasive nests and cords of squamous cell carcinoma arising from lining of anal sac. Note apocrine anal sac glands at periphery (arrowhead). HE. Bar = 360 μm.
Dog No. 5, a 10-year-old castrated male Shih Tzu, presented with chronic thickening of the left anal sac region. There was a history of a draining tract in the area. The left anal sac was excised and diagnosed as squamous cell carcinoma. The mass extended into the rectal wall, and there was concern that the initial excision was not complete. Two months later, a 3–4 cm mass suspected to be tumor regrowth was present on the left floor of the rectum. The patient was straining to defecate and was started on stool softener. More aggressive surgery was recommended, but the owner declined because of the age of the patient. After 1 month, the patient was again examined. The mass had continued to enlarge both cranially and circumferentially. Five days later, the owner elected euthanasia.
Microscopically, the tumors from all five patients displayed histologic features typical of squamous cell carcinoma. In better-differentiated areas, intercellular bridges and foci of keratin formation were evident. In more anaplastic areas, tumor cells were less stratified and nuclei displayed greater variation in size and shape with many large vesicular nuclei observed. A high mitotic index was present, with two to four mitotic figures seen in many high-power fields. Variably sized nests and cords of tumor cells, and even individual tumor cells, extensively infiltrated the supporting stroma. In dog No. 1, only a core biopsy was obtained for diagnostic purposes. In the other four cases, the entire anal sac and surrounding tissue were excised. In the latter cases, a central lumen could be observed, and surrounding tissue contained structures consistent in appearance with anal sac apocrine glands. Dog No. 3 seemed to be in an earlier stage at the time of diagnosis because the exact point of origin of the tumor from the lining of the anal sac could still be seen histologically (Figs. 1, 2), and the other four cases had more extensive stromal infiltration by the time diagnosis was made (Fig. 3). Lymphatic invasion was evident in tissue sections from dog No. 2. Lymphatic invasion was suspected in dog No. 1, but apparent lymphatic vessels involved were not completely lined by endothelial cells, and thus were not definitive.
Neoplasms involving the perianal area and squamous cell carcinomas involving various areas of skin are common in dogs. However, with the exception of an abstract that included three of the dogs in this report, 2 to the authors' knowledge, this is the first report of squamous cell carcinoma arising from the epithelial lining of the anal sac.
Origin of tumors from the internal lining of the anal sac may not be detected early, and this may allow considerable local infiltration before diagnosis is made. The perianal location of these tumors predisposes the affected patients to interference with normal defecation.
In Dog No. 3, the point of origin from the epithelial lining of the anal sac was still histologically evident (Figs. 1, 2), possibly indicating an early stage of tumor development. Surgical removal of this tumor resulted in an apparently favorable outcome. In the other cases, at the time of diagnosis, the point of origin could no longer be identified, more extensive infiltration was present (Fig. 3), and the outcomes were unfavorable.
Cutaneous squamous cell carcinomas in dogs are reported to be locally invasive but slow to metastasize. 6 This is consistent with the apparent behavior of these squamous cell carcinomas arising from the lining of the anal sac. No metastases were detected, but early euthanasia was elected for four of the five dogs because of problems associated with local infiltration of the tumors. In the remaining case there was no evidence of tumor recurrence or metastasis 7 months after surgical removal but further follow-up was not available. Although the number of dogs in this report is too small to definitively assess the biologic behavior of anal sac squamous cell carcinomas, based on these few cases, a guarded to poor prognosis seems appropriate depending on early detection and completeness of excision.