
Abstract
A perianal mass in a 15-year-old domestic shorthair cat with a history of a firm, painful swelling in the left ventrolateral perianal region was surgically excised and submitted for light microscopic evaluation. Histologically, this was a poorly demarcated, unencapsulated, multilobulated neoplasm that invaded surrounding perirectal skeletal muscle bundles. Lobules were composed of sheets and acinar arrangements of cuboidal to round neoplastic epithelial cells with scant to moderate eosinophilic to amphophilic cytoplasm and a round or oval nucleus with coarse chromatin. Mitotic figures were 2 per 40 x objective field. Acinar lumina sometimes contained eosinophilic proteinaceous material or cell debris. These microscopic features are consistent with anal sac gland carcinoma. This is the second report of this neoplasm in a cat.
Perianal tumors are common in dogs, with hepatoid gland adenoma most commonly reported. 2 Anal sac gland carcinoma, although less common in dogs, is also well recognized. 5 In contrast, perianal tumors are rare in cats, and to the author's knowledge, only 1 report of feline anal sac gland carcinoma is documented in a 12-year-old neutered male Siamese cat. 8 Another report of perineal apocrine gland adenocarcinoma in a 15-year-old castrated male domestic shorthair cat does not specify an anal sac location of the tumor. 4
A surgical biopsy from a 15-year-old spayed female domestic shorthair cat with a history of a firm, painful swelling in the left ventrolateral perianal region was surgically excised and submitted for light microscopic evaluation. The specimen was a firm, irregular, pale tan, subcutaneous mass (1.8 × 1.1 × 1.0 cm) that, on cut section, contained a moderate quantity of viscous fluid material. Preoperative hematologic and serum biochemical parameters were within normal limits.
The mass was fixed in 10% neutral buffered formalin, routinely processed, and embedded in paraffin according to accepted histologic technique. Five-micron-thick sections were stained with hematoxylin and eosin (HE) for microscopic examination. Histopathologically, a portion of the stratified squamous epithelial lining of the anal sac was seen in one section, and the subjacent tissue architecture was effaced and expanded by a poorly demarcated, unencapsulated, and multilobulated neoplasm (Fig. 1). The lobules were composed of neoplastic epithelial cells that formed solid sheets, nests, and acinar structures separated by a fine anastomosing fibrovascular connective tissue stroma (Fig. 2). Neoplastic cells in acini sometimes formed multiple layers that were crowded and disorganized against the basement membrane. Individual neoplastic cells were of slightly variable shape and ranged from attenuated cuboidal to round or polygonal with indiscrete borders and scant to moderate pale eosinophilic to amphophilic cytoplasm. Nuclei were predominantly round or oval, with coarse stippled chromatin and often 1 or 2 prominent nucleoli. Mitoses were 1 or 2 per 40× objective field and occasionally atypical. Acinar lumina varied from small to ectatic and sometimes contained variable quantities of pale eosinophilic proteinaceous fluid material or necrotic cell debris. Neoplastic cells invaded adjacent perirectal skeletal muscle bundles and extended to the surgical margins of the specimen. A moderate amount of desmoplasia was present. Multiple foci of necrosis with admixed infiltrates of neutrophils, lymphocytes, and plasma cells were also interspersed throughout the sections. Neoplastic invasion of lymphatic or blood vessels was not seen.
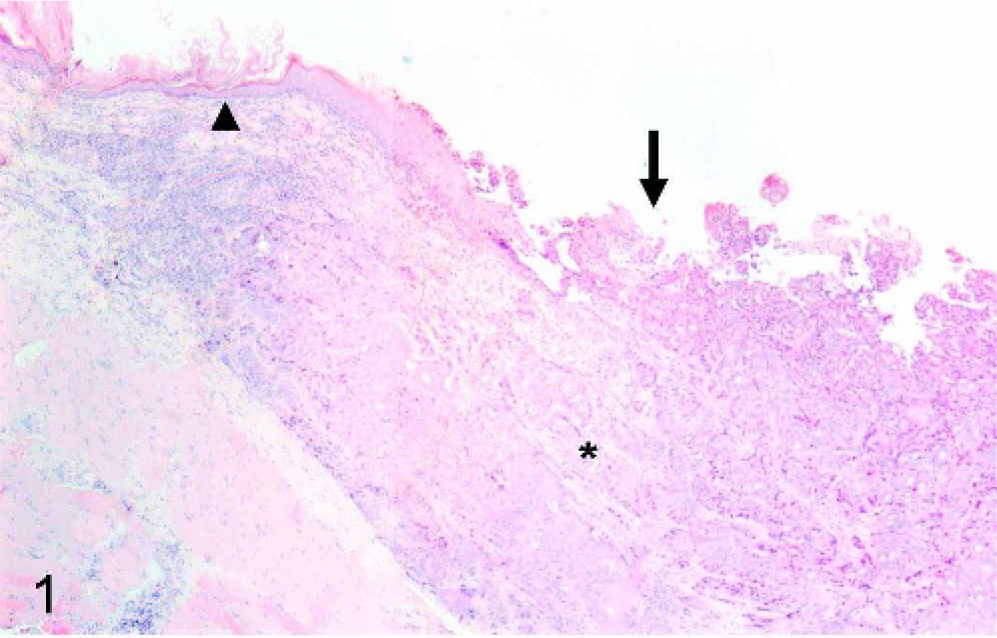
Anal sac gland carcinoma; cat. An unencapsulated proliferation of neoplastic apocrine glands (asterisk) is seen adjacent to the anal sac epithelium (arrowhead), which is regionally ulcerated (arrow). HE.
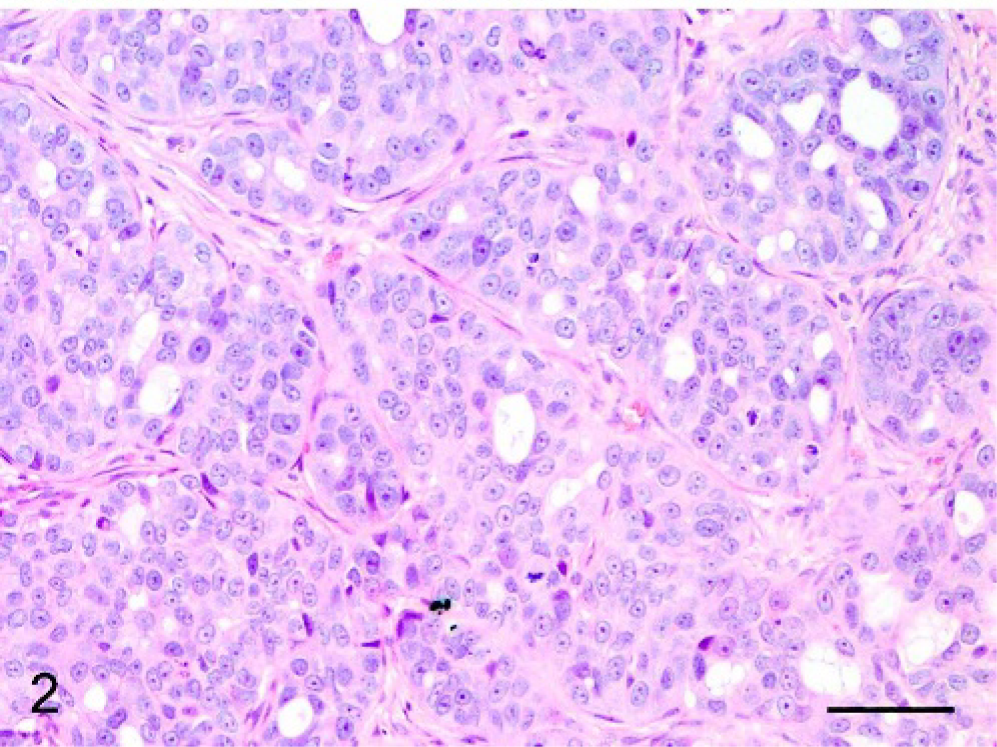
Anal sac gland carcinoma; cat. Nests and acinar arrangements of neoplastic cells separated by an intervening fine anastomosing fibrovascular connective tissue stroma. HE. Bar = 120 μm.
Anal sac gland carcinoma is reported to be the most common malignant perineal neoplasm in dogs, accounting for approximately 2% of canine skin tumors. 5 It predominantly affects animals between 5 and 15 years old, with peak occurrence between 7 and 12 years of age. 5 This neoplasm is usually unilateral and arises from the apocrine glands surrounding the fundus of the anal sac. 7 Some reports have suggested it to be more common in older female dogs, 7, 10 whereas others document no apparent gender predisposition. 1, 6
This highly malignant neoplasm in dogs frequently invades local tissues, and metastasis is an early feature of the disease that is often present at the time of diagnosis. 1, 9, 10 Metastasis commonly occurs by lymphatic drainage to regional sacral, iliac, and lumbar lymph nodes, with more distant spread less commonly to the lung, liver, and spleen 1, 9, 10 and rarely to other sites. 3 This neoplasm can occur as an occult disease in dogs, with careful rectal palpation required for diagnosis in such cases. 10 In some instances, it might not be detected until an animal presents with systemic signs, such as weakness, vomiting, anorexia, polyuria, and polydipsia because of concurrent humoral hypercalcemia of malignancy. 9, 10 Hypercalcemia has been attributed to production of a parathyroid hormone–related protein by the neoplastic cells, and although its documented incidence is variable, it has been reported in up to 51% of dogs with anal sac gland carcinoma. 1 Complete surgical excision of these neoplasms is frequently difficult because of their invasive nature and the associated host desmoplastic response, and recurrence is common. 7, 10
Histologic association with the anal sac and microscopic features of the neoplasm in this cat are consistent with a diagnosis of anal sac gland carcinoma. Its clinical presentation as a perianal swelling was similar to the way some cases present in dogs, and its histologic morphology and invasion of surrounding tissue was also comparable to the canine lesion. 5 Hypercalcemia, although documented in some cases in dogs, 9, 10 was not a feature in this cat at the time of surgical excision of the mass. Although the cat was presented to the clinician for an initial postoperative examination, additional follow-up clinical information is unavailable because she was not presented for further examination. Neoplastic cells did extend to the surgical margins, however, and this lesion was considered incompletely excised with recurrence a likely possibility. To the author's knowledge, this is only the second documented report of anal sac gland carcinoma in a cat.