
Abstract
An intestinal carcinoid with multiple metastases was identified in a 5-year-old male Shih Tzu with a clinical history of anemia, fatigue, anorexia, vomiting, intermittent diarrhea, intestinal bleeding, and progressive emaciation. There was a yellowish-white mass 15 mm in diameter in the anterior jejunum and white nodules consistent with metastases in many organs. Histopathologically, the mass consisted of neoplastic cells arranged in lobules, trabeculae, or closely interdigitating islands of cells. Neoplastic cells were generally polygonal with round hyperchromatic nuclei, modest amounts of eosinophilic cytoplasm, and eosinophilic cytoplasmic granules. Mitoses were common. Rosette formations of tumor cells were apparent in metastatic tumors. Immunohistochemically, tumor cells stained positive for cytokeratin 13, synaptophysin, protein gene product 9.5, neuron-specific enolase, chromogranin A, calcitonin gene-related peptide, serotonin (5-HT), and Leu-7. Serum 5-HT concentrations for this dog were increased 10-fold compared with those of normal dogs. All findings were consistent with a diagnosis of a malignant intestinal carcinoid.
Neuroendocrine cells are embryologically derived from the gut and are widely distributed in various tissues such as the tracheobronchial tree, liver, pancreas, and genitourinary system. 5 Gastrointestinal (GI) carcinoids, derived from neuroendocrine cells in the GI tract, are relatively uncommon neoplasms. Cases of GI carcinoids have been reported in humans and animals. 5 , 6 , 8 , 13 GI carcinoids in humans are characterized by slow growth and occasional metastasis. These tumors may be associated with a pattern of clinical symptoms referred to as the carcinoid syndrome. This pattern of symptoms includes diarrhea, episodic flushing, bronchospasm, cyanosis, telangiectasia, and skin lesions. 5 Cases of GI, hepatic, and pulmonary carcinoids have been reported in dogs. 6 , 8 , 9 , 12 , 13 Diagnoses in these cases were confirmed by histopathologic and electron microscopic features of the tumor cells; immunohistochemical characterization of canine intestinal carcinoids has not been reported. 6 This report describes the histopathologic and immunohistochemical characteristics of an intestinal carcinoid with multiple metastases in a 5-year-old male Shih Tzu.
This dog had a clinical history of anemia, fatigue, anorexia, vomiting, intermittent episodes of diarrhea, and intestinal bleeding for a 4-month period; signs were associated with progressive emaciation. Hematocrit (Ht), hemoglobin (Hb), and platelet count fluctuated but remained below normal reference values during the 4-month period. Seven days before death, hemogram values were Hb = 2.0 g/100 ml; Ht = 8.1%; platelet count = 51,610/ml; and leucocyte counts = 27,300/ml. Abdominal radiographs revealed a mass of soft tissue density in the small intestine and large amounts of gas throughout the intestines. Despite two whole-blood transfusions, the animal died.
Necropsy revealed a yellowish-white, semifirm mass measuring 15 mm in diameter in the wall of the anterior jejunum causing stricture of the intestinal lumen (Fig. 1). The mucosal surface was ulcerated and hemorrhagic; this appeared to account for the intestinal bleeding and anemia observed clinically. Multiple white nodules measuring 2–13 mm in diameter were evident in the liver, lungs, heart, esophagus, trachea, tonsil, and mesenteric lymph nodes.
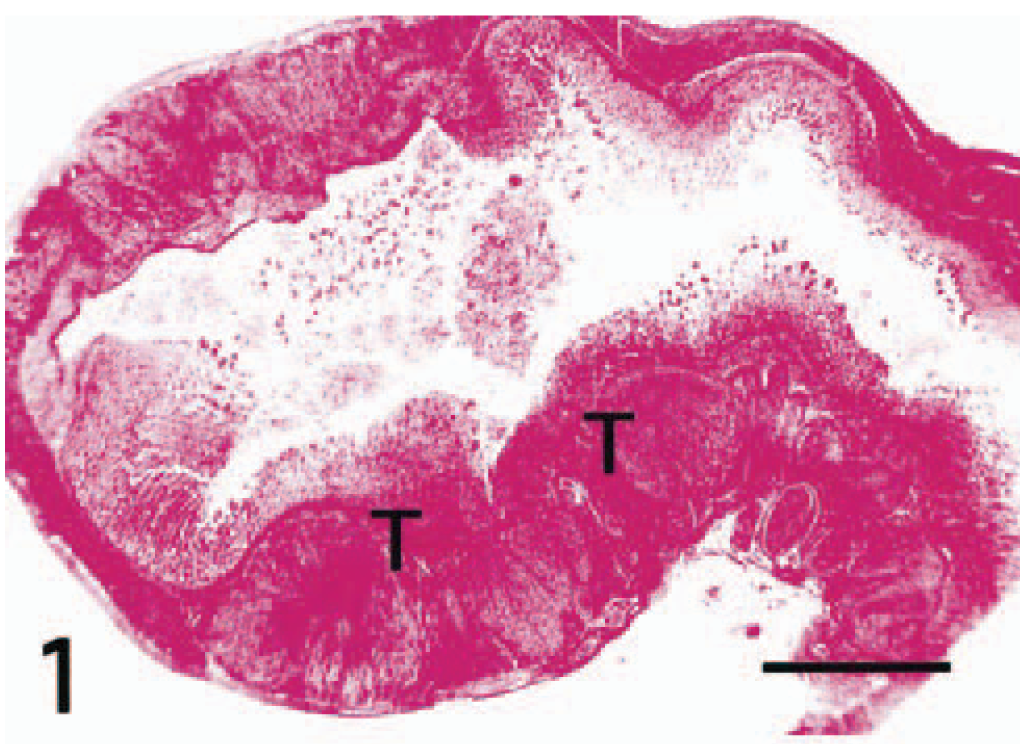
Jejunal carcinoid; Shih Tzu. Primary tumor (T) cells in the jejunal wall are arranged in lobules, trabeculae, or closely interdigitating islands. HE. Bar = 5 μm.
Tissue samples from the primary tumor in the anterior jejunum and metastatic nodules in the liver, lungs, heart, esophagus, trachea, tonsil, and mesenteric lymph nodes were fixed in 10% formalin, routinely processed for paraffin embedding, sectioned at 4 μm, and stained with hematoxylin and eosin (HE) and by Grimelius' method. Microscopically, the neoplastic cells of primary tumor in the jejunal wall were arranged in lobules, trabeculae, or closely interdigitating islands of cells. Neoplastic cells were separated by variable amounts of fibrovascular stroma (Fig. 2). The neoplasm extended from the lamina propria to the serosal surface of the jejunum and caused disruption in normal intestinal architecture.
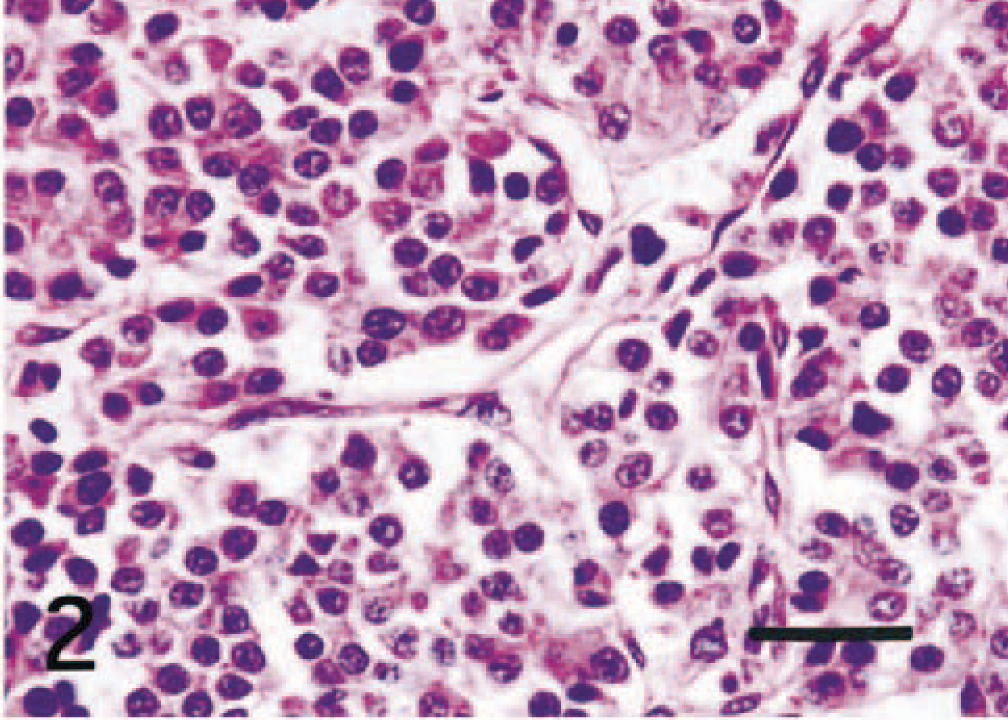
Jejunal carcinoid; Shih Tzu. Neoplastic cells are polygonal with round hyperchromatic nuclei and modest amounts of eosinophilic cytoplasm and are separated by fine fibrovascular stroma. HE. Bar = 20 μm.
Neoplastic cells were generally polygonal with round hyperchromatic nuclei and modest amounts of eosinophilic cytoplasm containing eosinophilic granules (Fig. 2). These cytoplasmic granules were stained by Grimelius' method. Mitotic figures ranged from 7 to 11 per high-power field. Neoplastic cells were frequently present in blood vessels and lymphatics in the lamina propria, tunica submucosa, and tunica muscularis.
In the liver, metastatic tumor foci were seen in the hepatic parenchyma (Fig. 3) and portal veins. Metastatic tumors were also present in pulmonary arteries, alveolar wall, and pulmonary alveoli of the lungs. In the heart, metastatic tumors were found in the branches of coronary arteries and interstitial connective tissues of the atrial myocardium. Multiple metastatic tumors were seen in blood vessels between the esophagus and the trachea. One tumor nodule extended from the lamina propria of the esophagus through the wall of the trachea into the tracheal lumen. Metastatic tumor cells were found in the submucosal layer of the tonsil. Tumor cells in the lung, heart, esophagus, and trachea were occasionally arranged in rosette (Fig. 4).
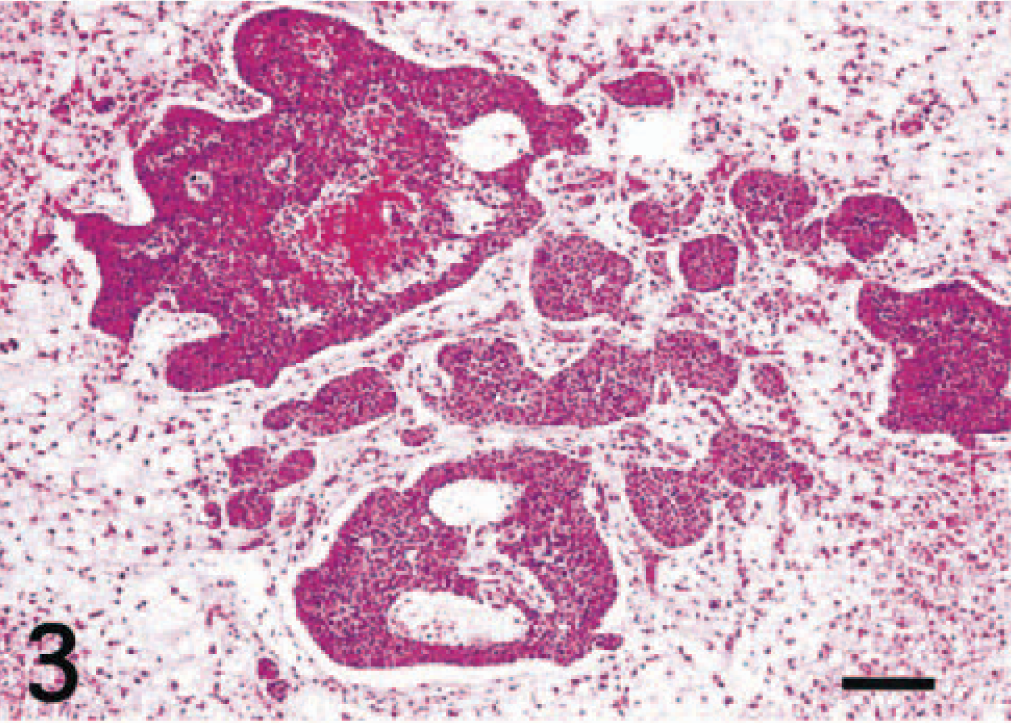
Liver; Shih Tzu. Metastatic carcinoid cells are arranged as islands and cords in the hepatic parenchyma. HE. Bar = 100 μm.
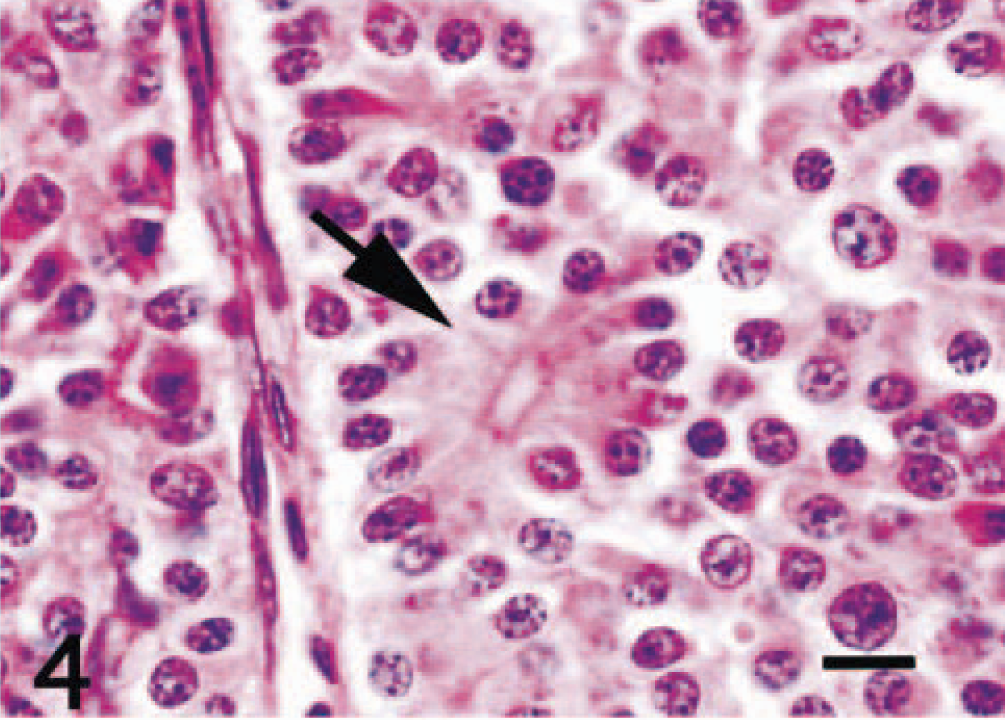
Lung; Shih Tzu. Metastatic carcinoid. Neoplastic cells are polygonal with round hyperchromatic nuclei and variable amount of eosinophilic cytoplasm. The arrow indicates a tumor rosette. HE. Bar = 10 μm.
Sections from the primary neoplasm and metastatic nodules were immunohistochemically stained by the avidin–biotin–peroxidase complex (ABC) procedure (Vectastain Elite ABC Kit; Vector Laboratories, Burlingame, CA) and examined microscopically. Details of the specific antisera used and staining results are summarized in Table 1. Deparaffinized sections were blocked for endogenous peroxidase in 3% H2O2 for 10 minutes. All sections were incubated with primary antibody at 4 C for 16 hours, with biotinylated secondary antibody for 30 minutes at room temperature, and with avidin peroxidase conjugate for 30 minutes. Sections were developed in 0.05% 3,3′-diaminobenzidine solution. For immunohistochemical control purposes, jejunal tissue from a normal dog was used. Control procedures included the use of excess antigen in relation to immune sera and nonimmune sera instead of the primary antibody; omission of the primary antibody resulted in the absence of specific reaction.
Results of immunohistochemical staining of the intestinal carcinoid of a Shih Tzu.
∗ +++ = positive signals in most of the neoplastic cells; ++ = positive signals in many neoplastic cells; + = positive signals in a few neoplastic cells; − = negative.
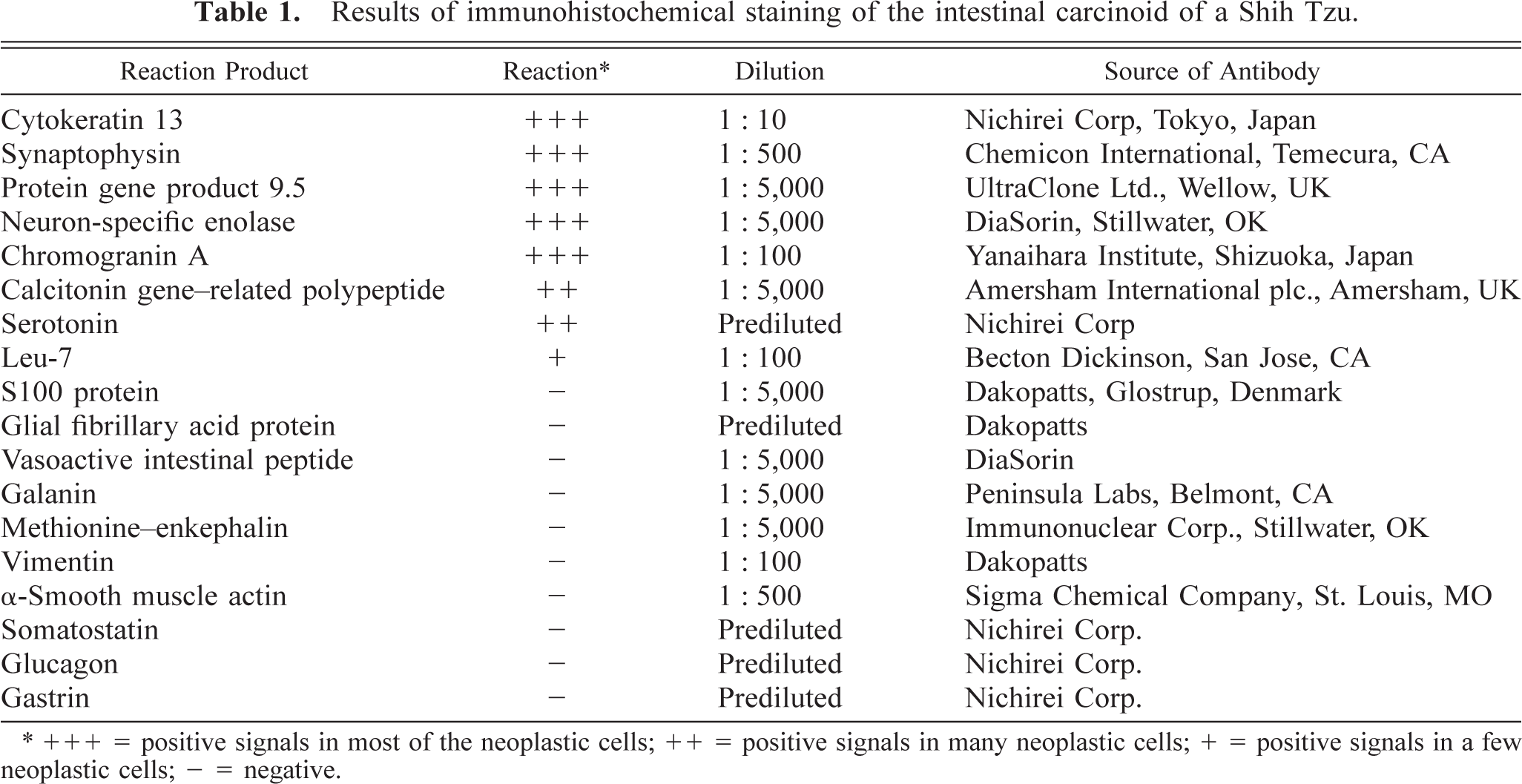
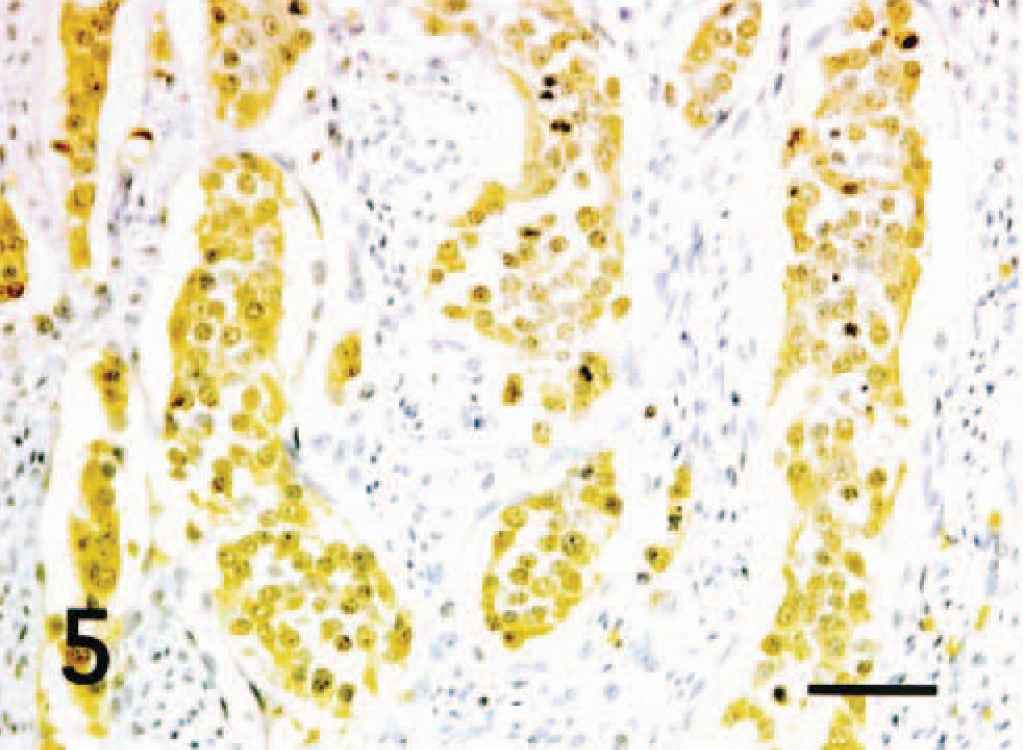
Most of the neoplastic cells in the primary neoplasm and metastases were intensely immunoreactive for cytokeratin 13, synaptophysin (SYN), protein gene product 9.5 (PGP 9.5), neuron-specific enolase (NSE), and chromogranin A (CGA) (Fig. 5). In addition, many neoplastic cells were immunoreactive for calcitonin gene–related peptide (CGRP) (Fig. 6) and serotonin (5-HT). A small number of neoplastic cells reacted with Leu-7. Tumor cells were negative for glial fibrillary acid protein, S100 protein, vasoactive intestinal peptide (VIP), galanin (GAL), methionine–enkephalin (ME), vimentin, α-smooth muscle actin, somatostatin, glucagon, and gastrin.
Jejunal carcinoid; Shih Tzu. Most of the neoplastic cells react positively to chromogranin A. ABC method with Mayer's hematoxylin counterstain. Bar = 20 μm.
Jejunal carcinoid; Shih Tzu. Many neoplastic cells react positively to calcitonin gene–related peptide. ABC method with Mayer's hematoxylin counterstain. Bar = 20 μm.
Concentrations of serum 5-HT were determined for this dog and four clinically normal dogs using high-performance liquid chromatography, as previously described. 10 The serum 5-HT of this dog was 2,386 nmol/liter. This value was approximately 10-fold greater than concentrations in the clinically normal dogs (range, 10–227 nmol/liter).
Morphologic and immunohistochemical features of the primary tumor and metastatic nodules in this dog were consistent with a malignant intestinal carcinoid. Immunohistochemical evaluation using antibodies against various neuropeptides has been useful in confirming the endocrine cell origin of neoplasm in humans. 1–4 , 10–12 , 14 CGA and NSE were usually detected in neoplastic cells of GI and pulmonary carcinoids in humans. 1–4 , 11 Furthermore, the neoplastic cells are often positive for CK, 5-HT, SYN, substance P, VIP, neuropeptides Y, ME, CGRP, calcitonin, PGP 9.5, Leu-7, GAL, somatostatin, and glucagon. Patients with carcinoid often have elevated plasma levels of 5-HT, 7 somatostatin, 7 pancreatic polypeptide, 7 CGRP, 14 and gastrin, 3 , 11 consistent with the production of 5-HT and various neuropeptides by the neoplastic cells.
Human carcinoids are typically diagnosed in elderly patients, the mean age at the time of presentation being 62 years (range, 13–93 years). 3 In humans, small intestinal carcinoids occur 6.5 times more frequently in the ileum than in the jejunum. 3 Intestinal carcinoids seem to affect dogs that are at least 9 years old. 6 , 8 , 13 Intestinal carcinoids usually occur in the large intestine (rectum, colon, and cecocolic junction); they are rarely found in the stomach and duodenum. 6 The jejunal location of the carcinoid in this case is unusual because no jejunal carcinoids have previously been reported in dogs. 6
Metastasis of carcinoids is common in domestic animals and demonstrates the malignancy of the tumor. In dogs, small intestinal carcinoids frequently spread to the lung and pleura, liver, regional lymph nodes, and pancreas. 6 In the present case, metastases were found in the liver, lungs, heart, esophagus, trachea, tonsil, and regional lymph nodes. These metastatic tumor locations suggested that the intestinal carcinoid spread through the blood and lymph vessels.
Carcinoid tumors of the GI tract have differentiation characteristics of the neuroendocrine system. They are capable of secreting peptides and amines (5-HT, somatostatin, gastrin, and histamine) produced by their normal counterparts. The most commonly secreted hormone is 5-HT. 6 Thus serum 5-HT concentrations can provide a useful diagnostic parameter to confirm carcinoid tumors. Diarrhea is thought to be caused by 5-HT. 5 In our study, clinical signs such as intermittent episodes of diarrhea before death may have resulted from high serum 5-HT.