
Abstract
An 11-year-old Fox Terrier dog was evaluated for a 10-month history of progressive exophthalmia and visual deficits in the right eye. Ophthalmologic examination revealed severe corneal fibrosis and pigmentation, which obscured examination of the anterior chamber of the right eye. There was decreased retropulsion of the right eye. Neurological examination revealed an absent menace response bilaterally. Pupillary light reflex was normal in the left eye. Due to the corneal pathology, pupillary light reflex was unable to be evaluated in the right eye. A retrobulbar mass with heterogeneous echotexture was identified using ultrasonography. Cytological evaluation of a fine-needle aspirate of the mass disclosed a neoplastic cell population consisting of round to polygonal cells with lightly basophilic to gray cytoplasm and round to ovoid nuclei having a coarse granular chromatin pattern. Magnetic resonance imaging disclosed a right-sided retrobulbar mass that extended through the optic canal and was contiguous with an extra-axial mass in the ventral right rostral and middle cranial fossae. The mass displayed homogenous and strong contrast enhancement. Following exenteration, histological examination of the retrobulbar mass was consistent with meningioma. Immunohistochemically, tumor cells stained positive for vimentin (cytoplasmic) and E-cadherin (membranous), and negative for S100, pancytokeratin, and cytokeratins AE1 and AE3.
In the dog, pathology involving the anatomic structures of the orbit may be the result of infectious, inflammatory, and neoplastic disease. Orbital infections occur secondary to foreign body migration, 18,33 extension from apical tooth root abscesses, 29 sinonasal disease, 17,26 or osteomyelitis of the bones comprising the orbit and calvaria. 35 Alternatively, orbital infection may develop from hematogenous spread. 34 Typically, orbital infection involves bacterial or fungal etiologies. 17,26 Inflammatory disease may primarily involve the optic nerve, as occurs with the ocular form of granulomatous meningoencephalitis. 8 In such cases, signs reflect nervous system involvement of the eye and/or brain, rather than orbital disease. Alternatively, inflammatory disease may arise from other tissues contained within the orbit. Focal inflammatory myopathies that may affect the orbit include masticatory muscle myositis and extraocular muscle myositis. 9,14 In cats, idiopathic sclerosing orbital pseudotumor has also been reported. 5 Orbital neoplasia may be divided into primary and secondary tumors. Primary tumors involve the anatomic structures contained within the orbit and the bony orbit itself, while secondary tumors represent metastasis or extension from surrounding anatomic structures (i.e., nasal tumors). 1 Of the primary orbital tumors, retrobulbar meningioma is a common nervous system tumor that arises from the meninges, which cover the optic nerve within the orbit. 24
Regardless of the disease process, clinical signs often consist of exophthalmia, decreased retropulsion of the globe, blindness, orbital swelling leading to a prolapsed globe, incomplete palpebral closure, strabismus, elevation of the membrana nictitans, pain on opening the mouth, visual deficits, and abnormalities in the pupillary light reflex (PLR). 31 Ophthalmic examination may disclose papilledema, retinal edema, and scleral indentation. 31 Secondary exposure keratitis also may occur. A presumptive diagnosis of orbital disease can be made based on clinical findings and imaging studies such as ocular ultrasound, computed tomography, or magnetic resonance imaging (MRI). 6,10,11,15,23 Given its high spatial and contrast resolution, MRI enables excellent assessment of the extent of disease within and extending from the orbit. 11 Despite this, MRI findings often lack specificity, which necessitates histologic evaluation of specimens obtained from a biopsy to establish a definitive diagnosis. 11 However, cytological evaluation of fine-needle aspirate specimens can be useful in the diagnosis of orbital diseases, such as abscesses, granulomas, or salivary gland pathology, and can potentially identify a malignant cell population. 7 The present report details the clinicopathologic data involving a retrobulbar meningioma in a dog and reviews the literature pertaining to orbital meningioma.
An 11-year-old female spayed Fox Terrier dog was referred for evaluation of a 10-month history of progressive, non-painful exophthalmia and visual deficits in the right eye. Initial signs began with mild protrusion of the right eye. Ophthalmic examination revealed papilledema, peripapillary retinal edema, and blindness oculus dexter (OD). Serologic testing for Rickettsia rickettsii and Ehrlichia canis was negative. Subsequent ocular examinations over the next 6 months revealed worsening of the exophthalmia and markedly decreased retropulsion of the right globe as well as optic nerve atrophy and indentation of the caudal aspect of the sclera OD in the nasodorsal quadrant. Additionally, corneal fibrosis and pigmentation developed secondary to exposure keratitis. As a result, the dog was referred to the University of Georgia, College of Veterinary Medicine Teaching Hospital (Athens, GA)
On presentation to the Veterinary Teaching Hospital, ophthalmic examination revealed marked exophthalmia, decreased retropulsion OD, and marked corneal fibrosis and pigmentation that prohibited examination of the anterior chamber. Neurologic examination revealed normal mentation, gait, postural reactions, and spinal reflexes. Menace response was absent in both eyes. Visual tracking and maze testing also was consistent with blindness. Indirect and direct PLR could not be evaluated OD given the marked corneal fibrosis and pigmentation. Direct PLR was positive in oculus sinister. Based on examination findings, an orbital or retrobulbar mass was suspected. Given the progression to bilateral blindness, extension into the cranial cavity was suspected. Differential diagnosis consisted of orbital neoplasia, infectious (retrobulbar abscess), or inflammatory disease.
A complete blood count, serum biochemistry, and urinalysis were indicative of anemia (35.9%, reference [ref.] interval: 36.6–59.6%), azotemia (blood urea nitrogen 90 mg/dl, ref. interval: 8.5–28.5 mg/dl; creatinine 1.9 mg/dl, ref. interval: 0.2–1.2 mg/dl), hyperphosphatemia (5.3 mg/dl, ref. interval: 2.9–5.1 mg/dl), 2+ proteinuria, and low urine specific gravity (1.016, ref. interval: >1.030). Ocular ultrasound of the right eye identified a large retrobulbar mass of mixed echogenicity and poorly defined caudal margins. The right optic nerve could not be identified. Ultrasonographic examination of the left eye and abdomen were normal. Thoracic radiographs revealed a well-defined, 2 cm in diameter, soft tissue nodule in the left caudal lung lobe.
Fine-needle aspirate and cytological evaluation of the retrobulbar mass revealed a neoplastic cell population of round to polygonal to occasionally elongated cells with a moderate amount of lightly basophilic to gray cytoplasm. Nuclei were round to ovoid containing 1 or more small distinct nucleoli and a coarse granular chromatin pattern. Moderate anisocytosis and mild to moderate anisokaryosis was present (Fig. 1).
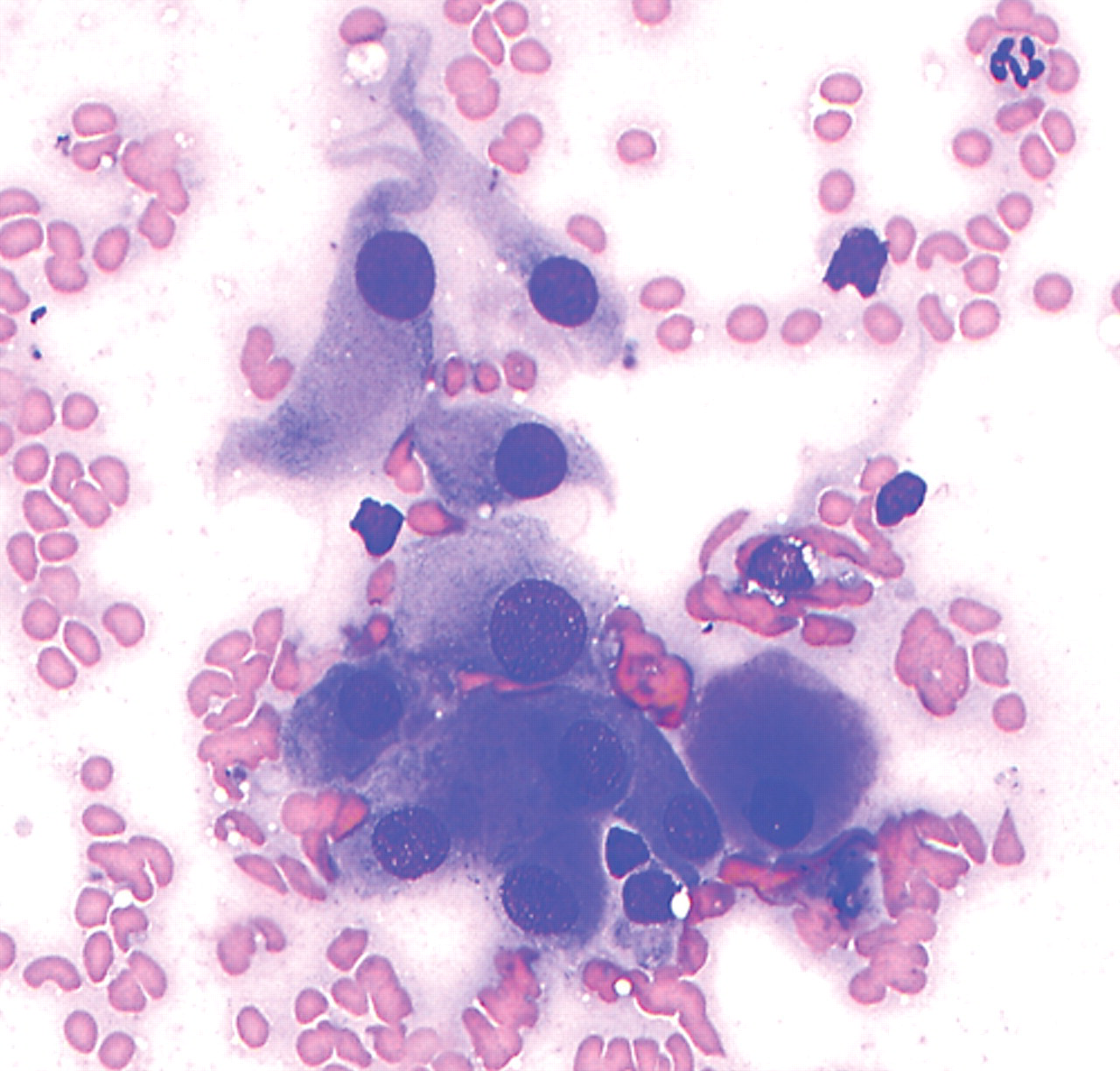
Photomicrograph of a fine-needle aspirate cytology of a retrobulbar mass in an 11-year-old female spayed Fox Terrier dog with a 10-month history of progressive exophthalmia. Note the several pleomorphic, polygonal to stellate neoplastic cells, which are present in small, loosely arranged aggregates. Note marked anisocytosis, moderate anisokaryosis, coarsely granular chromatin pattern, and small nucleoli. The cytological findings were consistent with a mesenchymal neoplasia. Wright stain.
Magnetic resonance imaging a of the head was performed using a 3.0T MRI unit. The following pulse sequences were obtained in the transverse, sagittal, and dorsal planes: T2-weighted (T2W), T2W fluid attenuated inversion recovery (T2W FLAIR), T1W FLAIR, T2*W, and short tau inversion recovery (STIR). The T1W FLAIR images also were obtained after intravenous administration of gadopentetate dimeglumine (0.1 mmol/kg). On MRI, a retrobulbar mass was identified filling the right orbit and resulting in rostral displacement of the eye and deformation of the caudal aspect of the globe. The mass extended through the right optic canal and was contiguous with an extra-axial mass in the right ventral region of the rostral and middle cranial fossae (Fig. 2). The retrobulbar mass as well as the extension within the optic canal and cranial cavity displayed uniform, strong contrast enhancement.
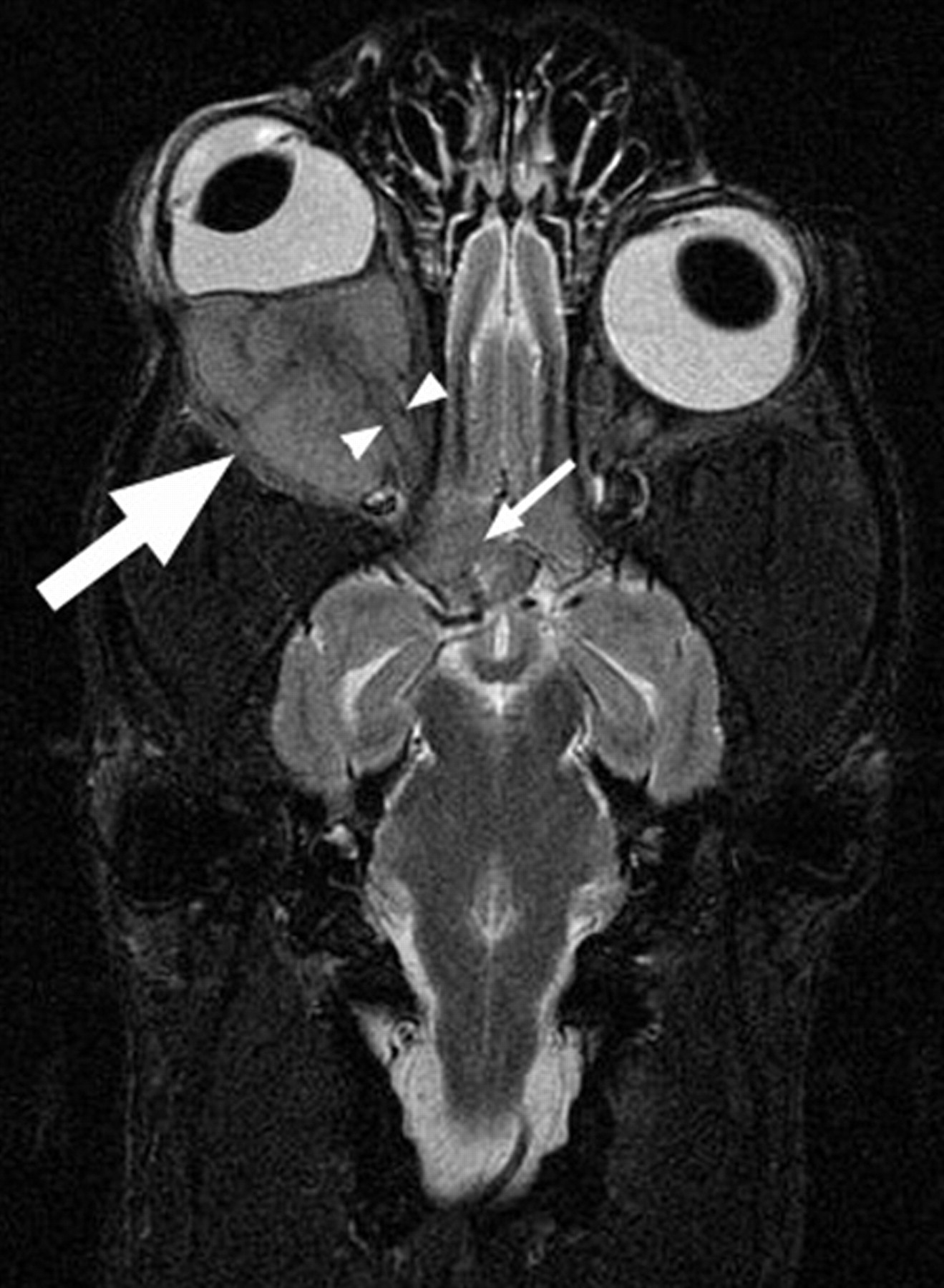
A dorsal plane short tau inversion recovery magnetic resonance imaging of the head. There is a lesion in the right orbit (large arrow), which results in compression and distortion as well as rostral deviation of the globe oculus dexter (exophthalmia). Within the caudal aspect of the mass, the optic nerve is visible (arrowheads). Additionally, extension of the lesion into the cranial cavity ventral to the diencephalon is evident (small arrow).
An exenteration of the contents of the right orbit was performed. Following surgery, the owners declined radiation therapy. Nine months post operatively, the dog is alive and blind in the left eye.
Grossly, the retrobulbar mass was white, soft, well circumscribed, and measured 2 cm × 1.5 cm × 1.5 cm. On cut surface, the mass was homogenous and soft and completely surrounded the optic nerve (Figs. 3, 4). A section of globe with the attached retrobulbar mass was examined histologically. An unencapsulated, infiltrative retrobulbar neoplasm, with a central area of myxomatous degeneration and peripheral extension into the periorbital adipose tissue and skeletal muscle, had obliterated the optic nerve through invasion by and replacement with neoplastic cells. Neoplastic cells were predominately epithelioid and were arranged in sheets, streaming cords, and occasionally concentric whorls that were separated by thin bundles of cells with a more spindle-shaped appearance, within a scant, hypocellular fibrovascular stroma. Neoplastic cells had abundant eosinophilic cytoplasm. The hyperchromatic nuclei were round to oval to occasionally elongate, with a finely stippled chromatin pattern and prominent single nucleoli (Fig. 5).
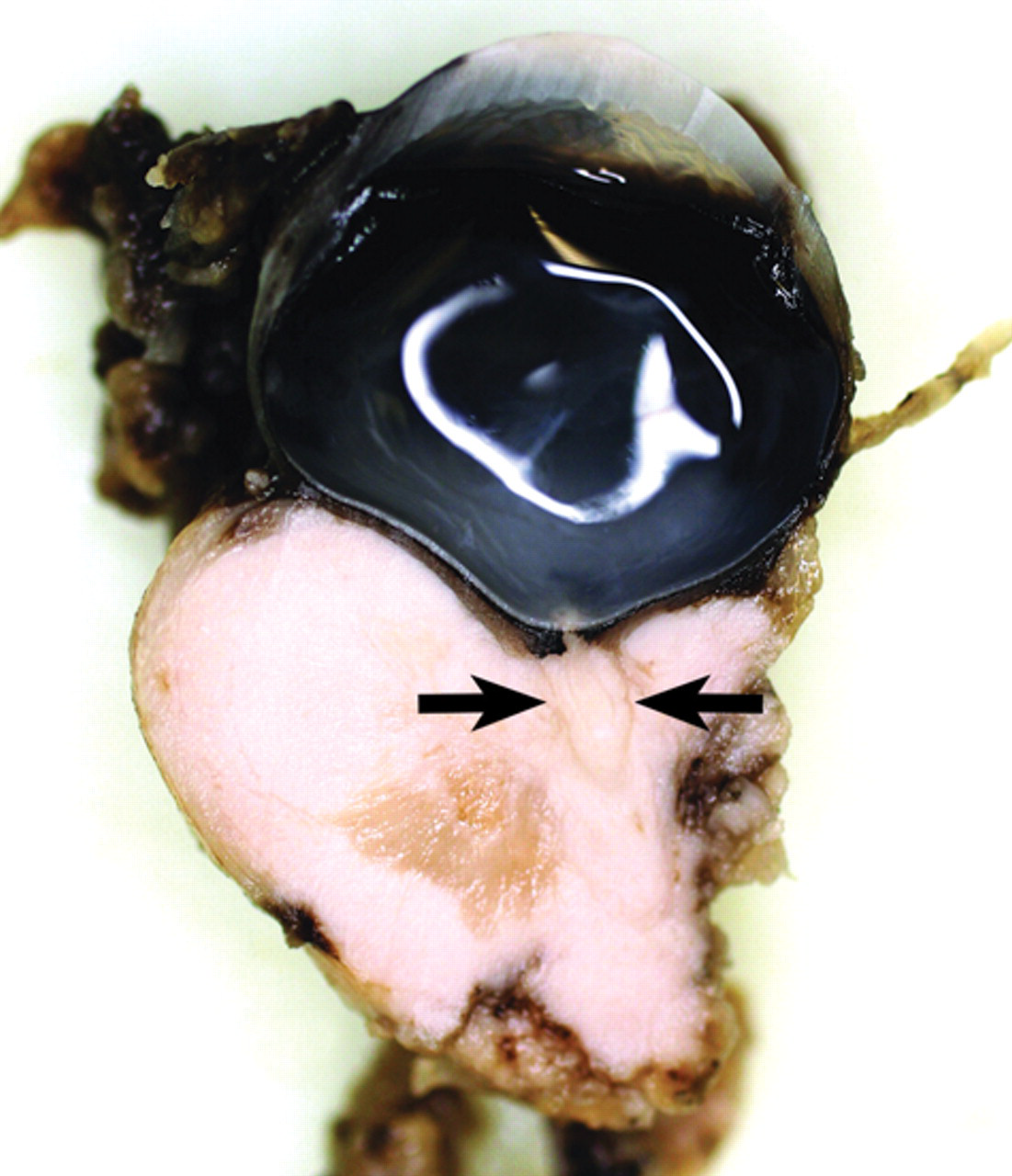
Photograph of the retrobulbar mass seen on magnetic resonance imaging in Figure 2. The photograph shows the cut surface of a dorsal, longitudinal section made of the globe and attached retrobulbar mass, as it appeared following exenteration of the affected orbit. Note that the mass appears to surround the optic nerve (arrows).
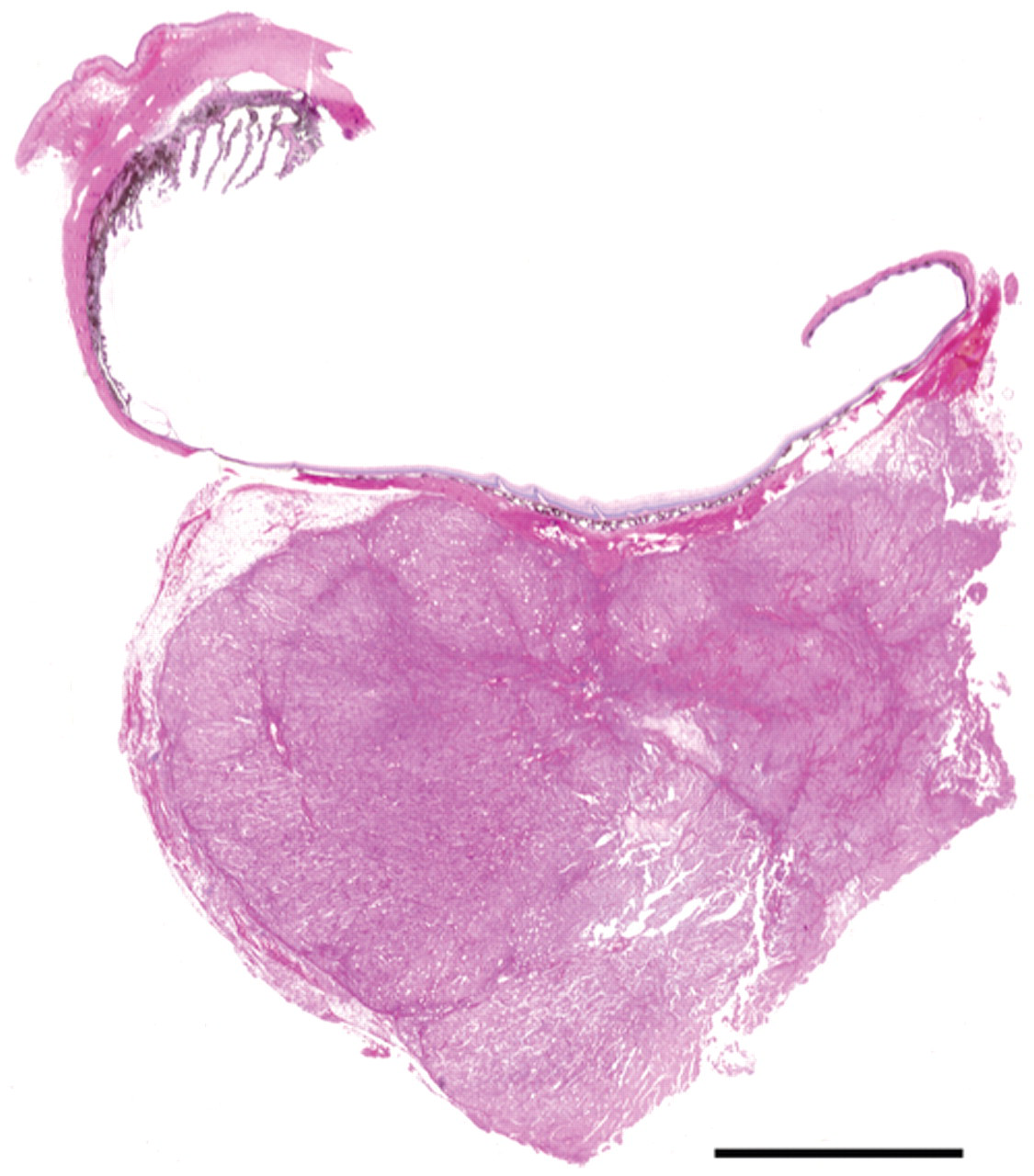
Sub-gross image of a longitudinal section of the right globe and associated retrobulbar mass. The mass is well demarcated, but unencapsulated, and has obliterated the optic nerve through invasion by and replacement with neoplastic cells. Additionally, neoplastic cells at the periphery of the mass can be seen invading the surrounding periorbital adipose tissue and skeletal muscle. Hematoxylin and eosin stain. Bar = 0.5 cm.
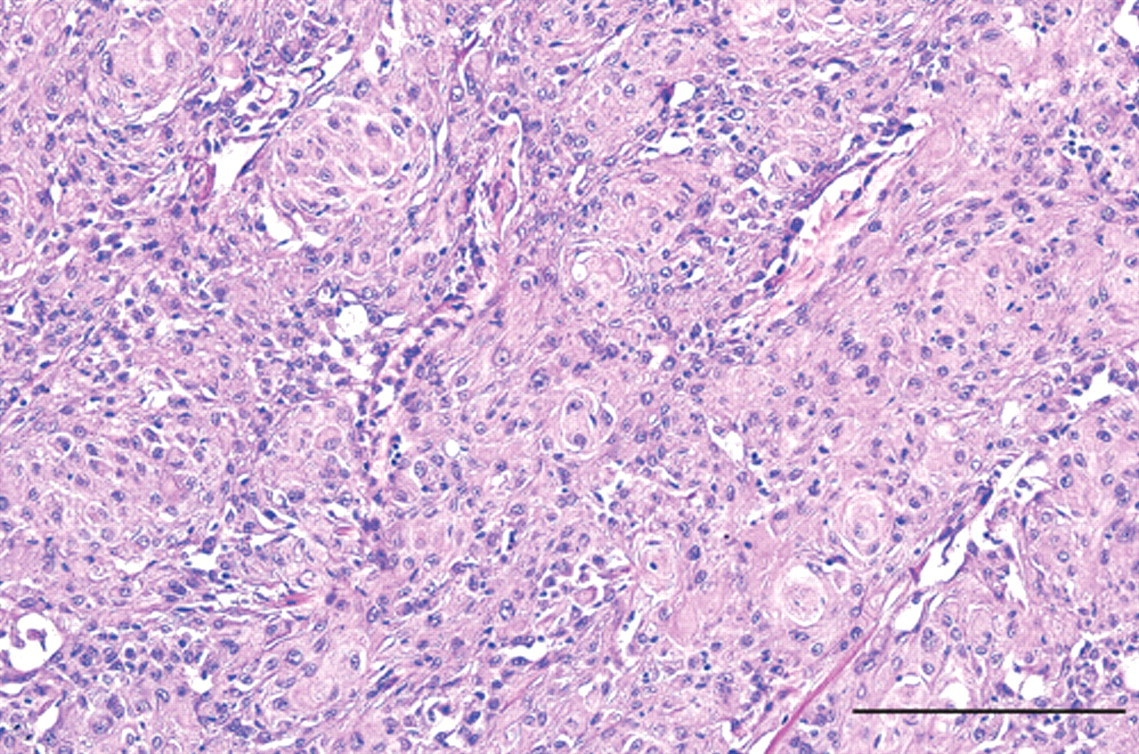
Photomicrograph of the soft, white retrobulbar mass in Figure 3. The majority of neoplastic cells are epithelioid in appearance, arranged in sheets and cords, and form concentric whorls, which are separated by thin bundles of more fibroblastic appearing cells. The microscopic appearance of the neoplasm was consistent with meningotheliomatous meningioma. Hematoxylin and eosin stain. Bar × 200 µm.
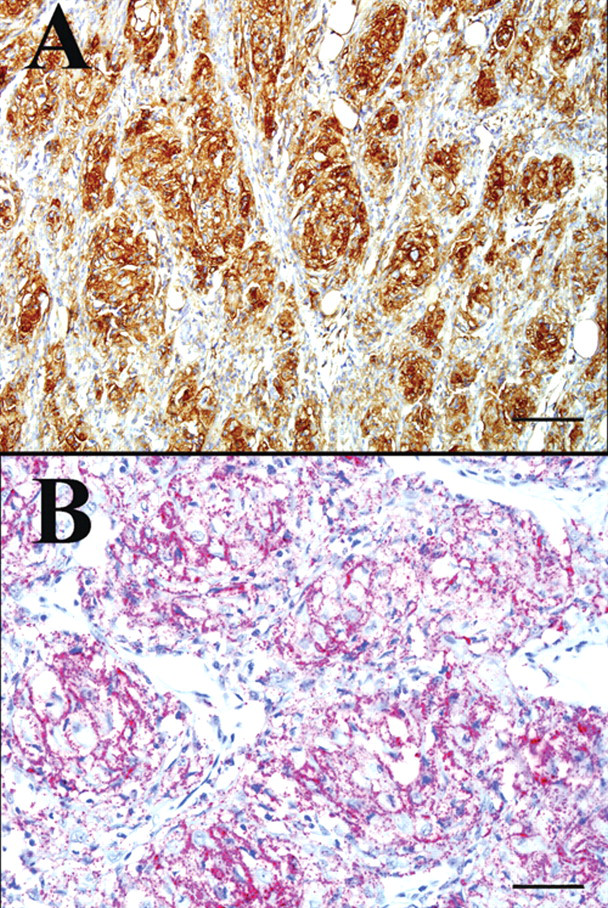
Histological features were consistent with meningotheliomatous meningioma, although carcinoma, nerve sheath tumor, and germ cell tumor were considered in the differential diagnosis. To confirm the diagnosis, the neoplasm was evaluated using immunohistochemistry for vimentin, b E-cadherin, c S100, d pancytokeratin, b and cytokeratins AE1 and AE3. b Immunohistochemical staining was performed with mouse monoclonal primary antibodies to vimentin (1:600), E-cadherin (1:1,000), pancytokeratin (1:100), and cytokeratins AE1/AE3 (1:200), as well as with a polyclonal rabbit anti-S100 antibody (1:3,000). The secondary antibodies were a biotinylated horse anti-mouse immunoglobulin G (IgG; vimentin, pancytokeratin, and cytokeratins AE1 and AE3) or goat anti-rabbit IgG (S100) e labeled with streptavidin–horseradish peroxidase conjugate and developed with diaminobenzidine chromogen. d For E-cadherin, the secondary antibody was a super sensitive multi-link biotinylated anti-IgG specific for mouse, rabbit, guinea pig, and rat. b Labeling was performed with super sensitive alkaline phosphatase conjugated to streptavidin. b The chromogen was Vulcan fast red. f Tumor cells stained positive for vimentin b (cytoplasmic) and E-cadherin c (membranous; Fig. 6), and negative for S100, d pancytokeratin, b and cytokeratins AE1 and AE3. b
Meningiomas are the most common mesodermal neoplasm of the canine central nervous system and occur more frequently in the brain than spinal cord. 21,32 Retrobulbar or primary orbital meningioma arises from the meninges of the optic nerve and is typically slow growing, invading circumferentially into the connective tissues of the orbit. 12,20,21 Grossly, retrobulbar meningiomas commonly appear as conical, solid tan to slightly granular masses, which are tightly adhered to the posterior aspect of the globe and taper along the nerve as it approaches the optic canal. 12,21 Retrobulbar meningioma is a rare neoplasm but has been reported previously in human beings, 19 dogs, 3,10,13,22,24,25,27 a cat, 1 and cattle. 30
Meningiomas in dogs are histologically diverse and display highly variable morphologic patterns. 21,32 Based on these histomorphologic differences, the World Health Organization (WHO) classifies domestic animal tumors of meningothelial cells into 9 different subsets, all with distinct characteristics; meningotheliomatous, fibroblastic, transitional, psammomatous, angiomatous, papillary, granular cell, myxoid, and anaplastic. 20 Additionally, microcystic (clear and vacuolated tumor cell cytoplasm) canine meningiomas, as classified according to the WHO human classification of meningiomas, have been reported. 25
Retrobulbar meningioma tends to have a predominately meningothelial or transitional pattern, but also exhibits distinctive morphologic features such as myxoid metaplasia, as was present in the current case, or cartilaginous and/or osseous metaplasia, which aids in their diagnosis. 12,24 Neoplastic cells tend to aggregate in cords, nests, and lobules and are large, pleomorphic, and epithelioid in appearance, with abundant eosinophilic cytoplasm. 12,25,32 This appearance and behavior can mimic that of an invasive epithelial tumor such as a squamous cell carcinoma or metastatic carcinoma, and in conjunction with the extensive variation in their histological pattern, retrobulbar meningiomas can be challenging to diagnose. 12,28 Although a specific immunohistochemical staining pattern using a variety of antigens does not exist, meningioma typically stains positive for vimentin and S100 and negative for glial fibrillary acidic protein and cytokeratin. Recently, positive E-cadherin has also been demonstrated. 4,25 In the present case, the diagnosis of meningioma is supported by positive vimentin and E-cadherin staining along with negative staining for cytokeratin, and helps corroborate the histomorphologic diagnosis. While not definitively diagnostic for meningioma, the positive staining for E-cadherin combined with negative staining for cytokeratin helps exclude carcinoma from consideration, as the latter would be expected to stain positive for both E-cadherin and cytokeratin. 28
Treatment for a retrobulbar meningioma includes exenteration to remove the affected globe and orbital contents, followed by radiation therapy. 4 Median survival time for dogs with a retrobulbar meningioma is undetermined; however, in one study, the median follow-up time of 1.7 years suggests a prolonged survival with surgery alone. 24 Survival times as long as 4.5 years postoperatively with surgery alone have been reported. 24 Local recurrence is common, 13,24 and intracranial extension along the optic nerve resulting in infiltration of the optic chiasm and diencephalon with subsequent development of blindness in the contralateral eye also can occur. 3,16,24 Additionally, extracranial metastasis has been reported 13,27 ; as such, the 2-cm pulmonary mass identified radiographically in the current case might represent metastasis from the retrobulbar meningioma. Following surgery, radiation therapy for retrobulbar meningiomas may be beneficial as radiation therapy prolongs postoperative survival for intracranial meningiomas. 2 Dogs with intracranial meningiomas treated with a combination of surgery and radiation have a median survival time of 16.5 months as compared to a median survival time of 7 months with surgery alone. 2 Ultimately, the optimal treatment protocol and prognosis for retrobulbar meningioma needs to be better defined. This is especially important for dogs with intracranial extension. However, the case reported herein provides valuable information regarding the potential for long-term survival following surgery alone for dogs with intracranial extension of retrobulbar meningioma.
Footnotes
a.
General Electric 3.0T Signa HDx, GE Healthcare, Milwaukee, WI.
b.
BioGenex Laboratories Inc., San Ramon, CA.
c.
BD Biosciences, San Jose, CA.
d.
Dako North America Inc., Carpinteria, CA.
e.
Vector Laboratories Inc., Burlingame, CA.
f.
Biocare Medical, Concord, CA.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.