
Abstract
Four adult mutant nackt mice, which demonstrate alopecia and CD4+ T-cell deficiency, and two outbred SENCAR mice (sentinels) were presented for routine health surveillance. Lesions were not observed at necropsy. Microscopically, all four nackt mice demonstrated multiple concretions that were 30–100 μm in diameter, irregularly rounded to oval, nonbirefringent, and amphophilic to basophilic. Many of the concretions appeared attached to or within the alveolar walls of all lung lobes. Approximately half of the concretions had irregular fracture lines. All concretions were periodic acid-Schiff positive, and Von Kassa staining revealed diffuse calcification. None of the concretions were associated with inflammatory cell infiltrates, and metaplastic ossification was not evident. A diagnosis of pulmonary alveolar microlithiasis, a rare disease in both humans and animals, was made based on the size and location of the concretions and the lack of an inflammatory response. This is the first report of a laboratory mouse demonstrating pulmonary alveolar microlithiasis.
Pulmonary alveolar microlithiasis is a rare condition in humans and animals with an unknown cause. The disease is characterized by the formation of calcium phosphate microliths (calcospherites) within the alveoli of the lungs without an associated inflammatory response. This disease was first described in humans by Harbitz11 in 1918 as extensive calcification of the lungs. In 1933, Puhr22 gave the disease the name alveolar microlithiasis. Since then, slightly more than 200 individual and small group case reports have been documented in the human literature.17,19,21,24,25 The veterinary medical literature has even fewer documented reports of alveolar microlithiasis found only in four dogs,5,8,15 a cat,6 a binturong,7 an orangutan,13 and a breeding colony of Afghan pikas.16 The pikas have the potential for being an animal model for alveolar microlithiasis because of its familial occurrence in this species. Our report documents a variant of pulmonary alveolar microlithiasis, presumably the early stages of the disease, in nackt mice.
We recently reported the nackt mouse mutation that affects skin and CD4+ T-cell development.3 Nackt is an autosomal recessive mutation with complete penetrance that was originally mapped to mouse chromosome 13, at a location 37 centiMorgans distal from the centromere. Affected animals show sparse, rough pelage from the first hair coat followed by regrowth and renewed hair loss during the subsequent hair cycle. The neck and back of adult mutant mice remain alopecic throughout life, and histologically the epidermis is hyperplastic with acanthosis and epidermal and follicular orthokeratosis. The most striking immunologic finding is a marked decrease in the proportion of CD4+ T cells in the thymus and peripheral lymphoid tissues. The nackt mutation represents a 118-base pair deletion of the cathepsin L gene, which is required for degradation of the invariant chain, a critical chaperone for major histocompatibility complex class II molecules.4
Four adult nackt mice (three female and one male) and two adult outbred SENCAR female mice, a strain unrelated to nackt that is sensitive to carcinogens, from the Department of Carcinogenesis at the University of Texas M. D. Anderson Cancer Center were presented for routine health surveillance. Mice were housed in specific pathogen–free rooms in a facility accredited by the American Association for The Accreditation of Laboratory Animal Care. Mice were kept in suspended polycarbonate cages (Lab Products, Maywood, NJ) with autoclaved hardwood bedding (PJ Murphy Forest Products Corp., Montville, NJ). Room environment was controlled at 20–22 C, 60–70% humidity, and 14 hours of light/10 hours of dark. Commercial pelleted rodent food (Harlan Teklad, Madison, WI) and autoclaved reverse osmosis water were available ad libitum. After euthanasia by carbon dioxide, complete necropsies were performed on all the animals, and standard tissues were collected and placed in 10% formalin. All tissues were then processed, paraffin-embedded, stained with hematoxylin and eosin (HE), and evaluated microscopically.
The lungs of all four mutant nackt mice were similarly affected. Within multiple alveolar lumina of each lung lobe, comprising no more than 5% of the total lung field, were amorphous to partially laminated (onion ringed) concretions that appeared to be attached to or within the alveolar wall (Figs. 1, 2). An occasional concretion was seen free within an alveolar or bronchiolar lumen. The concretions ranged in diameter from 30 to 100 μm and were irregularly rounded to oval, nonbirefringent, and amphophilic to basophilic. Approximately half of the concretions had irregular fracture lines. All concretions were periodic acid–Schiff positive, and Von Kassa staining revealed diffuse calcification. None of the concretions were associated with inflammatory cell infiltrates, and metaplastic ossification was not a feature in these animals. The alveolar walls, interstitium, and pulmonary vasculature appeared normal. These concretions were not observed in either of the SENCAR sentinel mice examined. A diagnosis of pulmonary alveolar microlithiasis was made based on the size and location of the concretions and the lack of an inflammatory response.
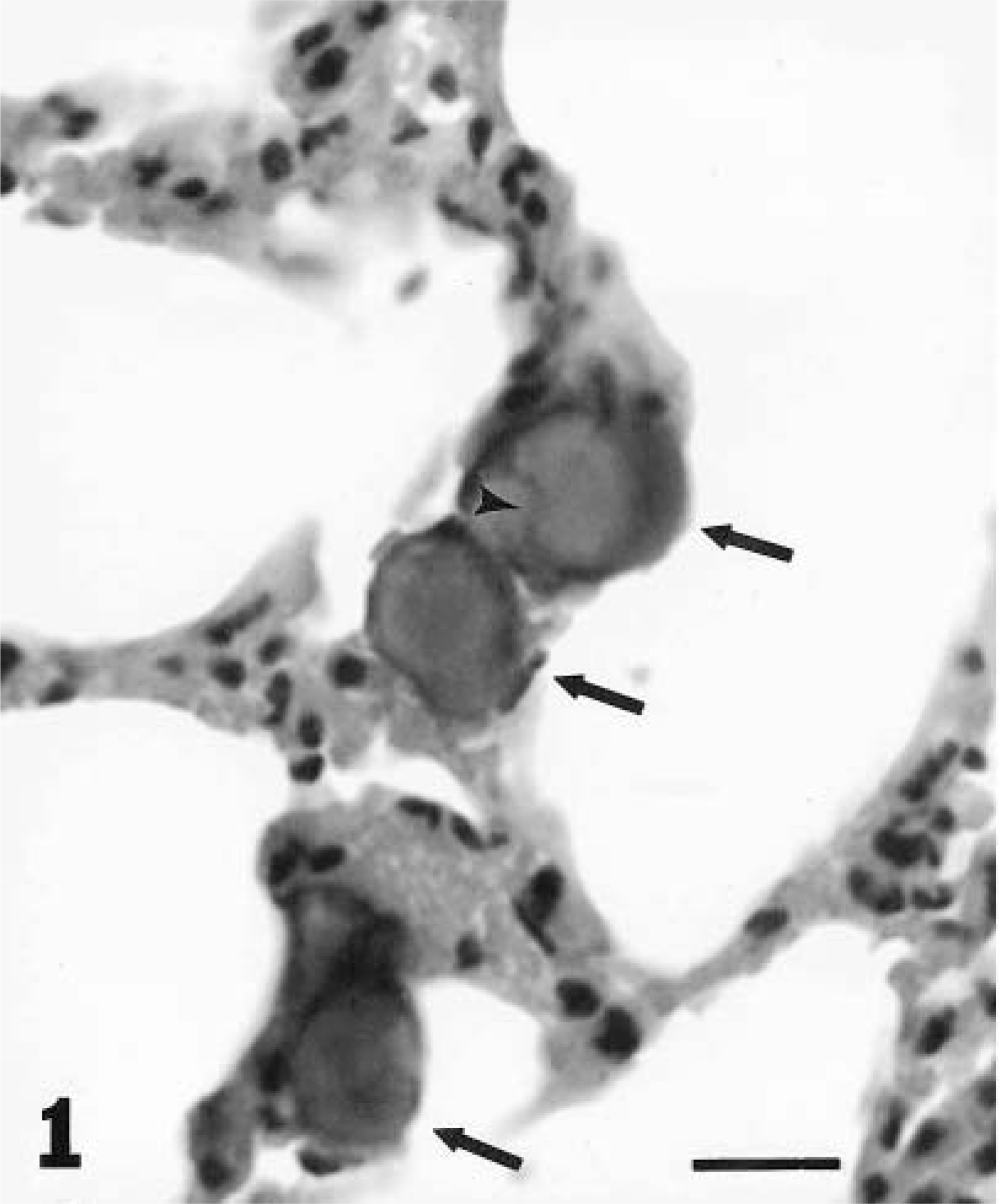
Lung; nackt mouse. Multiple microliths of various sizes are attached to or within alveolar walls (arrows). Note the irregular fracture line (arrowhead) and absence of inflammation. HE. Bar = 30 μm.
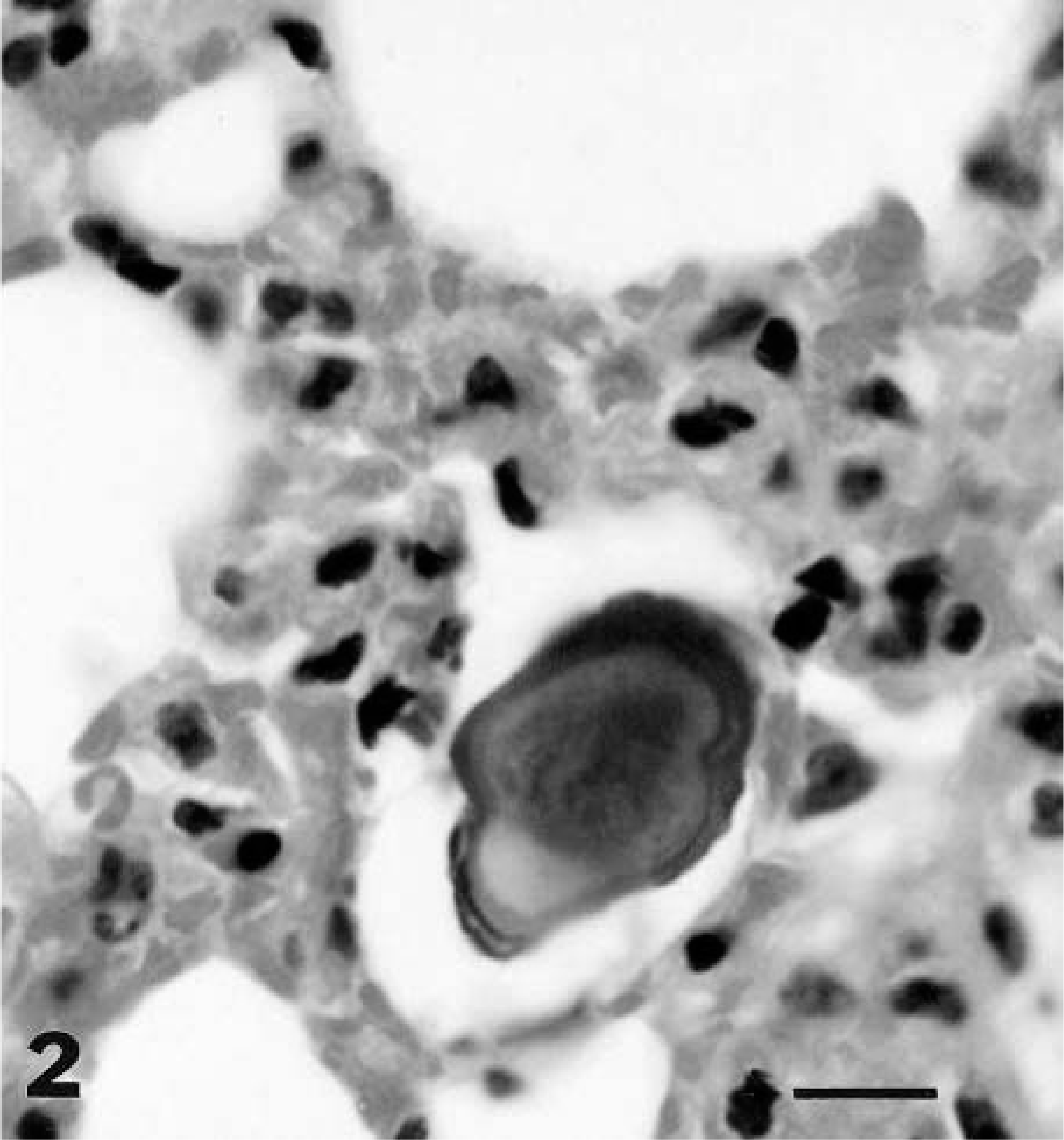
Lung; nackt mouse. Detailed view of a microlith. Note the laminations. HE. Bar = 15 μm.
In previous reports of microlithiasis in the human and veterinary literature, microliths were so numerous that the lungs were gritty on palpation, large numbers of alveolar lumina were filled, and in some cases decalcification of the lung was necessary to allow proper processing for microscopic evaluation.5,15,19,20,21 In some of these reports, the diameter of the microliths reached or exceeded 1 mm.15,25 In the mice we examined, the microliths were not discernible on palpation, filled only approximately 5% of alveolar lumina, and did not exceed 100 μm in diameter. However, the size and in some cases the number of the microliths were similar to those reported in Afghan pikas16 and dogs.8
The differential diagnosis of pulmonary alveolar microlithiasis includes pulmonary ossification, pulmonary corpora amylacea, and so-called blue bodies. In pulmonary ossification, the particles of bone are deposited haphazardly throughout the parenchyma, including the interstitium. Ossification was not observed in any of the nackt mice. Osseous metaplasia has been seen in dogs5,15 and Afghan pikas16 with pulmonary alveolar microlithiasis. The ossification was presumed to be the conversion of microliths into bone.5 Pulmonary corpora amylacea are laminated, rounded bodies found in emphysematous and normal lungs of elderly humans. Their eosinophilia in HE-stained sections and their failure to demonstrate calcification aid in the differentiation of corpora amylacea from microliths. In contrast, the microliths in the nackt mice were calcified, as demonstrated with von Kassa stain. Pulmonary blue bodies are intra-alveolar, laminated, basophilic concretions consisting of calcium carbonate in a mucopolysaccharide matrix.14 They usually occur in interstitial pneumonitides that resemble idiopathic desquamative interstitial pneumonia in human beings.14 In a cat reported to have microlithiasis in conjunction with bronchopneumonia, the concretions may have actually been blue bodies because they consisted of calcium carbonate.6 Pulmonary microliths are readily distinguished from blue bodies by their larger size (blue bodies are 15–40 μm and microliths are 250–750 μm) and their different chemical composition (calcium phosphate).19 Pulmonary alveolar microlithiasis also differs from blue bodies by the common absence of inflammation.19 Although many of the concretions observed in the nackt mice were similar in size to blue bodies, some were larger, and the absence of inflammation contributed to these concretions being diagnosed as a variant, or the early formative stage, of microlithiasis. A similar diagnosis was made in a human based on the size of the concretions (<100 μm in diameter) and the absence of laminations and inflammation.1 The microliths in these mice may have eventually enlarged by the addition of calcium phosphate to the external surface, enhancing the visibility of the laminations. Chemical analysis was not performed on the microliths in the nackt mice.
Pulmonary alveolar microlithiasis occurs with both a familial pattern and a sporadic pattern.17,19,25 It affects all ages, and there is no gender predilection.17,19 Possible etiologies include an inherited metabolic abnormality in the lung,19 abnormalities in calcium and phosphorus metabolism,2 abnormalities in the immune system,18 environmental factors,19,21 and anatomic and physiologic abnormalities of the lung.19,25 Although nackt mice are maintained in congenic strains, evaluation of archived tissue and more recent animals presented for routine health surveillance (>20 mice) has failed to demonstrate microlithiasis. Therefore, this disease entity in this group of nackt mice is sporadic and may have been related to an unknown environmental factor, possibly in association with immunosuppression or the lack of functional cathepsin L, a ubiquitous scavenger enzyme believed to be involved in intracellular protein degradation,4 in these mice.
Alveolar microlithiasis has been seen in association with other human medical conditions such as milk alkali syndrome,20 diaphyseal aclasia,23 pectus excavatum,12 and hypertrophic pulmonary osteoarthropathy.10 There have been additional cases of microlithiasis affecting extrapulmonary sites such as the sympathetic ganglia,9 gonads,9 and seminal vesicles2 in association with pulmonary alveolar microlithiasis. Microliths were not observed in any other tissues examined in the nackt mice.
Currently, no known medical treatment for pulmonary alveolar microlithiasis is available, and the disease can progress to the extent of compromising lung capacity and contributing to heart failure.19 Total lung transplantation is the only known cure for advanced disease.17 Although alveolar microlithiasis is sporadic in mice with the nackt mutation, these mice may be a useful model contributing to a better understanding, treatment, and cure of pulmonary alveolar microlithiasis.