
Abstract
A 2-year-old female Boxer dog was presented with a history of skin lesions that started 1 month after being given oral glucocorticoids for a neurologic problem. Clinically, the animal had focal areas of alopecia with papules and nodules often with ulceration overlain by crusts. Lesions were most common on the dorsum and the lateral aspects of the trunk and extremities. Histologic evaluation revealed pigmented fungal organisms within the lumina of hair follicles and throughout the dermis and subcutis. These organisms were associated with a multinodular, pyogranulomatous luminal folliculitis/furunculosis, dermatitis, and panniculitis. Curvularia sp. was isolated from the cutaneous lesions. The histologic identification of dematiaceous fungal organisms in the hair follicles may explain how phaeohyphomycosis can occur without history of a penetrating injury.
Phaeohyphomycosis is a general term for an infection by any of a number of pigmented fungi. Most of the organisms associated with phaeohyphomycosis are considered opportunistic. The fungi known to cause phaeohyphomycosis are ubiquitous and have been recovered from vegetative matter and soil all over the world. Traumatic implantation of the etiologic agent and wound contamination by the organism are thought to be the primary modes of infection. Clinical disease is uncommon and almost invariably occurs in immunocompromised or debilitated hosts.
In this report, we describe the clinical and histologic features of phaeohyphomycosis due to Curvularia spp. in a dog with a history of long-term corticosteroid administration. A distinctive feature of this case was that organisms were commonly identified in the lumina of hair follicles, suggesting that the follicular os was the portal of entry for colonization of the dermis and subcutaneous fat.
A 2-year-old female Boxer dog was presented with a history of skin lesions that started 1 month after she was given oral glucocorticoids (prednisone, 1 mg/kg every 12 hours) for a neurologic problem. Clinically, the animal had focal areas of alopecia that contained papules and nodules, often with ulceration overlain by crusts. Lesions were most common on the dorsum and the lateral aspects of the trunk and extremities. The lesions were nonpainful and nonpruritic.
The clinical differential diagnosis included bacterial pyoderma, demodicosis, and superficial and deep fungal dermatitis. Six 6-mm punch biopsies of haired skin were obtained from representative lesions and submitted for histologic and microbiologic evaluation.
Samples for histologic evaluation were fixed in 10% neutral buffered formalin, embedded in paraffin, processed routinely, and stained with hematoxylin and eosin (HE), periodic acid–Schiff (PAS), Gomori–methenamine silver (GMS), and Fontana–Masson techniques. Examination revealed numerous, variably pigmented, septate fungal organisms in the lumina and walls of follicular infundibula and within nodular pyogranulomas in the dermis and subcutaneous fat. The pyogranulomas were of various sizes and were composed of epithelioid cells, multinucleated giant cells, neutrophils, and lymphocytes (Fig. 1). Although generally translucent, some of the fungal organisms had brownish pigment in the cell walls of the hyphae. The natural pigmentation varied from dark brown to light yellow. The hyphae were septate and branched and varied in diameter (8–10 µm to ≥20 µm in dilated vesiculated forms). Hyphae with larger diameters and thicker walls had regional constrictions associated with terminal globose dilations, giving the appearance of chlamydospores. The organisms were usually scattered throughout the inflammatory reaction; however, in some areas they were clustered, forming small aggregates.
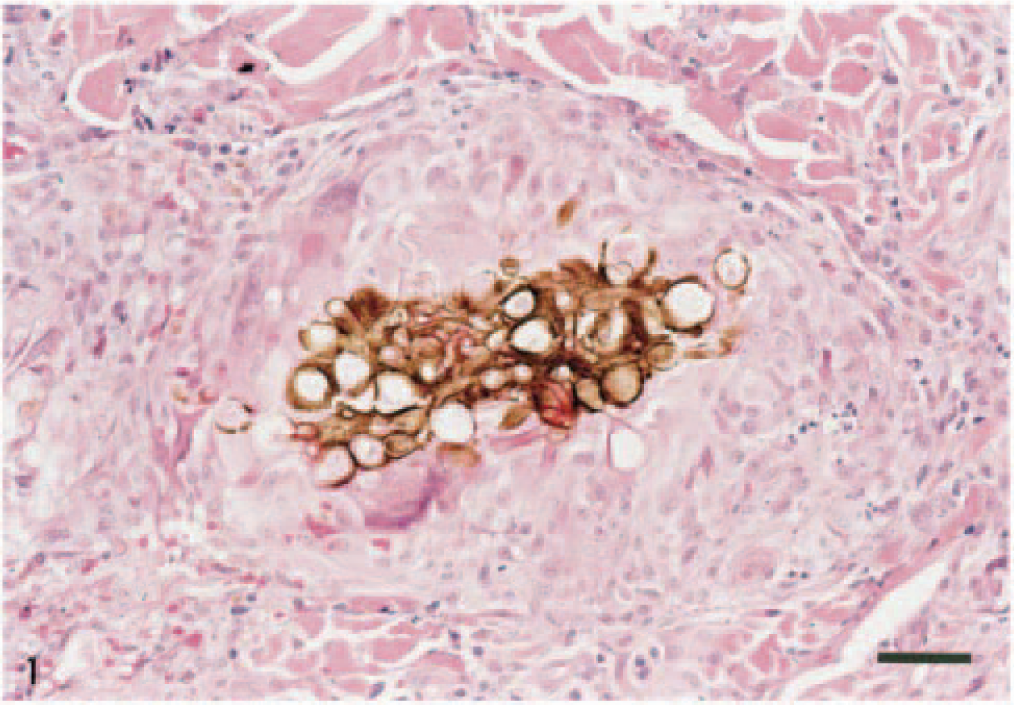
Skin; dog. Granulomatous lesion in the deep dermis. Central aggregate of brown, pleomorphic hyphae surrounded by epithelioid-like macrophages, multinucleated giant cells, and lymphocytes. HE. Bar = 70 µm.
Hyphae with a similar morphology but less pigmentation were present within the cornified material of the follicular infundibula (Fig. 2). Occasionally organisms were present in the walls of the outer sheaths (Fig. 3). Infected follicles were surrounded by mixtures of lymphocytes, macrophages, and neutrophils that sometimes extended into the follicular lumina (Fig. 3). This mixture occasionally evolved into a furunculosis with apparent extrusion of dematiaceous fungi into the dermis. The larger pyogranulomas had central necrosis and were accompanied by areas of epidermal ulceration.
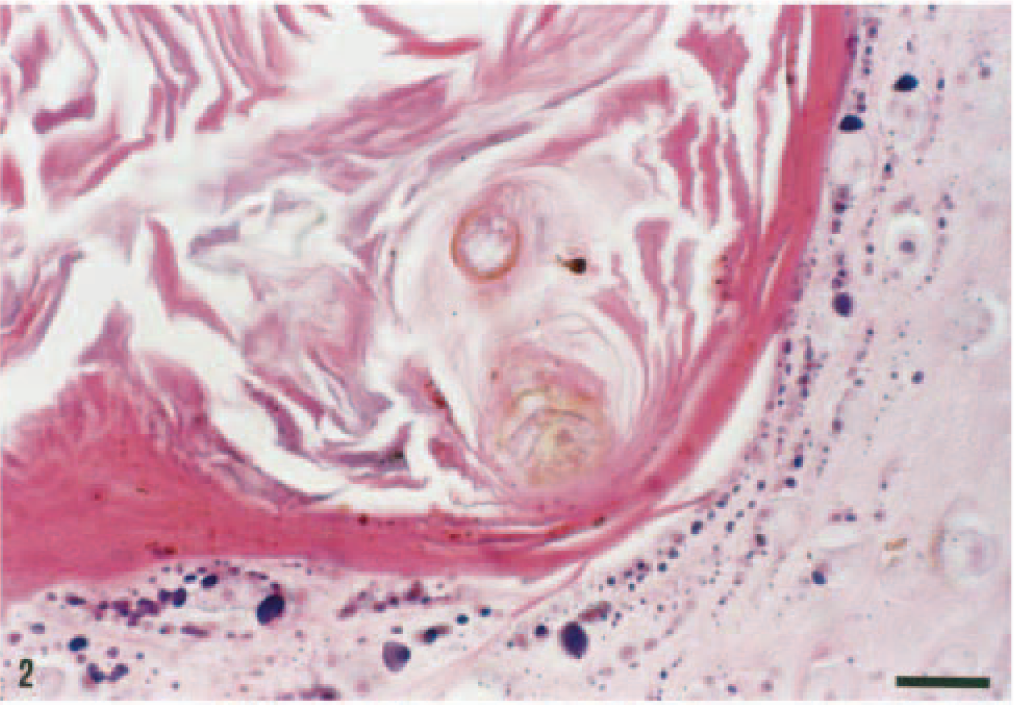
Skin; dog. Dematiaceous fungus within the keratin of follicular infundibulum. HE. Bar = 20 µm.
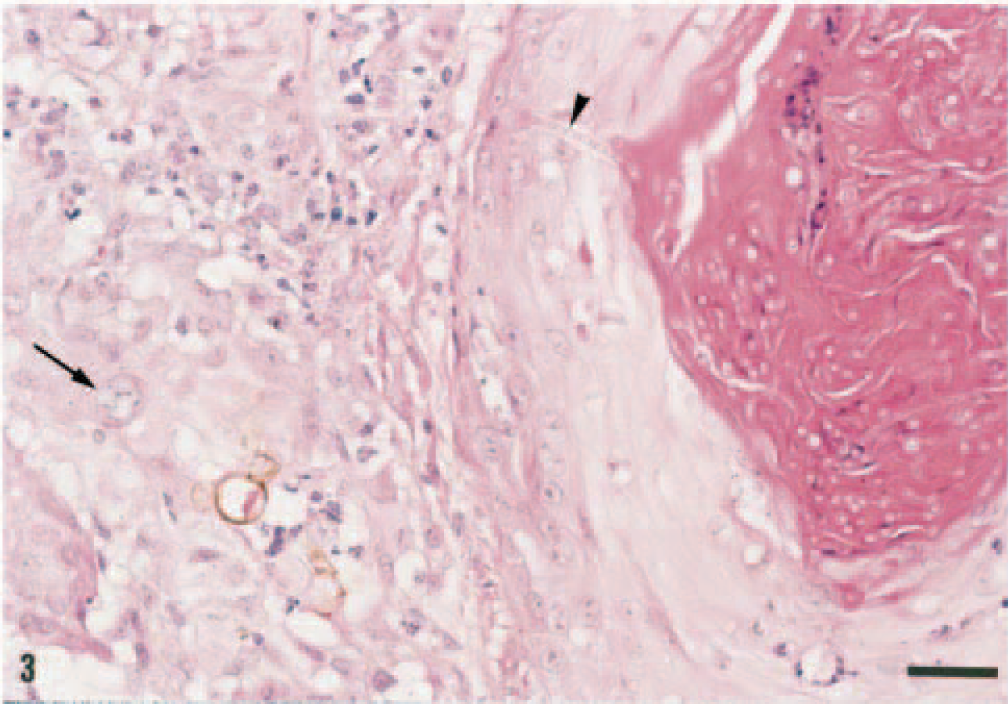
Skin; dog. Pyogranulomatous perifolliculitis. Numerous fungi are present in the follicular infundibulum. A septate hypha is present in the wall of the outer sheath (arrowhead). Notice the brown fungus near the hair follicle, with a dilatation similar to a chlamydospore. The organisms varied from dark brown to devoid of pigment (arrow). HE. Bar = 40 µm.
The fungal organisms were best demonstrated with PAS and GMS histochemical stains. In sections stained by the Fontana–Masson method, the cell walls of fungi present in both the dermis and the hair follicle lumina were dark gray to black (Fig. 4).
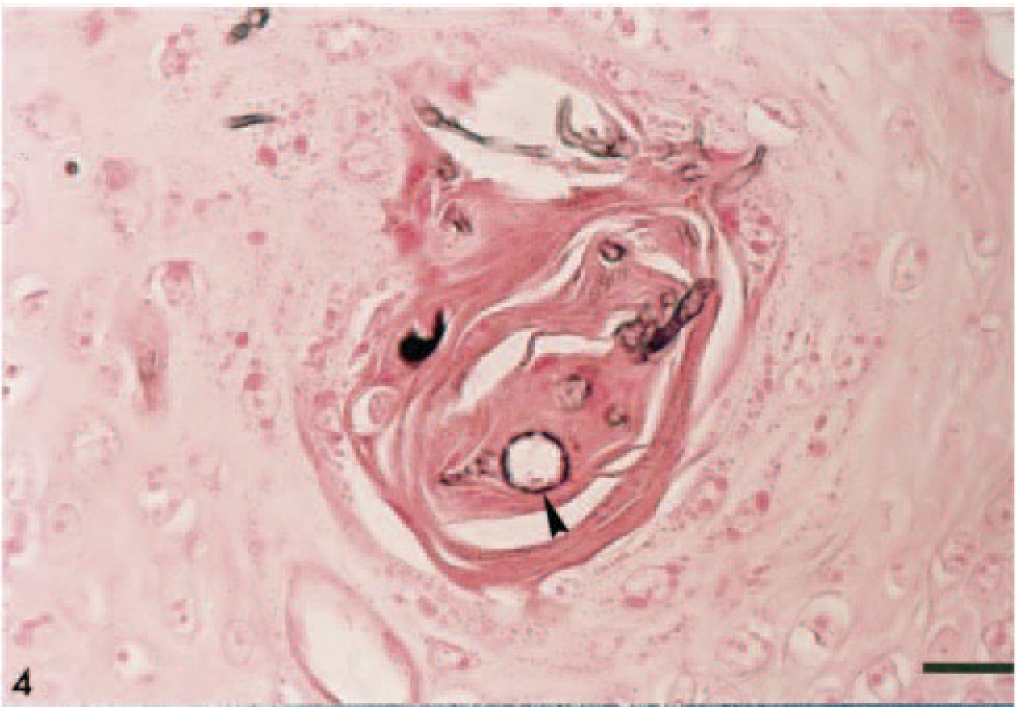
Skin; dog. Intrafollicular fungi stained black. Staining is limited to the cell walls of hyphae. The etiologic agent is pleomorphic, with dilated structures similar to chlamydospores (arrowhead). Fontana–Masson. Bar = 30 µm.
Skin samples were submitted for bacterial and fungal cultures. On Sabouraud's peptone-glucose agar, pure cultures of pigmented fungus grew. Curvularia was identified in culture because it grew quickly at 25 C, it had lanose, melanizing colonies, and it produced dark, triseptate poroconidia. Based on the clinical features, the demonstration of pigmented fungi in histologic sections, and isolation of Curvularia sp. on Sabouraud's glucose agar, a diagnosis of cutaneous and subcutaneous phaeohyphomycosis was made.
Phaeohyphomycosis is the name given to cutaneous and systemic diseases caused by black molds that develop dark-walled, septate mycelia in tissue. The diagnosis of phaeohyphomycosis requires demonstration of pigmented fungi in wet mounts or in histologic sections. 5 With HE, the pigmentation of the fungi varies from dark brown to light yellow. Hyphae may appear devoid of pigmentation. Dematiaceous fungi are pigmented by melanin, 6 and the quantity of melanin produced depends upon the availability of nutrients, growth rate, age of the organisms, and viability. 10 Fontana–Masson staining highlights melanin pigment by reducing silver and results in a dark gray-black pigment in both mammal and plant species. 22 In several culture-proven cases of dematiaceous fungal infections, the organisms did not appear pigmented on HE-stained sections but stained with the Fontana–Masson procedure. 9 For this reason, Fontana–Masson staining has been used to differentiate dematiaceous fungi from other fungi 20 and to enhance the staining of melanin in lightly pigmented organisms. 16,20,24 Although Fontana–Masson staining is useful for identifying pigmented fungi, 20 it may not be specific for these fungi; many nondematiaceous fungi can also be stained with this technique. 10
Curvularia is a pigmented fungus that has been associated with phaeohyphomycosis 3 and eumycotic mycetomas. 8 Organisms are scattered throughout the inflammatory reaction and producing a characteristic C-shaped scroll in histologic sections. 1,8,9,24,25 Both features were observed in this case. Still, the histologic appearances of phaeohyphomycotic agents are similar enough that they cannot be unequivocally differentiated solely on the basis of morphology, and culture is always needed for specific identification of the etiologic agents. 5,14
The fungi known to cause phaeohyphomycosis are ubiquitous and are usually recovered from vegetative matter and soil. 7 Most infections arise from traumatic implantation or wound contamination by the organism. For human infections phaeohyphomycosis has been divided into four forms based on the location of the infection and the route of inoculation: superficial, cutaneous, subcutaneous, and systemic. 12 Superficial infections are limited to the epidermis and hair follicles, with no involvement of dermal connective tissues and minimal inflammation. Cutaneous phaeohyphomycosis involves keratinized and dermal tissues, and inflammation is characteristically observed. Both superficial and cutaneous forms do not affect the subcutaneous fat and are believed to result from colonization of the epidermis and hair follicles. Subcutaneous phaeohyphomycosis is the most common form and is characterized by the presence of granulomas in the adipose panniculus. It follows the traumatic implantation of the etiologic agents or, as appeared to occur in this case, a progression from superficial to cutaneous to subcutaneous infection. 12 The systemic form involves internal organs other than soft tissues adjacent to the skin. The most common types of phaeohyphomycosis in veterinary medicine are the subcutaneous and systemic forms. 18,24 In most of the cases reported in domestic animals, there is no involvement of the epidermis or upper dermis, and traumatic implantation or wound contamination is thought to be the primary mode of infection. 3,13,16 In the dog described here, the lesions were a combination of the cutaneous and subcutaneous forms.
Histologically, the most striking and unexpected feature of this case was the presence of numerous fungal organisms in the follicular infundibula associated with a pyogranulomatous folliculitis/furunculosis. Several explanations are possible for this observation. The first is that this dog suffered from a dual infection of Curvularia in the dermis/subcutis and of dermatophytes in the hair follicles. We considered this unlikely because dermatophytes were not identified by culture and the infundibular hyphae had the same morphology as those present in the dermis, with terminal structures that resembled chlamydospores. 5 In addition, the organisms in the hair follicles occasionally had a light brown pigment that was strongly accentuated with Fontana–Masson stain. These features are not present in dermatophytes.
The second possibility is that the organisms were being eliminated through the follicular epithelium. Transepidermal elimination is a common means by which foreign material is removed from the dermis. 2,11 Although this process has been associated with other cutaneous mycoses, 15,21 we do not believe it occurred in this case based on the large number of organisms present in the infundibula and because elimination of a foreign body from the dermis is invariably associated with the concurrent extrusion of dermal debris such as collagen. Dermal debris was not found in the infundibula in which organisms were identified.
The third possibility is that the infection originated in the cornified tissues and from there invaded the subjacent dermis and subcutaneous fat. Invasive fungal dermatitis in which the skin served as a portal of entry for Curvularia has been described in extremely low-birth-weight human neonates 17 and, less often, in adults. 1 In these cases, skin biopsies revealed a progression of infection starting with colonization of the stratum corneum, then extension into the infundibula of the hair follicles, and finally invasion through the walls of the outer sheaths and into the dermis/subcutis, where organisms incited a pyogranulomatous inflammatory response. 4,14
The presence of intrafollicular pigmented hyphae was previously described in a dog with subcutaneous phaeohyphomycosis, although in that dog, the hair follicles were devoid of inflammatory cells and there was a history of traumatic injury. 3 In the dog of the present report, the presence of abundant intrafollicular organisms associated with an inflammatory response and the absence of a history or clinical evidence of traumatic injury suggest an initial superficial infection followed by invasion of adjacent tissues.
Curvularia and other etiologic agents associated with phaeohyphomycosis are considered opportunists, and infection of healthy humans and animals is uncommon. Although phaeohyphomycosis in humans is associated with immunosuppression or a concurrent debilitating disease, immunosuppression is not a common finding in cats with phaeohyphomycosis. 16 Although host susceptibility to Curvularia infection is poorly understood, an experimental study in mice suggested that cellular immunity plays an important role in prevention of severe disease. 23 The dog in this report may have been immunocompromised because of the corticosteroids that were administered for a month prior to development of cutaneous lesions.
This case represents an example of invasive phaeohyphomycosis. The histologic finding of fungal organisms within the follicular infundibula and extending across the outer sheath indicates a nontraumatic mechanism for implantation of the fungi into deeper tissues of immunosuppressed dogs.