
Abstract
Fonsecaea pedrosoi is the most common fungal agent associated with human chromoblastomycosis. In the current study, a phaeohyphomycotic condition of the skin caused by Fonsecaea pedrosoi is described in a dog.
Keywords
Introduction
Chromoblastomycosis, phaeohyphomycosis, and eumycotic mycetoma are a group of systemic and cutaneous diseases caused by dematiaceous fungi. 1 Dematiaceous fungi are characterized by a brown to black pigmentation of their hyphae and are ubiquitous in nature. Most common species encountered in disease conditions include Fonsecaea spp., Alternaria spp., Bipolaris spp., Cladophialophora spp., and Curvularia spp. 3 This report describes a phaeohyphomycotic condition caused by Fonsecaea pedrosoi infection in a dog.
Fresh and formalin-fixed skin samples from a Jack Russell Terrier were submitted for biopsy and culture. The dog had a 3-year history of chronic erythema, alopecia, and pustulation of the axillary regions and ventral abdomen (Fig. 1A). Clinical history described periodic treatment with cephalexin, ketoconazole, and chloramphenicol, resulting in temporary remission. In the clinical history, it was mentioned that the dog was recently treated with steroids for 30 days.
Formalin-fixed tissues were routinely processed, embedded in paraffin, 5-μm sections cut, placed on glass slides, and stained with hematoxylin and eosin (HE) for light microscopic examination. Additionally, a special histological stain (Grocott-Gomori methenamine silver stain) was applied following the standard operating protocols at the histopathology section of the Veterinary Diagnostic and Investigational Laboratory (VDIL). A routine aerobic culture and fungal culture were performed on fresh skin samples following standard operating protocols of VDIL's bacteriology section.
The skin biopsy specimen extended only to the mid-dermis to deep dermis, with no subcutis included. There was mild to often-marked orthokeratotic keratosis with rare crusting. The ostia and follicles were markedly dilated (up to 1 mm in diameter) and plugged with keratin. There was mild to moderate irregular thickening of the epidermis, with mild undulation and preservation of the basal layer. The follicular epithelium was thin (1 to 2 cell layers). No normal hair follicles were included in the section. The blood vessels in the superficial dermis were increased, and there was occasional marked dilation of vessels. There was edema and hemorrhage throughout the dermis that appeared to be more prevalent within the superficial dermis. There was moderate to heavy infiltration of lymphocytes, plasma cells, and macrophages; however, fewer infiltrates of eosinophils and neutrophils were observed. These infiltrates were especially prominent in the superficial dermis but extended as aggregates into the mid-dermis and minimally extended along follicles, with rare infiltration of the follicular epithelium. Lightly pigmented hyphae were seen with difficulty on HE staining. A Grocott-Gomori methenamine silver stain revealed random hyphae throughout the dermis. The hyphae were approximately 5 μm in diameter, segmented but nonparallel walled, and rarely branching (Fig. 1B). Some hyphae presented as short budding chains.
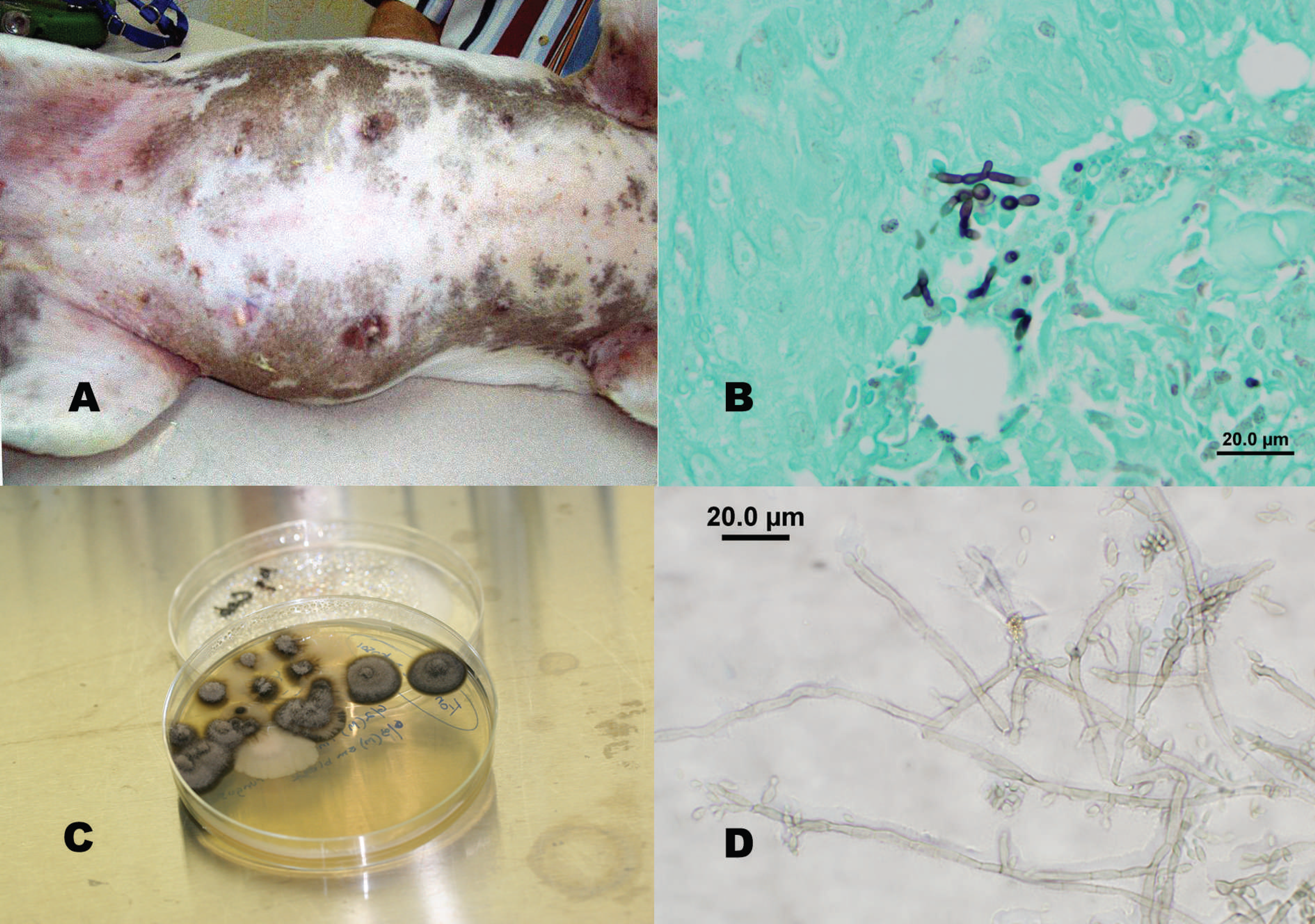
Routine aerobic culture and a fungal culture were performed on the tissue. Aerobic culture resulted in the growth of few colonies of Staphylococcus epidermidis, Actinomyces spp., and Pseudomonas stutzeri. Fungal culture resulted in a pure growth of moderate numbers of small black fungal colonies after 7 days of incubation at ambient temperature. The fungal colonies were greenish black with a velvety heaped and folded surface (Fig. 1C), and were covered with silvery mycelium. Upon further incubation, colonies developed a cone-shaped convex protrusion at the center. Microscopic examination was performed using a transparent adhesive tape preparation and lactophenol cotton blue stain. The isolate had septate brown branching hyphae with Fonsecaea-type conidiation (Fig. 1D). From the colony morphology and microscopic characteristics, this fungal isolate was identified as Fonsecaea pedrosoi.
Fonsecaea infections are more common in tropical and subtropical regions, and can cause a variety of pathological changes ranging from simple sinusitis, keratitis, and subcutaneous infection to severe and life-threatening disseminated conditions in human. 2 Two species of Fonsecaea are reported in human chromoblastomycosis, F. pedrosoi and F. compacta. 2 Fonsecaea pedrosoi is a predominant etiology in human chromoblastomycosis, 2 whereas F. compacta is rare.
The first reported nonhuman case of phaeohyphomycosis caused by F. pedrosoi was reported in a cat. 4,5 This feline case presented as a nonpruritic swelling on the nasal planum, unlike the spreading pattern of cutaneous infection observed in the present case. To the authors' knowledge, there have been no reports of infection in dogs with this species of fungus.
There are more than 60 genera of fungi causing phaeohyphomycosis. Some of the most common genera include Alternaria, Bipolaris, Cladophialophora, and Curvularia, all of which are widespread in the environment. 1 Fewer species of dematiaceous fungi are known to cause chromoblastomycosis. The most common fungal species (more than 90% of the cases) reported in human beings is F. pedrosoi. 1 This fungal species also has been reported as an occasional cause of cerebral and subcutaneous phaeohyphomycosis. 1
Infections caused by dematiaceous fungi in humans require both surgical and medical treatment. Itraconazole is found to be effective in most cases of chromoblastomycosis. In the present canine case, the veterinary practitioner reported 2 treatment cycles with itraconazole, resulting in clinical remission but subsequent relapses. Complete surgical recession of small lesions and antifungal treatment is the recommended treatment in human chromoblastomycosis 6,7 ; however, a complete cure is not achievable, and relapses are common. Further, in the present case, steroid treatment was administered for 1 month prior to biopsy submission and may have caused an iatrogenic immunosuppression with subsequent exacerbation of the condition. Based on the clinical and laboratory findings, a diagnosis of superficial phaeohyphomycosis was rendered. Considering the high incidence of chromoblastomycosis caused by F. pedrosoi in humans, the zoonotic potential of this pathogen should not be ignored.
Acknowledgements. The authors would like to thank Dr. Tom Holms, Holms Animal Clinic, Waycross GA, for providing necessary clinical information on the patient and the University of Georgia–Tifton Veterinary Diagnostic and Investigational Laboratory for assistance in tissue processing.