
Abstract
A 4-year-old male Pekingese dog was referred to the clinic with a history of recurrent seizures and progressive abnormal gait and behavior, which did not respond to treatment. At necropsy, a large cortical defect in the right temporo-parietal cortex, malacia of subcortical white matter, right basal nuclei, and capsula interna, as well as abnormalities of the right hippocampus were observed. Histological examination of the brain revealed moderate to severe nonsuppurative meningoencephalitis in the left cerebral hemisphere and extensive infarction-like lesions with milder inflammation in the right hemisphere. In the right hippocampus, the pyramidal cells were arranged in a gyrus-like pattern and intermingled with gemistocytic and fibrillary astrocytes. The histopathological features of the inflammatory lesions were consistent with necrotizing meningoencephalitis and resembled those described in so-called Pug dog encephalitis. The hippocampal changes were interpreted as dysplasia (monolateral hippocampal cortical hamartia), unrelated to clinical signs and necrotizing inflammatory lesions.
The association of noncorrelated dysontogenetic and inflammatory lesions of the central nervous system is an exceptional finding. We describe a necrotizing meningoencephalitis and infarction-like lesions in a Pekingese dog associated with a cortical hamartia of the right hippocampus.
A 4-year-old intact male dog was referred to the clinic for small animals at the Faculty of Veterinary Medicine, Pisa University, Italy, with a history of seizures and abnormal gait. Vaccinations, including annual boosters, against distemper virus, parvovirus, leptospirosis, and canine adenoviruses had been given at appropriate time intervals. No major medical problems, with the exception of neurological signs for the last 6 months, had ever occurred. On neurological examination, the most conspicuous findings were a head tilt to the left and a tendency to circle to the left. Proprioceptive positioning responses were delayed in the left limbs and normal in the right. Menace responses were absent on the left and normal on the right. Pupillary light reflexes, as well as spinal cord reflexes, were normal bilaterally. Seizures, described as generalized motor seizures, occurred approximately twice per month, but in the last 2 weeks, the dog had suffered at least two prolonged seizures per week. The anatomic diagnosis was a lesion in the right forebrain.
Results of a complete blood count, serum biochemical analyses, and urinalysis were within reference ranges. Cerebrospinal fluid evaluation revealed 110 cells/µl and a positive Pandy test. The predominant cell type was the small lymphocyte. The owner declined further diagnostic tests, and the dog was treated with phenobarbital, dexamethasone, and amoxicillin. The dog was discharged, but a week later returned for clinical examination because of severe convulsions and abnormal behavior. The dog was depressed, his appetite was diminished, and he had urinated and defecated in the house several times. Ataxia, as well as postural deficits in the left limbs and the right hind limb were observed. Despite therapy, seizure activity increased, and the dog's neurological status worsened. The prognosis was poor and the owner requested euthanasia.
On postmortem examination, the brain showed a cortical defect of approximately 12 by 8 mm in the right parieto-temporal cortex. The brain was fixed in phosphate-buffered 10% formalin solution and then transversally cut. Gross examination of the cross sections disclosed the presence of extensive, multifocal, cortical and subcortical malacic areas in the right cerebral hemisphere. The affected areas were discolored brown, and tissue cavitations were present in the malacic areas. The lesions involved temporo-parietal cortex, lobus piriformis, subcortical white matter, capsula interna, and basal nuclei. Mild swelling of the left cerebral hemisphere with mild displacement of the fornix and thalamic midline structures was also observed. The right hippocampus was enlarged, and a convoluted appearance was evident (Fig. 1).
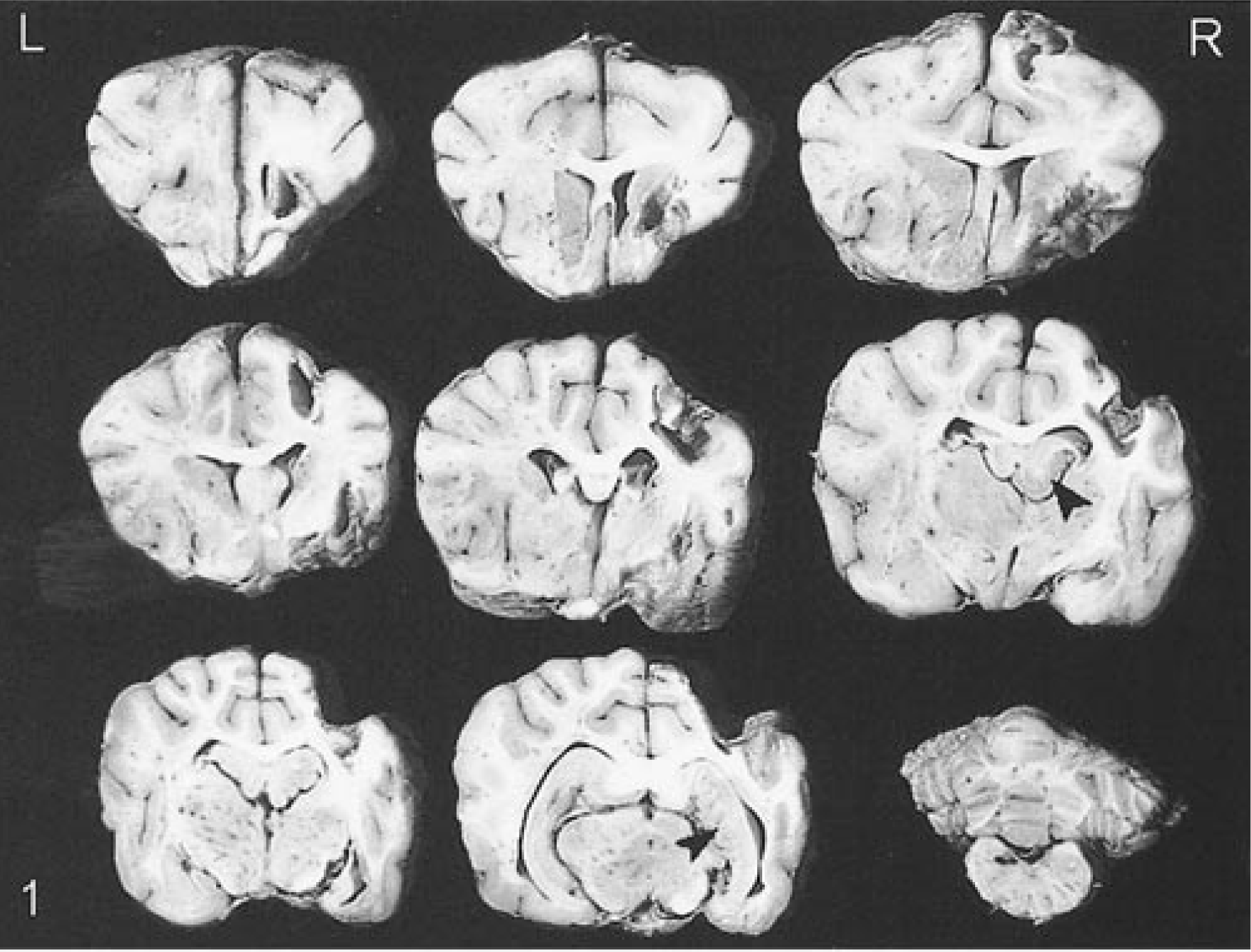
Transverse sections of fixed brain; dog. There are extensive multifocal necrotic lesions in the right hemisphere involving capsula interna, basal nuclei, parietal and temporal cortex, lobus piriformis, and subcortical white matter. A mild right displacement of midline structures is also present. The right hippocampus is enlarged and arranged in a gyrus-like pattern (arrowheads).
The brain, spinal cord and major organs were sampled and routinely processed for histology. Tissue sections were stained with hematoxylin and eosin, Luxol fast blue, periodic acid–Schiff, crystal violet for Nissl substance, Bielschowsky, Gram, and Grocott methods. Selected brain sections were also stained with the immunoperoxidase method for glial fibrillary acidic protein, as well as for canine distemper virus, Toxoplasma gondii, and Neospora caninum.
Histologic changes were restricted to the brain. Microscopic examination of the malacic lesions of the right hemisphere revealed neuropil disruption with presence of glial fibrils and mesenchymal connective tissue, congested capillaries, lymphocytes, many Gitter cells, and macrophages containing hemosiderin. Inflammation was minimal with small lymphocytic cuffs and a few gemistocytes in the white matter adjacent to the necrotic cavities. Subcortical cavities showed tissue rarefaction with moderate inflammation and many Gitter cells.
Histologic examination of the left cerebral hemisphere disclosed severe multifocal nonsuppurative meningoencephalitis involving both gray and white matter. Subcortical white matter was most severely involved and lesions were characterized by perivascular accumulation of lymphocytes, many plasma cells, and macrophages. The inflammatory cells infiltrated the white matter, which showed edema, gliosis, myelin vacuolization, and occasional axonal swelling. Marked proliferation of rod cells and hypertrophy and hyperplasia of vascular endothelium were additional findings. Moderate inflammatory changes were also observed in the septum pellucidum and capsula interna. In the most severely affected areas, inflammation extended to the gray matter with presence of multifocal microglial foci, necrosis of single neurons of the deeper strata, and occasional neuronophagia. In these areas and in the sulci, leptomeningitis was more pronounced, showing accumulation of lymphocytes, plasma cells, and macrophages with extension to the subpial perivascular space (Fig. 2).
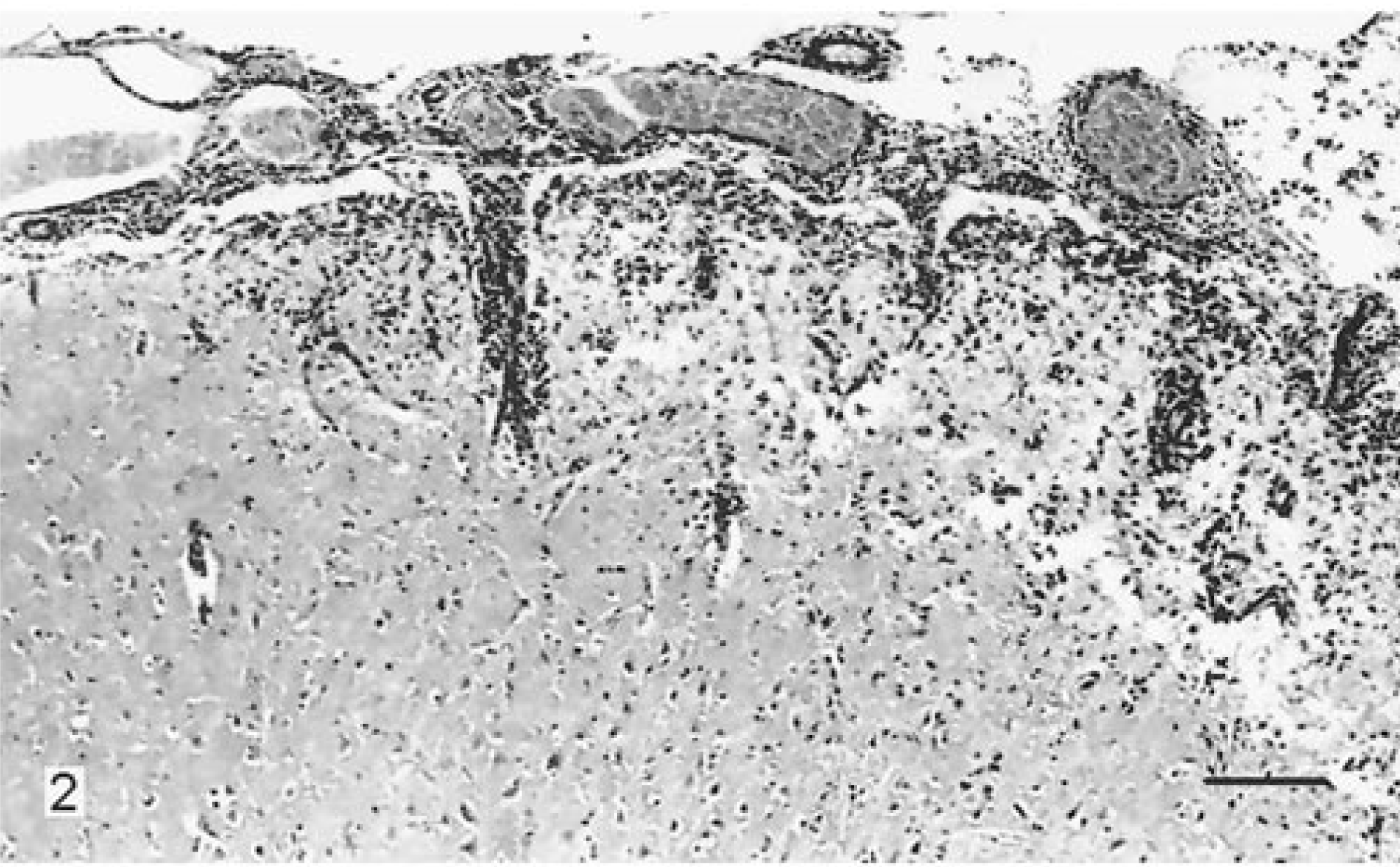
Left cerebral hemisphere; dog. There is marked infiltration of mononuclear cells in the meninges and around vessels in the parenchyma and cerebrocortical necrosis. Hematoxylin and eosin. Bar = 300 µm.
Cerebellum and lower brain stem were unaffected. Special stains (Gram and Grocott methods) did not demonstrate bacterial or fungal agents. Immunohistochemistry was negative for canine distemper encephalitis, toxoplasmosis, and neosporosis.
The architecture of the right hippocampus was replaced by a single, large layer of neural cells arranged in a closely piled gyrated ribbon resembling a polymicrogyric cortical structure with normal subcortical white matter (Fig. 3). The pyramidal cells were loosely arranged and misaligned. In the center of the hippocampus, they were intermingled with gemistocytic and fibrillary astrocytes. Within the malformed tissue there were conspicuous, randomly oriented capillaries with prominent elongated endothelial nuclei and a few small lymphocytic cuffs. A residual dentate gyrus with normal granular cells was still recognizable in the ventral hippocampal area. The left hippocampus was normal.
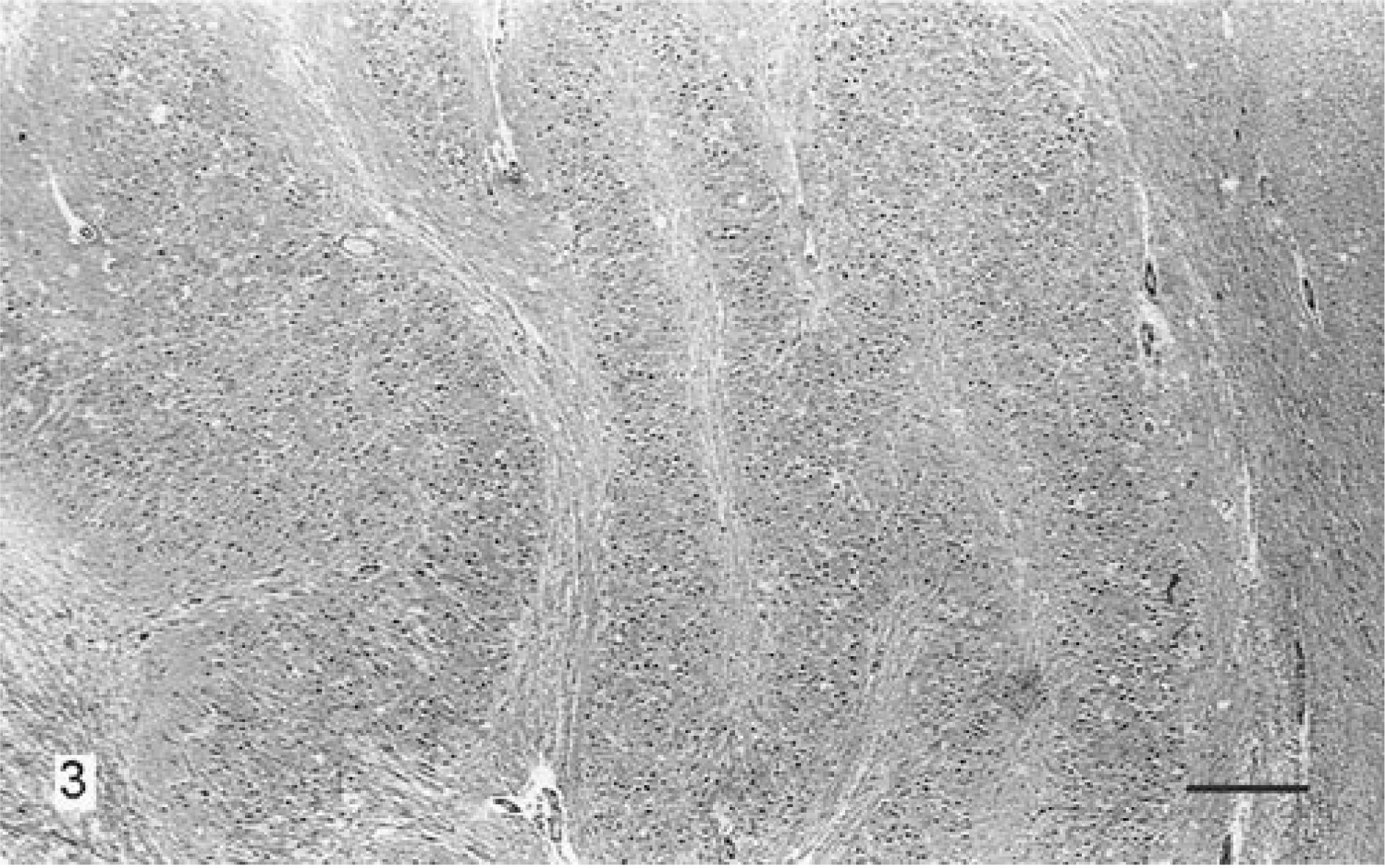
Right hippocampus; dog. The pyramidal cells are arranged in multiple convoluted gyri, piled one above the other. Hematoxylin and eosin. Bar = 1,200 µm.
At least two different, most likely unrelated, types of lesions were present in the brain of this dog: a form of necrotizing meningoencephalitis and a dysplasia in the right hippocampus, best characterized as cortical hamartia, that is, overrepresentation of tissue elements normally present in a particular location. The necrotizing meningoencephalitis was mainly located in the left telencephalic gray matter, subcortical white matter, and basal nuclei with severe infiltration of mononuclear cells and gliosis. These findings are similar to the features of necrotizing meningoencephalitis described in Pug and Maltese dogs, in which unilateral or bilateral leptomeningitis, nonsuppurative perivascular inflammation, and neuronal necrosis, as a rule without conspicuous involvement of cerebellum and lower brain stem, have been considered distinctive of the disease. 2 10 13 In our dog, the right hemisphere showed infarction-like lesions, but the presence of residual nonsuppurative inflammation suggested a primary vascular disorder was unlikely. However, a vascular malformation, possibly in connection with the hippocampal dysplasia, as cause of the development of the infarction-like lesions cannot be excluded.
Clinically, the dog of this report can be included in the group of dogs chronically affected with necrotizing meningoencephalitis. 2 These dogs usually present with generalized or partial motor seizures and are neurologically normal during the interictal period. Seizures may recur at varying intervals, and the neurological syndrome develops into a progressive form. In our dog, the neurological syndrome seemed more protracted than in the chronic form of Pug dog encephalitis, in which the maximum survival is less than 6 months from the onset of seizures. Moreover, the onset of signs in this dog was at a higher age compared to the average age of Pug and Maltese dogs. For these reasons, we presume that the inflammatory lesions may have first involved the right hemisphere, resulted in infarction-like lesions and then spread to the left hemisphere where they were still in progress. This protracted pathogenesis might be responsible for the chronic and relapsing neurological syndrome shown by the animal. It is still an open question whether necrosis is the cause of or a consequence of seizure activity, 11 but the extent and severeness of the necrotizing changes in this dog rather suggest the former.
A breed-specific necrotizing meningoencephalitis first recognized in Pug dogs (Pug dog encephalitis) in California 3 has now been diagnosed in several countries 1 4 7 13 (M. Vandevelde, unpublished). Further observations of a similar disease in Maltese, 10 Shih Tzu, 10 and Chihuahua dogs 12 indicate that this entity may be more widespread among dogs of small size, in particular toy breeds. A distinctive clinical and pathologic form of necrotizing encephalitis has also been described in Yorkshire Terriers. 6 9 12
The architecture and cytologic abnormalities of the right hippocampus were consistent with a dysplasia restricted to the hippocampal area. The lesion might be due to defective neuronal migration and differentiation during gestation. In humans, such malformative lesions predominantly affect the cerebral neocortex and have been correlated with the development of seizure activity. 5 Reports of epilepsy due to focal cortical dysplasia in animals, as well as descriptions of such neural malformation, are lacking. Seizures, in addition to other neurological signs, have been documented in animals affected with severe congenital anomalies, such as hydrocephalus, lissencephaly, and porencephaly. 8 Because the dog was already 4 years old when the first clinical symptoms were observed, we believe that the hippocampal dysplasia had no clinical consequences and hardly affected the course of the disease.
Footnotes
Acknowledgements
We thank Professor Marc Vandevelde for his comments on the histopathology of this case. This study was supported by grants from the Italian Ministry of University and Scientific Research (MURST) and the University of Pisa.