
Abstract
Cholesterol granulomas are uncommon pathologic lesions in animals, although they are important intracranial tumors in humans. This report describes cholesterol granulomas associated with multiple organ systems of three captive meerkats. In the most severe case, meerkat No. 1, the pathologic behavior of the cholesterol granuloma was unique in that it appeared to locally invade the cerebrum and calvarium, possibly contributing to neurological deficits observed antemortem. A review of other meerkat necropsies revealed incidental, asymptomatic cholesterol granulomas in organs of two other individuals, meerkat Nos. 2 and 3. Histologically, all lesions were composed of cholesterol clefts admixed with large, foamy macrophages containing hemosiderin, multinucleated giant cells, lymphocytes, plasma cells, and foci of mineralization. Hypercholesterolemia was documented in two of the three meerkats.
With the exception of the horse, cholesterol granulomas are rarely reported in animals. Up to 20% of older horses have cholesterol granulomas associated with the choroid plexuses of the lateral and/or fourth ventricles. 5 Although there is potential for expression of antemortem neurologic deficits associated with these lesions, most are found incidentally at necropsy. 5 In dogs, cholesterol granulomas have been documented intracranially, 9 in the middle ear, 2 and in the maxillary sinus. 7 In other species, they have been reported in the spinal dura of a Russian viper snake, 12 the meninges of a Cuban anole lizard, 12 multiple tissues in Cuban tree frogs 11 and leaf-tailed geckos, 3 and were described in the cerebrum of a meerkat in an Armed Forces Institute of Pathology slide set (AFIP case No. 2591775, 1996).
Cholesterol granulomas in humans are infrequent and are usually localized to cranial tissues, particularly the petrous apex, 1 the middle ear, 6 and the choroid plexus. 4 Cholesterol granulomas in humans have also been described in tissues outside the cranium, including the breast, parotid gland, peritoneum, lymph nodes, thyroglossal duct, kidneys, liver, and spleen. 10
This report describes the clinical and pathologic features of multiple cholesterol granulomas affecting three unrelated meerkats, and the possible pathophysiologic processes associated with cholesterol granuloma development are discussed.
An 8-year-old, captive-born, male meerkat (meerkat No. 1) at the North Carolina Zoological Park presented acutely depressed, lethargic, and dehydrated. Initial blood parameters were within baseline reference ranges (Table 1) for meerkats with the exception of serum cholesterol, which was greater than 520 mg/dl. Serum cholesterol remained greater than 520 mg/dl over three separate blood samples during 4 weeks of hospitalization. Radiography revealed severe osteolytic lesions associated with the dorsal cranium, cervical and thoracic spondylosis, and cardiomegaly, suggesting dilatative cardiomyopathy, which was confirmed by echocardiography. After 4 weeks of hospitalization, the meerkat developed bilateral forelimb paralysis, and due to poor prognosis, was humanely euthanized. At necropsy, the brain was firmly adhered to the calvarium by yellow, granular material, which extensively replaced the meninges and the underlying cerebral cortex (Fig. 1). The pericardium contained a small, yellow, granular plaque. Biventricular cardiac dilatation and pulmonary edema were also noted.
North Carolina Zoological Park (NCZP) and International Species Inventory System (ISIS) reference ranges for serum cholesterol concentrations in meerkats.
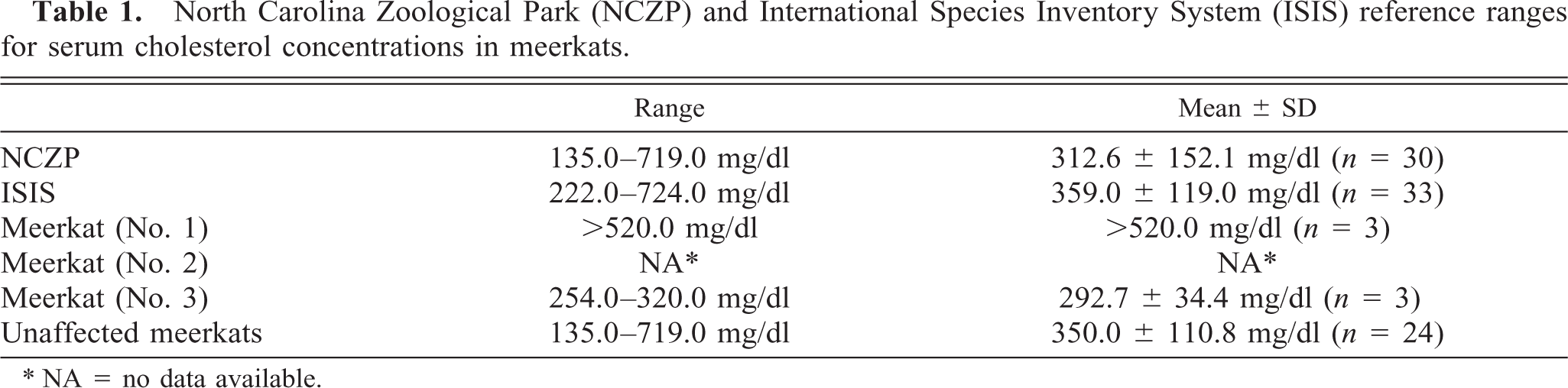
NA = no data available.
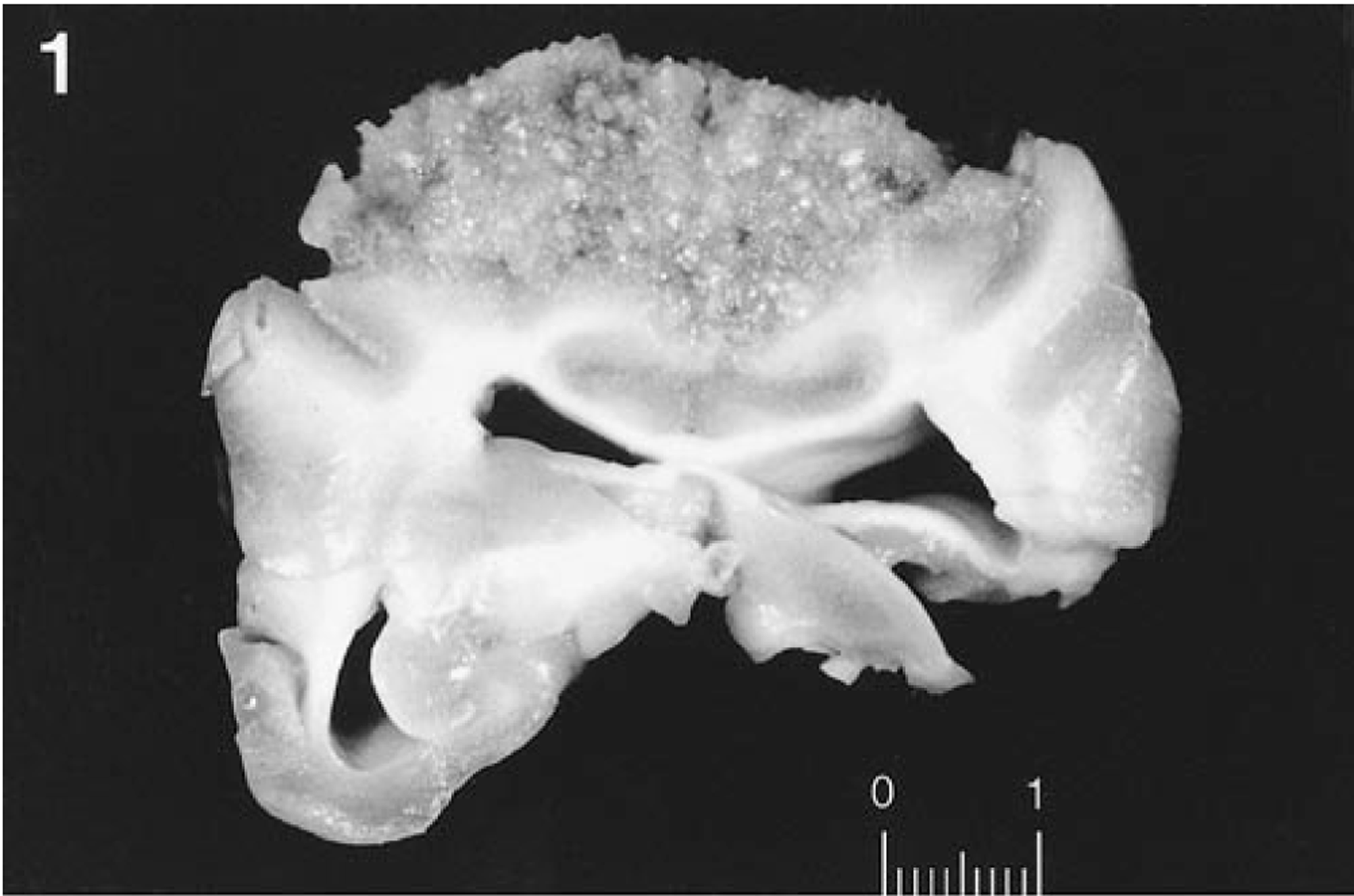
Brain; meerkat No. 1. Cholesterol granuloma effacing the cerebral architecture. Bar = 1 cm.
Histologically, the cerebrum was focally effaced and replaced by clear, elongated, irregularly arranged, cholesterol clefts surrounded by mild to moderate aggregates of foamy, hemosiderin-laden macrophages, lymphocytes, plasma cells, and multinucleated giant cells, with areas of mineralization (Fig. 2). The overlying bone of the calvarium was replaced by similar cholesterol and inflammatory aggregates (Fig. 3). The cerebellum and brainstem were unaffected. The pericardium also contained a well-circumscribed, 0.5- × 0.5-cm cholesterol granuloma. Besides the cerebral and pericardial cholesterol granulomas, histologic lesions included myocardial fibrosis and myofiber atrophy, multifocal bronchial gland adenomas, focal endogenous lipid pneumonia, and chronic interstitial nephritis.

Cerebrum; meerkat No. 1. Cerebrum eroded by elongated, irregularly arranged, cholesterol clefts surrounded by aggregates of foamy, hemosiderin-laden macrophages, lymphocytes, plasma cells, and multinucleated giant cells, with areas of mineralization. HE stain. Bar = 30 µm.

Calvarium; meerkat No. 1. Expansile, nonencapsulated, cholesterol granuloma eroding the calvarium. HE stain. Bar = 300 µm.
A 4.5-year-old, male meerkat (meerkat No. 2) born at the North Carolina Zoological Park was presented dead with no known recent medical problems. No previous hematological values were available. Histologic findings included aortic valvular and left ventricular endocarditis, multifocal cholesterol granulomas of the superficial renal cortex, and a 0.2-cm-diameter cholesterol granuloma focally expanding the pancreatic parenchyma. A single mesenteric lymph node contained a 1-cm-diameter cholesterol granuloma with adjacent erythrocytic debris. Hepatic and pulmonary congestion, splenic edema, and pancreatic atrophy were also noted.
A 10-year old, captive-born, male meerkat (meerkat No. 3) at the North Carolina Zoological Park presented with marked mandibular swelling and associated gingival hyperplasia. Only an elevated serum cholesterol (304 mg/dl and 320 mg/dl) was remarkable in two blood samples drawn 10 days apart, and serum cholesterol was also elevated on serum chemistries performed 2.5 years earlier during clinical assessment of an unrelated medical problem (Table 1). Biopsy of the gingival lesion revealed squamous cell carcinoma, and the meerkat was humanely euthanized. Findings at necropsy included a large, invasive, moderately well-differentiated squamous cell carcinoma that extended into the adjacent bone and skeletal muscle with metastases to the left submandibular lymph node and right middle lung lobe. The spleen contained a focal, circumscribed cholesterol granuloma. Other diagnoses included aortic atherosclerosis, coronary endarterial calcification, biliary cysts, and chronic renal infarcts.
Cholesterol granulomas are considered to be benign, well-circumscribed, and typically asymptomatic lesions, often described incidentally at necropsy. The most common pathologic behavior of a cholesterol granuloma is slow expansion with relatively little destruction of surrounding tissue. 5 However, severe compression of adjacent tissues or obstruction of cerebrospinal fluid outflow can cause overt clinical signs. All but one of the cholesterol granulomas described in these cases were small, well-circumscribed, asymptomatic lesions, but the cerebral lesion in meerkat No. 1 was quite atypical and was initially thought to be a neoplastic process. The cholesterol granuloma was not well-circumscribed and had the unusual gross and histologic appearance of invasive projections penetrating surrounding brain parenchyma, destroying the meninges, overlying periosteum, and calvarium. This meerkat developed profound neurological deficits, possibly due to the marked compression and destruction of cerebral tissue, but chronic cervical and thoracic spondylosis may have contributed to some of the observed deficits as well. Although bone destruction as a sequela has been ascribed to expanding cholesterol granulomas, the authors are unaware of descriptions in the literature of cholesterol granulomas having invasive pathophysiologic behavior.
The pathogenesis of cholesterol granulomas has not been clearly elucidated. The most common hypothesis is that cholesterol granulomas develop at sites of hemorrhage and/or tissue necrosis secondary to an inflammatory focus. 1 5 An association between inflammation/hemorrhage and cholesterol granuloma formation in the meerkats described in this report is unconvincing. In meerkat No. 2, the cholesterol granuloma within the mesenteric lymph node contained erythrocytic debris, implying previous hemorrhage. However, the etiology of the remaining granulomas in all three cases are not well supported by the inflammation/hemorrhage hypothesis.
Alternatively, elevated serum cholesterol may predispose individuals to the development of cholesterol granulomas. Rabbits fed a lipid-rich diet appear to be predisposed to developing cholesterol granulomas of the choroid plexus. 8 In humans, there is an association between hyperlipidemia (elevated cholesterol and triglycerides) and the development of cholesterol granulomas of the choroid plexus. 8 An association between hyperlipidemia and hypercholesterolemia and the development of disseminated xanthomatosis has also been described in leaf-tailed geckos and Cuban tree frogs. 3 11 Two of three meerkats with cholesterol granulomas presented in this paper had elevated serum cholesterol concentrations relative to the expected baseline range of other mammalian species. Our own baseline reference data on this colony, as well as data reported by the International Species Inventory System (ISIS), suggests that elevated serum cholesterol concentrations may be typical in captive meerkats (Table 1).
The causes of elevated serum cholesterol in captive meerkats are unknown but could be a function of diet, inborn errors of lipid metabolism, or adaptive species-specific physiology. Without knowledge of serum biochemical values of free-ranging meerkats, we cannot determine whether elevated serum cholesterol concentration in this species is physiologically normal or a consequence of captive management. The three individuals presented in this report were not known to be genetically related, reducing the likelihood of a familial genetic trait predisposing to hypercholesterolemia and/or cholesterol granuloma formation. During the past 10 years, meerkats at the North Carolina Zoological Park have been fed a combination of a commercial processed meat diet and a commercial dry dog food, supplemented with hard-boiled eggs, and a variety of fruits and vegetables. This diet is relatively high in animal fat. The three meerkats described in this report were maintained on this diet throughout their lives. Consumption of a diet high in saturated fat and cholesterol may predispose captive meerkats to hypercholesterolemia and associated pathologic sequelae, including cholesterol granuloma development. Further exploration of dietary and species-specific metabolic factors will be necessary in order to determine whether a causal relationship underlies cholesterol granuloma formation in captive meerkats at the North Carolina Zoological Park.
Footnotes
Acknowledgements
We gratefully acknowledge M. K. Stoskopf and S. Kennedy-Stoskopf for review of the manuscript and W. Savage and an anonymous reviewer for providing excellent suggestions.