
Abstract
An 8-y-old Labrador Retriever dog had mild ataxia of the hindlimbs 4 mo after lumbosacral dorsal laminectomy for intervertebral disk disease. Ataxia of the hindlimbs gradually worsened over the next 6 y. On autopsy, gross lesions were not recognized in the spinal cord. Histopathology revealed an intradural extraparenchymal cholesterol granuloma in the cauda equina associated with remnant nerve roots. Nerves associated with the cholesterol granuloma had axonal degeneration, myelin vacuolation, and edema. In those foci, macrophages were increased in number between nerve fibers. Immunohistochemistry for neurofilament protein and Luxol fast blue staining highlighted the presence of remnant axons and myelin sheaths within the granuloma. Inflammatory cell infiltrates in the granuloma were mainly macrophages and CD3- or CD20-immunopositive T or B lymphocytes, respectively. We conclude that the cholesterol granuloma likely formed subsequent to degenerative neuropathy in the cauda equina.
Cholesterol crystals are typically detected in tissue with chronic hemorrhage or necrosis; the deposition of cholesterol crystals results in the formation of cholesterol granulomas (tumor-like cholesteatomas). 10 Cholesterol granulomas in the nervous system are most common in the choroid plexus of the fourth or lateral ventricle of aged horses, 3 and have also been reported in the CNS of other animals, including the fourth ventricle of a dog, 7 longitudinal cerebral fissure of a cat, 4 supracallosal sulcus of a cat, 14 and the parietal lobe and meninges in meerkats.1,15 However, the spontaneous formation of a cholesterol granuloma in the peripheral nervous system is extremely rare, and has been reported only once in a dog in a lumbar nerve root where it was associated with localized degenerative neuropathy. 13 We report here a canine case of intradural extraparenchymal cholesterol granuloma associated with the nerves of the cauda equina.
An ~8-y-old, castrated male, Labrador Retriever dog was presented to the Veterinary Medical Center of Obihiro University of Agriculture and Veterinary Medicine (Hokkaido, Japan) with a 3-mo history of intermittent ataxia of the hindlimbs. Computed tomography (CT) with intrathecal contrast medium showed protruding disk material that compressed the spinal cord between L7 and S1. Dorsal laminectomy at L7-S1 was performed, and soft tissue, considered to be degenerate disk material, was removed. After the excision, the vertebral arch was fixed to the vertebral body with bone cement and 2 screws. Excised tissue was not examined histologically. The postoperative course was favorable, and ataxia of the hindlimbs disappeared. However, mild ataxia of the right hindlimb was noted ~4 mo after surgery. Similar clinical signs subsequently developed in the left hindlimb. Physical examination revealed decreased proprioception in both hindlimbs. No other abnormalities were detected by clinical examination, including blood and urine tests. Over the next 6 y, ataxia of the hindlimbs gradually worsened. The dog also had polydipsia and polyuria for 1 y prior to death, however, the precise cause of those clinical signs was not determined. Terminally, the dog was lethargic and anorectic, and died naturally at ~14-y-old.
Autopsy was performed the day after death. To perform a gross examination of the spinal cord and spinal canal, the vertebral arches from C1 to L7 were resected and the spinal cord was removed. The dorsal vertebral arch of L7 had been firmly fixed to the vertebral body by 2 screws from the transverse processes on each side. The area fixed with the screws was separate from the spinal canal, and there were no gross lesions in the spinal cord that were recognized from outside the dura mater. Furthermore, no significant changes were observed in the lumbosacral spinal canal. Hindlimb musculature was atrophic.
Samples from major organs were fixed in 15% neutral-buffered formalin and processed routinely; 3-µm thick sections were stained with H&E for histologic examination. Luxol fast blue (LFB) staining and immunohistochemistry (IHC) were also performed to characterize the lesion in the cauda equina. IHC was conducted with primary antibodies specific for CD3, CD20, Iba1, neurofilament protein light-chain, neurofilament protein heavy-chain, and myelin protein zero (Table 1). Sections were incubated with each primary antibody at room temperature (RT) for 2 h after antigen retrieval (Immunosaver; Nisshin EM) at 98°C for 45 min and endogenous peroxidase blocking. Sections were then incubated with a secondary antibody (MAX-PO polymer reagent; Nichirei Bioscience) at RT for 30 min, and the binding of the antigen and antibody was visualized with 3,3′-diaminobenzidine (DAB; Nichirei Bioscience). Double immunofluorescence (IF) using anti–neurofilament protein heavy-chain and anti–myelin protein zero antibodies was also performed. Sections were incubated with a mixture of the primary antibodies at RT for 2 h, and then incubated with a mixture of the secondary antibodies (Alexa Flour 488–conjugated goat anti-mouse IgG [1:200 dilution], Alexa Fluor 594–conjugated goat anti-rabbit IgG [1:200 dilution]; Thermo Fisher) at 37°C for 30 min. As a negative control, primary antibodies were replaced by a mouse IgG1 (Dako) or rabbit Ig fraction (Dako), depending on the host of the primary antibodies. Nerve bundles in the cauda equina sampled from a 14-y-old male French Bulldog, which had no neurologic signs and died of interstitial nephritis and pulmonary edema, were used as a control for comparison with the results of IHC and IF.
Antibodies used to investigate a cauda equina cholesterol granuloma in a dog.
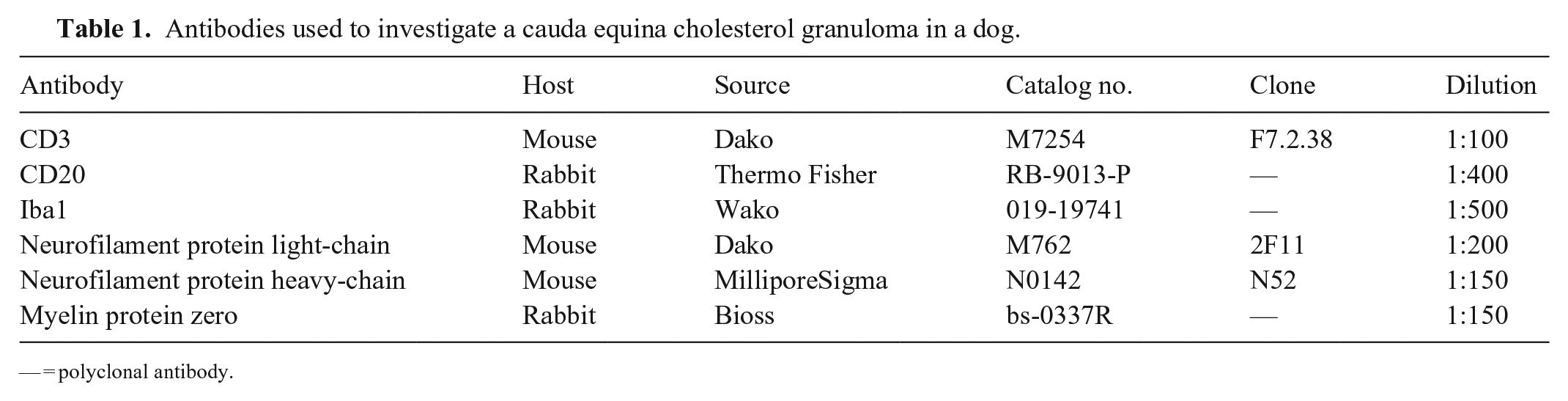
— = polyclonal antibody.
H&E-stained sections of the cauda equina (L7) revealed an intradural extraparenchymal mass on the left side that was associated with the spinal nerves (Fig. 1A). The mass consisted of a fibrous tissue network with numerous irregularly and variably sized sheaves of needle-like cholesterol clefts associated with an inflammatory cell infiltrate (Fig. 1B). Inflammatory cells were mainly macrophages with abundant eosinophilic cytoplasm (Iba1-positive) and T (CD3-positive) or B (CD20-positive) lymphocytes; a few multinucleate giant cells were also observed. Based on those findings, the mass was diagnosed as a cholesterol granuloma. Nerves surrounding the cholesterol granuloma had multifocal myelin vacuolation and accumulation of eosinophilic serous fluid between separated nerve bundles (Fig. 1C, 1D), which were observed ipsilateral (left side) and contralateral (right side) to the granuloma, and were more severe in nerves on the right side (Fig. 1D) than on the left side (Fig. 1C). In the section of cauda equina caudal to L7, there was focal macrophage and lymphocyte infiltration (Fig. 1E). Axonal degeneration, consisting of multifocal vacuolation and myelin ovoid formation, was also detected in those foci (Fig. 1F). Therefore, the cholesterol granuloma was suspected to be associated with degenerate nerves. These histologic lesions were not observed in the control dog.
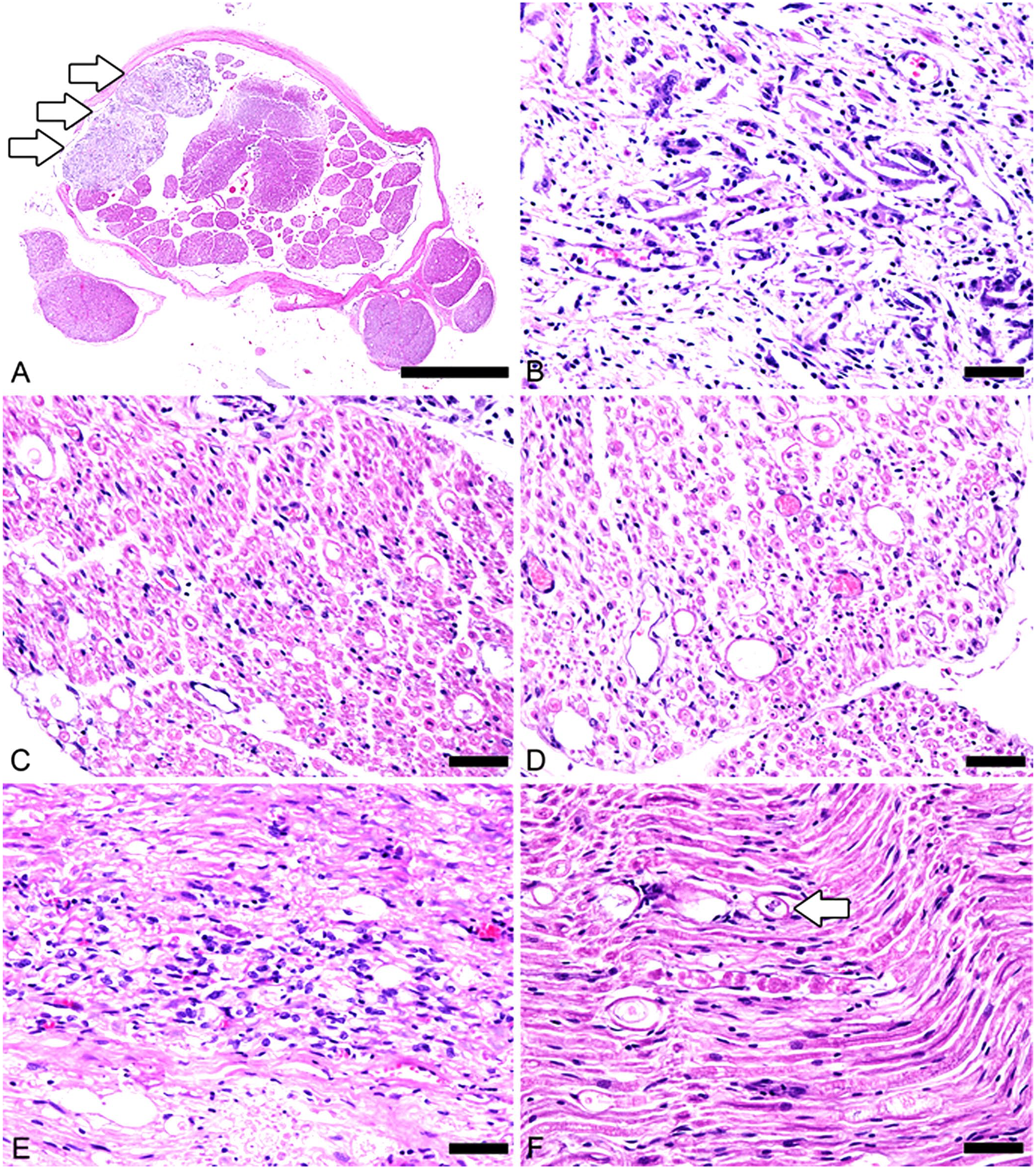
Cholesterol granuloma and surrounding nerves in the cauda equina of a dog.
The results of LFB staining revealed remnant myelin sheaths within the cholesterol granuloma (Fig. 2A). Furthermore, a few remnant axons immunolabeled for neurofilament protein light-chain were also detected within the granuloma (Fig. 2B). Those results indicated that the cholesterol granuloma was associated with nerves of the cauda equina. In nerves surrounding the cholesterol granuloma, double IF with neurofilament protein heavy-chain and myelin protein zero antibodies indicated a lower density and more heterogeneous diameters of axons and myelin sheaths (Fig. 3A–C) than those in the control case (Fig. 3E–G). A few Iba1-positive cells were detected between nerve fibers in the control case (Fig. 3H). The number of Iba1-positive cells between nerve fibers was higher in our case, and clusters of Iba1-positive cells were observed multifocally (Fig. 3D). The cervical, thoracic, and lumbar nerve roots and both sciatic nerves were also examined, and some sections were subjected to IHC. Mild vacuolation was observed focally in the sciatic nerves; however, no obvious histologic changes were observed in the cervical, thoracic, and lumber nerve roots compared to those of the control dog. The spinal cord segments from C1 to L7 were also evaluated histologically, and no significant changes were found. There were small groups of atrophic muscle fibers in both hindlimbs.
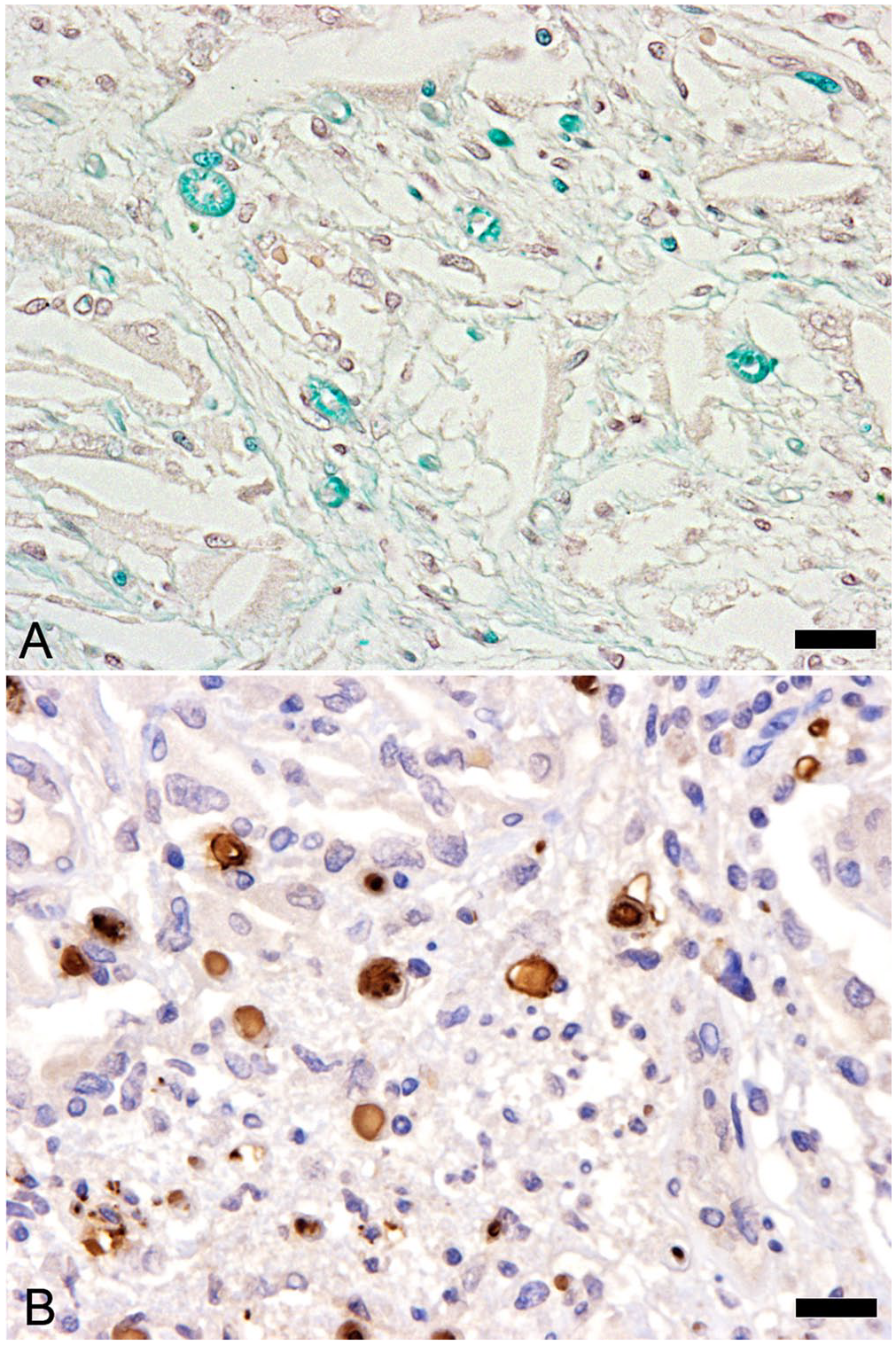
Cholesterol granuloma in the cauda equina of a dog.
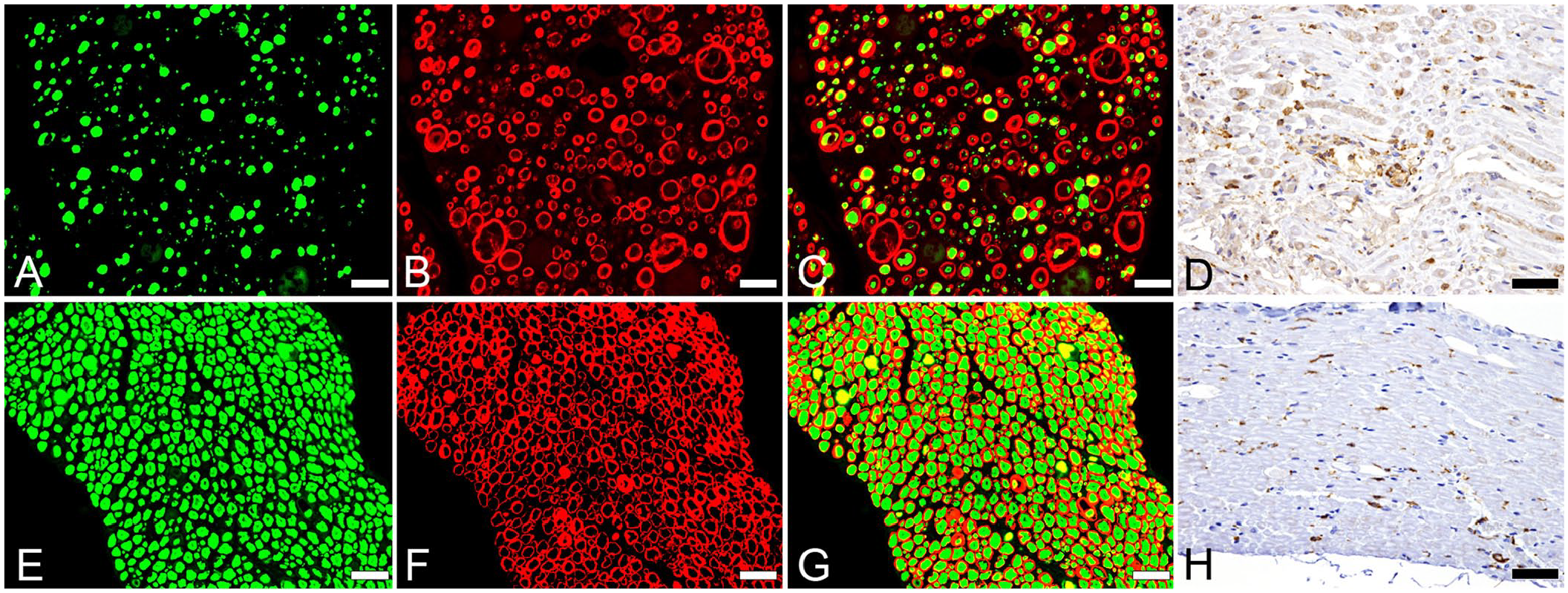
Nerves surrounding the cholesterol granuloma in the cauda equina of a dog (
Comorbid pathologic findings were bilateral adrenocortical adenomas, renal secondary hyperparathyroidism, mineralization of blood vessels in the lung and kidney, pulmonary edema, splenic hematomas, and subcutaneous lipomas.
Based on the results of CT and the postoperative course after herniated disk removal, ataxia of the hindlimbs prior to surgery appeared to be the result of intervertebral disk protrusion. Four months after surgery, hindlimb ataxia reappeared initially on the right side. Although the cholesterol granuloma was observed on the left side of the cauda equina, axonal degeneration was detected bilaterally in the nerve bundles of the cauda equina and was most severe on the right side. Therefore, postoperative ataxia may have been caused by degenerative neuropathy in nerves of the cauda equina, and the cholesterol granuloma was not directly related to the clinical signs.
Nerve bundles had axonal degeneration and accumulation of eosinophilic serous fluid between nerve bundles, which was interpreted as edema. Edema is a characteristic histologic finding in the acute stage of inflammation. 12 Paraplegia persisted in our case for several years; the edema observed may indicate the ongoing nature of the inflammation in the affected nerves.
Cholesterol crystals act as foreign bodies, and typically induce granulomatous inflammation. 10 Cholesterol granuloma in the nervous system is often encountered in the choroid plexus of the fourth or lateral ventricle of aged horses. 3 There are few case reports of cholesterol granuloma in peripheral nerves. Cholesterol granuloma has been reported in the lumbar nerve root of a dog 13 and in sural nerves of guinea pigs. 5 In the canine case, 13 the cholesterol granuloma had formed in association with chronic inflammatory demyelinating polyradiculoneuropathy (CIDP). Myelin is rich in cholesterol, and a study on damaged optic nerves in rats indicated that injured myelin was transformed into cholesterol crystals. 6 Cholesterol crystals in the canine case report 13 were attributed to the destruction of myelinated nerve fibers secondary to inflammation in CIDP.
The common histologic characteristics of CIDP in humans include axonal degeneration, edema, perivascular or endoneurial infiltration of lymphocytes and macrophages, and onion bulb formation resulting from repeated demyelination and remyelination. 9 Although the occurrence of CIDP in veterinary medicine is rarer than in humans, histologic findings similar to those in humans have been reported in dogs and cats with CIDP.2,11 Nerve bundles in our case had axonal degeneration and accumulation of eosinophilic serous fluid between nerve bundles, which was interpreted as edema. Aggregates of macrophages were observed in our case in the nerve bundles surrounding the cholesterol granuloma. Onion bulbs, which are rare histologic findings in human cases of CIDP, 8 were not detected in our case. Based on these findings, we speculate that the degenerative neuropathy observed in our case was a manifestation of CIDP. However, the diagnosis of CIDP in human medicine is based on the findings of various clinical and laboratory examinations, including biopsy. 16 Therefore, reaching a definitive diagnosis of CIDP based on histologic examination alone is difficult. Given that the histologic findings in our case were not specific to CIDP, we were unable to identify a precise association with CIDP.
To the best of our knowledge, there are no reports of cholesterol granulomas in CIDP-affected nerves in humans. On the other hand, cholesterol granuloma arising from CIDP-affected nerves has been reported in a Labrador Retriever dog, 13 which is the same breed as our case. Assuming that the degenerative neuropathy observed in our case was the result of CIDP, CIDP in dogs, especially in Labrador Retrievers, may not be identical to CIDP in humans, and may be a new aspect of CIDP in dogs. In addition, we also need to consider the contribution of surgery on the lumbosacral region to the degenerative neuropathy and the formation of cholesterol granuloma given its clinical course. Nevertheless, the granuloma in our case appeared to be caused by the destruction of myelin sheaths, similar to the previous canine case report. 13
Footnotes
Acknowledgements
We thank Ms. Akiko Tomikawa for her technical support with histologic processing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.