
Abstract
In order to determine the existence of glomerular lesions in Saimiri boliviensis, renal biopsies were performed in 20 clinically healthy animals of similar age and both sexes. Biopsies were obtained by laparotomy with a Tru-Cut biopsy needle. Mesangioproliferative glomerulonephritis characterized by an increased number of mesangial cells and increased mesangial matrix was present in 35% of the animals. Proliferative glomerulonephritis characterized by increased numbers of epithelial and endothelial cells with narrowed capillary lumen, and membranous glomerulonephritis characterized by diffuse thickening, wrinkling, and occasional lamellation of basement membranes, were present in 15% of the samples. Ultrastructural features included increased mesangial matrix, fusion of the visceral epithelial foot processes, thickened glomerular basement membranes, and incipient lamellation. Immunohistochemical examination revealed granular deposits of immunoglobulin M in the cytoplasm of mesangial cells and in the mesangial matrix in 50% of the samples.
Various renal lesions have been described in Old World 6 12 16 30 and New World primates, 5 7 9 14 15 25 30–32 in wild as well as in captive animals. As with other kidney conditions, glomerular lesions have been seen in many different monkey species and age ranges. The severity of glomerular changes varies from solitary minor lesions to extensive forms of glomerulonephritis. 30
In the Old World monkeys Macaca mulatta, solitary hyalinized and sclerosed glomeruli, proliferative arteriopathy with eccentric nodular thickening, and disoriented proliferating cells, accompanied by abundant mononuclear cellular infiltrate, have been described. 30
Mesangioproliferative glomerulonephritis (GN) has been recognized in apparently normal Macaca nemestrina. 6 12 30 These lesions have different degrees of severity. Histological changes consist of increased number of mesangial cells and matrix, with thickening of the capillary walls. 6 12
Ultrastructural and immunofluorescence studies in Macaca nemestrina suggested that renal lesions might be a consequence of immune complex deposits (immunoglobulin [Ig] M antigens) in the mesangial region. 6 Immunofluorescence studies have demonstrated glomerular depositions of IgA, IgG, and particularly IgM. 12 Direct immunofluorescence studies in Papio cynocephalus detected granular deposits of IgG, IgM, IgA, and complement fractions C3 and C4 in the glomeruli. 16
The New World primates are also susceptible to various renal conditions. 7 9 15 30 In the Callithricidae family, mesangioproliferative nephropathy is described; it is characterized by increased numbers of mesangial cells, amount of mesangial matrix, and reticular fibers. 7 25 The disease remains subclinical for long periods but it is progressive. It is responsible for, or is at least related to, death in 20% of animals. 7 8 In the same family, mesangial sclerosis, proliferation, fibrosis of the Bowman capsule, and glomerular sclerosis associated with hematuria, proteinuria, and urinary casts have been described. 25 In Aotus trivirgatus, the most common renal lesion is an immune-mediated GN associated with hemolytic anemia. The most common lesions include mesangial cell proliferation, increase of mesangial matrix, duplication of basal membranes with thickening of the capillary walls, and glomerular sclerosis. 15 30 32 Immunofluorescence studies in the Callithrichidae family demonstrated the presence of IgM among the mesangial cells and mesangial matrix. 7 8 25 This finding suggests that the lesion may be mediated by immunological mechanisms. 7 9
Immunohistochemical studies conducted in the Callithricihidae family indicate that IgM complexes are the primary immunoglobulin present in 100% of cases. IgM complexes are present in different sites. 7 According to Couser and Stilmant, 11 mesangial deposits of IgM precede and probably lead to glomerular lesions, whereas Bolton et al. 4 indicate that IgM deposition is independent of glomerular lesions in aged rats. It has been proposed that the antigens provoking the IgM responses in Callithrix jacchus may vary considerably and may have an environmental, dietary, or infectious origin. 8
In the squirrel monkey Saimiri boliviensis, GN are classified in four types: focal sclerosing, membranoproliferative, membranous, and a combination of membranoproliferative and membranous. 27 31 In humans, primary diffuse mesangial proliferative GN occupies a preponderant place in the histopathological classification of glomerulopathies. 22 Immunofluorescence findings include diverse combinations of IgG, IgM, complement fractions, and fibrinogen. 20 23 29 When IgA predominates, usually the condition is considered separately and designated as IgA nephropathy. 1 21 In the last years, a primary mesangial proliferative GN with IgM predominating on immunofluorescence has been described and considered as a distinct clinicoimmunopathological entity. 2 10 21
The diversity of glomerular lesions described by several researchers in different species of primates on occasions associated with meaningful clinical alterations led us to hypothesize that the same could occur in S. boliviensis. The purposes of this study were to characterize the morphologic features of glomerular lesions in apparently healthy primates of the species S. boliviensis, as well as to assess the quality of renal biopsies obtained with a Tru-Cut needle.
Materials and Methods
Renal biopsies were carried out on 20 clinically healthy primates of the species S. boliviensis. The animals were between 8 and 10 years old. There were 9 female and 11 male primates, with body weights ranging between 650 and 900 g. The animals belonged to a colony established in the Argentinean Primate Center (APC) in 1980. They were housed in 15-m3 outdoor cages in harems of two male with six to seven female primates. The monkeys were fed with a balanced food containing at least 24% proteins, 3% fat, 5.5% fiber, 0.7% calcium, and 0.6% phosphorus and supplemented with vitamins and minerals. Each animal received daily an amount of this food equivalent to 9% of its body weight. Seasonal fruit, especially oranges, were also provided. Water was available ad libitum. The animals were clinically examined once a month, and clinical blood tests were done twice a year as a routine.
Urinalysis and serum determinations (creatinine, urea nitrogen, total protein, albumin, calcium, and phosphorous) were performed immediately before renal biopsies at the APC, and histopathological studies were done by the faculty of veterinary science.
The biopsy procedure was performed under general anesthesia using ketamine (13 mg/kg) and xylazine (6 mg/kg). Animals were placed in right lateral recumbency, and the costal arch was clipped, cleaned, and disinfected. A disposable True-Cut (Baxter Laboratory) biopsy needle was introduced into the abdominal cavity through a small skin incision. The left kidney was then immobilized by manual fixation through the abdominal wall, and the needle was inserted into the kidney and guided along the long axis within the renal cortex. After biopsy, each animal was placed in an indoor cage, and follow-ups were performed during 1 week. Clinical evaluation and sampling in this study were completed in 1 month.
The samples were fixed in 10% neutral buffered formalin. Each sample was divided into halves. One of these was embedded in plastic (Technovit), cut to 1 μm thick, and stained with hematoxylin and eosin, toluidine blue, periodic acid–Schiff, Masson trichromic modified by Goldner, and Movat silver technique. The other half was embedded in paraffin (Paraplast) and cut to 3–6 μm thick for immunostaining using StrepABComplex/HRP Duet, Mouse/Rabbit (Dako Laboratories) in order to demonstrate deposits of IgG, IgA, and IgM. Rabbit antibody against human IgA and IgG (Dako), human IgM (Sigma Chemical Company) and biotinylated goat antibodies against rabbit were used as primary and secondary antibodies, respectively. The immunoreaction was visualized by 3,3-diaminobenzidine tetrahydrochloride (Sigma) and hydrogen peroxide solution.
For ultrastructural study, small pieces 0.5 to 1 mm in diameter were refixed in 3% glutaraldehyde, postfixed in 1% osmiun tetroxide, and embedded in epoxy resin (Poly Bed, Polyscience). Ultrathin sections were stained with uranyl acetate and lead citrate and observed under a transmission electron microscope (JEM 1200-1200Ex, JEOL).
Glomerular lesions were grouped taking into account a descriptive criterion. According to the involved histological component, they were classified into mesangial GN, proliferative GN, membranous GN, glomerular fibrosis, and glomerular hyalinosis. According to their extent in individual glomerulus, they were classified into global and segmental. The severity of glomerular lesions was determined, taking into account a subjective gradation, and were classified as slight (+), moderate (++), and severe (+++).
Results
Laboratory findings
Serum and urine analysis did not show any abnormalities.
Light and electron microscopy
Renal biopsies permitted us to obtain cylinders that varied from 4 to 12 mm long × 1 mm thick. Each sample contained between 6 and 19 glomeruli, with an average of 10 glomeruli per section. The results of histological study of renal biopsies are summarized in Table 1.
Histopathological characterization of glomerular lesions in renal biopsies from 20 Suaimiri boliviensis.∗
GN = glomerulonephritis; - = no staining; + = slight lesions or minor amounts; ++ = moderate lesions or moderate amounts; +++ = severe lesions or large amounts.
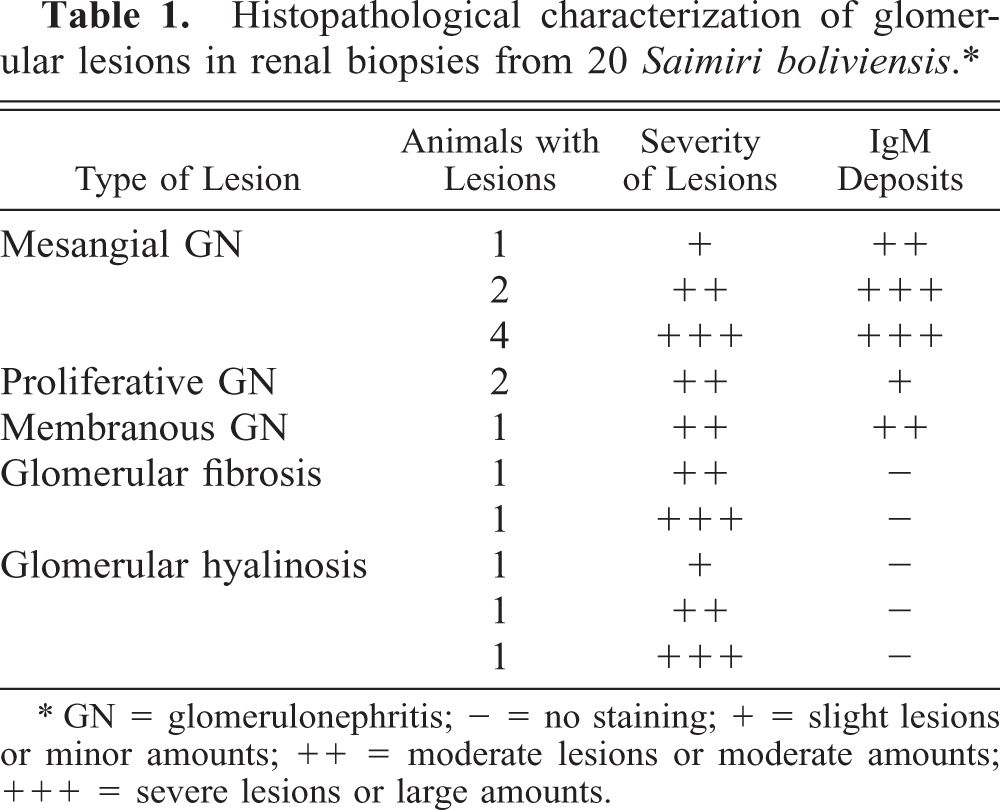
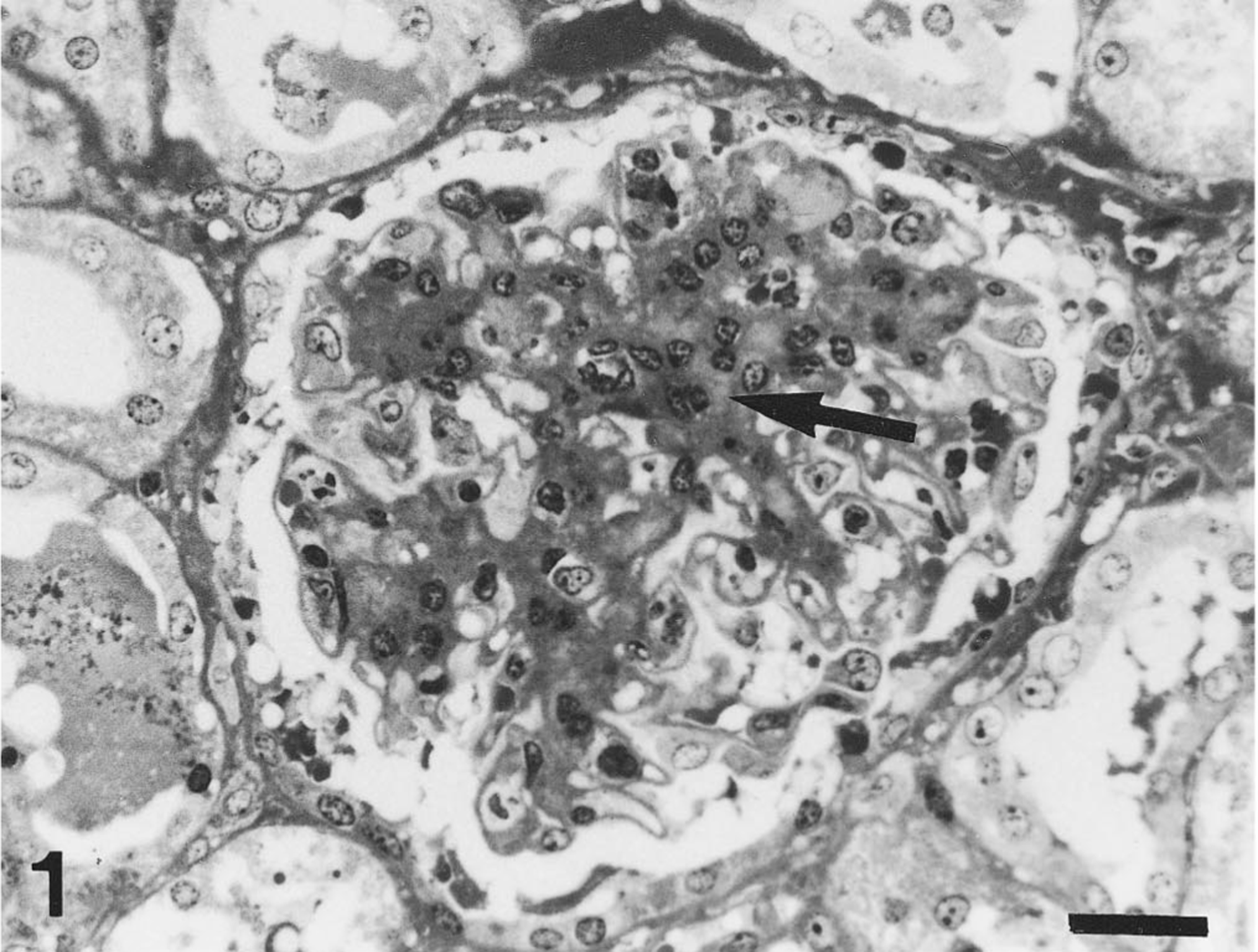
An increase in mesangial matrix was the predominant glomerular lesion. The glomeruli were affected in global or segmental forms (Fig. 1). The increase in mesangial matrix was confirmed through ultrastructural studies (Fig. 2). The presence of a granular deposit of IgM in the mesangial region was demonstrated in all seven biopsies in which mesangial GN was diagnosed. Occasionally, an increase in mesangial matrix and mesangial cells in the hiliar glomerular zone was observed.
Kidney. Glomerulus with increase of mesangial matrix (arrow) in global mesangioproliferative glomerulonephritis. Semithin section, toluidine blue stain. Bar = 25 μm.
Kidney. Transmission electron micrograph of a glomerulus. Note increase of mesangial matrix (MM); increased numbers of mesangial cells are also noted in mesangioproliferative glomerulonephritis. Bar = 2 μm.
In lesions characterized by cellular proliferation, an increased number of epithelial and endothelial cells with narrowed capillary lumen were seen. Epithelial cell proliferation with crescent formation occupying a sector or all the subcapsular space and involving the parietal epithelium of the Bowman capsule was evident.
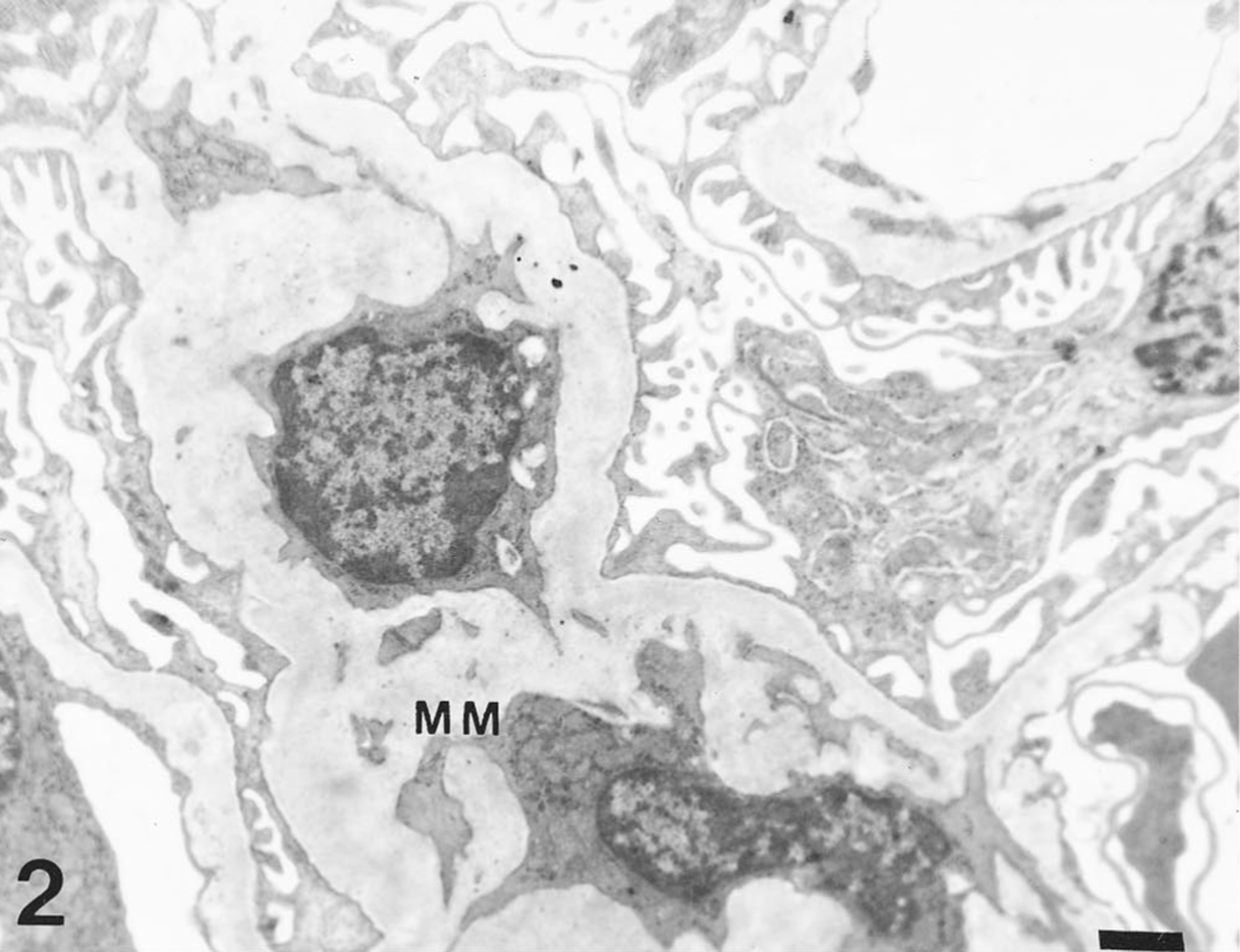
Glomerular basement membrane lesions were present in fewer glomeruli than were mesangial lesions. They were characterized by diffuse thickening, wrinkling, and occasional lamellation of basement membranes, in association with other glomerular conditions and chronic inflammatory processes of the renal interstitium (Fig. 3).
Kidney. Glomerulus with focal double countour of glomerular basement membranes (arrows) in global membranous glomerulonephritis. Semithin section, Movat silver stain. Bar = 25 μm.
Ultrastructurally, fusion of the visceral epithelial processes foot was seen, as was thickening of basement membranes of the capillary walls with incipient lamellation. Electron-dense deposits in the mesangium, subepithelium, and subendothelium were not observed.
Other lesions, including fibrosis and glomerular hyalinosis, were observed. Glomerular fibrosis was characterized by external or internal lamellar proliferation of the Bowman capsule occupying the subcapsular space, with atrophy and fibrosis of the glomerulus. The glomerular fibrosis had a focal and segmental distribution. The presence of mesangial collagen fibrils was demonstrated upon electron microscopical examination.
Glomerular hyalinosis was more frequent than glomerular fibrosis. It was characterized by the presence of ischemic, collapsed, and obliterated capillary loops. Replacement of the glomerular tuft by a hyaline mass occurred in advanced lesions. These findings were always associated with glomerular fibrosis, and chronic interstitial lesions were characterized by fibrosis and lymphoplasmacytic infiltration.
Immunohistochemistry
Neither IgA nor IgG were demonstrated in biopsy samples. IgM was detected in 10 of the 20 biopsies (50%), as evidenced by the presence of brown granular deposits in the cytoplasm of mesangial cells and in the mesangial matrix (Fig. 4; Table 1). In one of them, in addition to the mesangial distribution, fine, granular deposits of IgM along the glomerular capillary walls were evident.
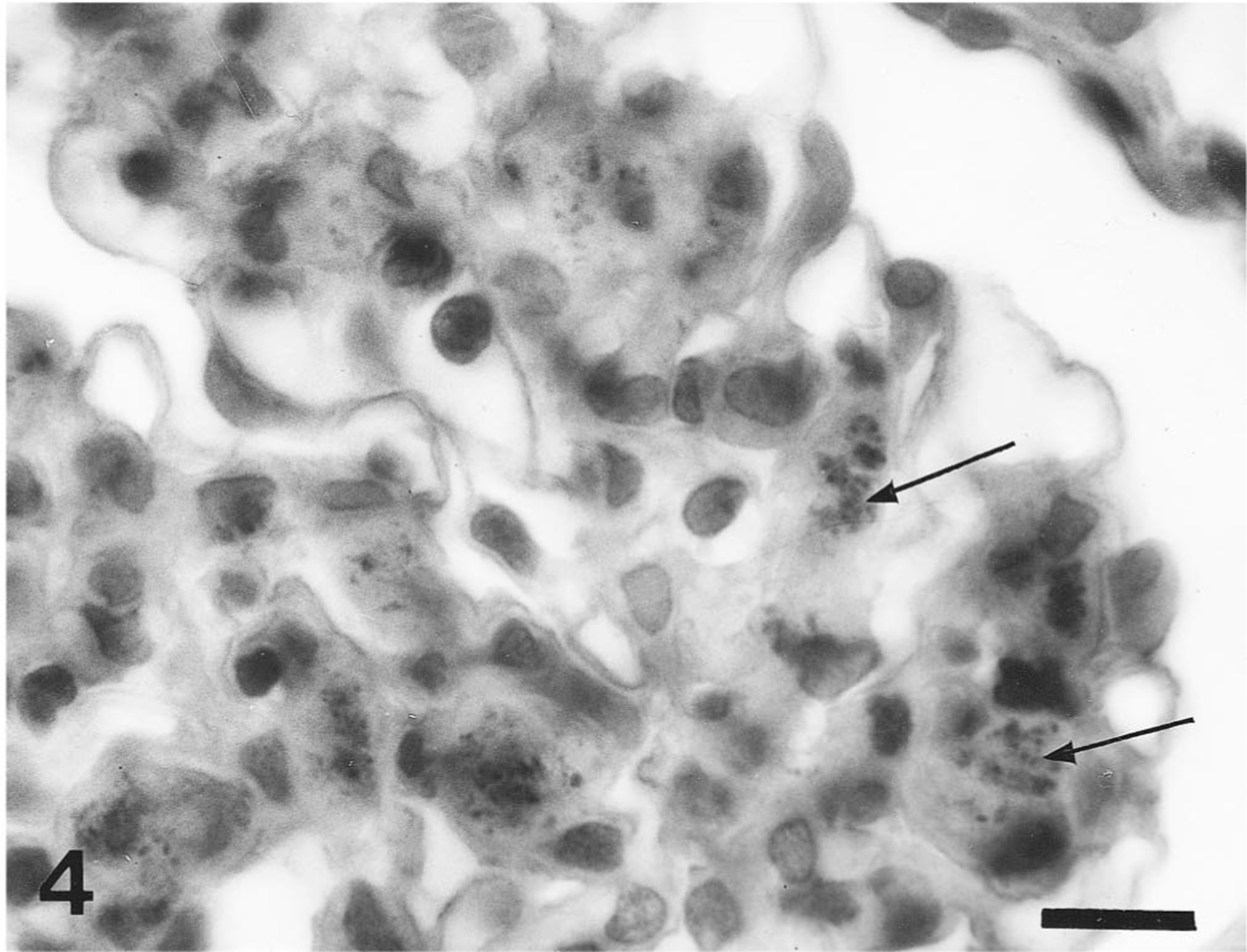
Glomerulus with IgM deposits (arrows) in mesangioproliferative glomerulonephritis. Immunohistology, avidin–biotin complex method. Bar = 10 μm.
Discussion
For biopsy purposes, the left kidney was selected because in S. boliviensis it is usually located more caudally than the right. Despite limitations of renal biopsy for the detection of medullary and pelvic lesions, the quality of samples collected for this report was adequate to make a reliable diagnosis in all of the samples. Seventy-five percent of the biopsies in this study had glomerular lesions. The most frequently observed condition (35% of the samples) was mesangioproliferative GN. These findings are coincident with those described in tamarins and marmosets (New World primates). 7 9
Most glomerular lesions in humans occur in the mesangial area. 28 The mesangium is the most sensitive structure of the glomerulus. It is the first to react to irritation, with an increase in mesangial matrix and in the number of mesangial cells, and it is the last to return to normalcy after other glomerular pathologic changes have disappeared. 28 In humans with interstitial nephritis and mesangioproliferative GN, blood circulation and renal function can be normal. 3 19 28 It can be assumed this is also true for S. boliviensis, as no signs of disease or laboratory abnormalities were present in the animals in this study despite the existence of renal lesions.
IgM deposits were recognized in all samples presenting mesangioproliferative GN in this study. Similar observations have been made in tamarins and marmosets. 7 9 Some authors support that the antigens provoking the IgM responses may have an environmental, dietary, or infectious origin. 8 13 Although some researchers have proposed that in aged rats, mesangial deposits of IgM precede, and probably lead to, glomerular lesions, 11 other have suggested that IgM deposits are independent from the glomerular lesion. 4
Kashgarian 17 and Rotter 28 support the concept of the mesangium as a specialized extracellular space that is constantly perfused by macromolecules and filtration residues (IgM) by virtue of its relationship with glomerular capillaries.
Deposits of IgM in S. boliviensis in this study were not necessarily present as immune complexes or associated with complement, as no electron-dense deposits in the mesangium or in the basement membrane of the capillary walls were recognized on ultrastructural examination.
Two cases of proliferative GN, both associated with IgM deposits, were found in this study. All glomeruli were thoroughly affected. The Bowman space had disappeared, and the capillary lumen was narrowed because of endothelial and epithelial cell proliferation. In human beings, proliferative processes are accompanied by enlargement of the glomerular capillary tuft and expansion of Bowman's capsule. 3 This glumerulopathy is preceded by upper respiratory tract or skin infections caused by certain strains of group A beta-hemolytic streptococci. 26 Proliferative GN in S. boliviensis in this study may have occurred as a consequence of subclinical ascendant infection of the urinary tract.
Membranous GN was the least frequently observed lesion. Thickening or doubling of the basement membranes was observed using impregnation techniques. These lesions were associated with an increase in the mesangial matrix and the presence of IgM deposits on the basement membrane. In human beings, membranous GN is considered the most severe glomerular change. It can be immunologically mediated, idiopathic, or secondary to systemic disease or immune deficiency states. 18 22 24
Histopathological examination of the biopsies in this study demonstrated that most of them presented varying degrees of glomerular lesions. Immunohistochemical techniques demonstrated that the deposits of IgM in S. boliviensis have a standard mesangial distribution and are mostly related to glomerular lesions characterized by an increase of mesangial matrix.
The presence of IgM in the mesangial matrix and the basement membrane and the absence of electron-dense deposits indicate that glomerular lesions are not immune mediated and probably are not related to IgM.
Footnotes
Acknowledgements
We thank Francisca Morales and Ramón Romero from the Argentinean Primate Center for their excellent technical assistance. We also thank Dr. Miguel A. Petruccelli, Faculty of Veterinary Sciences, National University of La Plata, for the electronic microscopic examinations. We are also grateful to Dr. María Cecilia Castellano for the English-language revision and for her critical reading of the manuscript.