
Abstract
Ganglion cysts were diagnosed in a 4-month-old male Afghan Hound. Grossly, the subcutaneous ovoid cysts around the caudal right elbow joint and left ischiatic tuberosity had abundant mucinous fluid and internal folding. The lesions recurred twice around the elbow joint after surgical removal. Neither cyst communicated with the joint cavity. Histologically, the cyst wall consisted of inner myxomatous and outer immature connective tissue. Some parts of the cyst wall had various stages of myxoid metaplasia of collagen tissue leading to new cyst formation. Ultrastructural study revealed that cells in the myxoid metaplastic lesion had well-developed cytoplasmic secretory elements, including abundant rough endoplasmic reticulum, Golgi apparatus, and many smooth-walled vesicles. These ganglion cysts apparently resulted from the metaplasia of fibroblasts to secreting cells.
Keywords
Ganglion cysts containing mucinous fluid arise from various sites but usually are in close proximity to joints and tendon sheaths. 1 , 5 , 6 , 8 These lesions are extremely rare in animals in comparison to their occurrence in human beings. 8 Although some hypotheses concerning the origin of ganglion cysts have been proposed in human pathology, 1 , 3–5 there is still no consensus on the genesis of these lesions.
The veterinary literature does not contain detailed histologic descriptions of ganglion cysts, including ultrastructural changes. Here, we describe the histologic lesion development and ultrastructure of ganglion cysts in a juvenile dog.
In 15 July 1994, a 4-month-old male Afghan Hound was admitted to the local animal hospital in Sapporo with a 2-week history of a progressively enlarging swelling in subcutaneous tissues around the caudal right elbow joint. Mucosanguineous fluid was dripping from the swelling. The lesion was not painful except on vigorous palpation. When the lesions were removed surgically on 25 July, a 2.5- × 2.0- × 2.0-cm cyst was found in the subcutaneous tissues. The cyst was attached to the caudal olecranon but was not connected to the joint cavity or tendon sheaths. After surgery, a single growing cyst recurred in subcutaneous tissues around the right elbow joint. On 16 August, the recurrent 2.5- × 2.5- × 4.0-cm cyst was again surgically removed. In 7 December, a single growing cyst was observed in the subcutaneous tissue over the left ischiatic tuberosity. On 16 December, a second recurrence of the cyst on the right elbow was detected in subcutaneous tissues. On 21 December, both cysts around the caudal right elbow joint (2.5 × 2.0 × 2.0 cm) and left ischiatic tuberosity (2.5 × 2.0 × 2.0 cm) were surgically removed. Neither cyst involved the joint cavity or the tendon sheaths. Since the last surgery, recurrence of the cysts has not been observed in any sites during 4 years of follow-up.
All cysts were filled with pale-yellow mucinous fluid and had internal shiny folds in the lining wall (Fig. 1). The dog was healthy at and after surgical operation. All excised tissues were fixed in 10% neutral buffered formalin, embedded in paraffin, sectioned, and stained with hematoxylin and eosin, alcian blue and periodic acid–Schiff (pH 2.5) (AB-PAS), and Masson's trichrome. For transmission electron microscopy, small pieces of the formalin-fixed tissues were transferred to 3% glutaraldehyde—0.1 M phosphate buffer (PB), postfixed in 1% osmium tetraoxide—0.1 M PB, and embedded in Quetol (Epon 812). Ultrathin sections were double stained with uranyl acetate and lead citrate and examined with a JEOL JEM-1210 electron microscope.
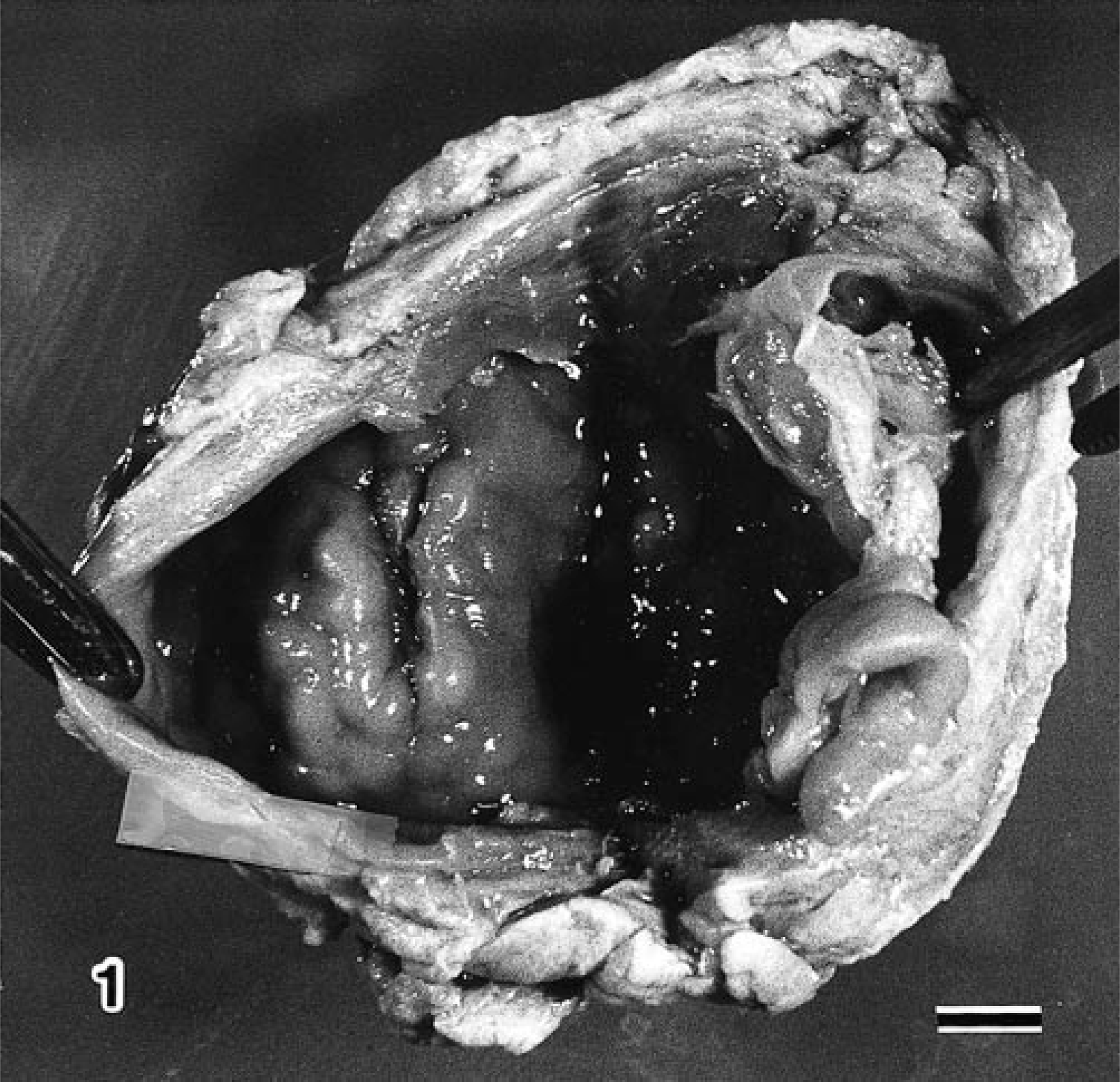
Ganglion cyst; dog. Opened cyst with internal shiny folding in subcutaneous tissue around caudal elbow joint. Bar = 0.5 cm.
Microscopic examination of multiple cross sections of the cysts showed that the wall of the cyst was composed of inner myxomatous and outer fibromatous areas (Fig. 2). Inner myxomatous areas consisted of pleomorphic stellate and spindle cells distributed haphazardly through an abundant myxoid stroma. These cells had moderate eosinophilic cytoplasm and pleomorphic nuclei with a small nucleus. The lining cells of the inner cyst wall were fibroblasts. Overall cellularity was moderately low. Mitotic figures were very rare (less than one per 10 high-power fields). The outer layer of the cysts was similar to immature granulation tissue and was composed of spindle fibroblasts arranged haphazardly in a moderately collagenous stroma (Fig. 2). Overall cellularity was moderately high, and mitotic activity was very low (less than one per 15 high-power fields). Well-developed tortuous capillary channels were distinct. At the base of all the ganglion cysts, the wall was in contact with the bone but had not destroyed its structure.
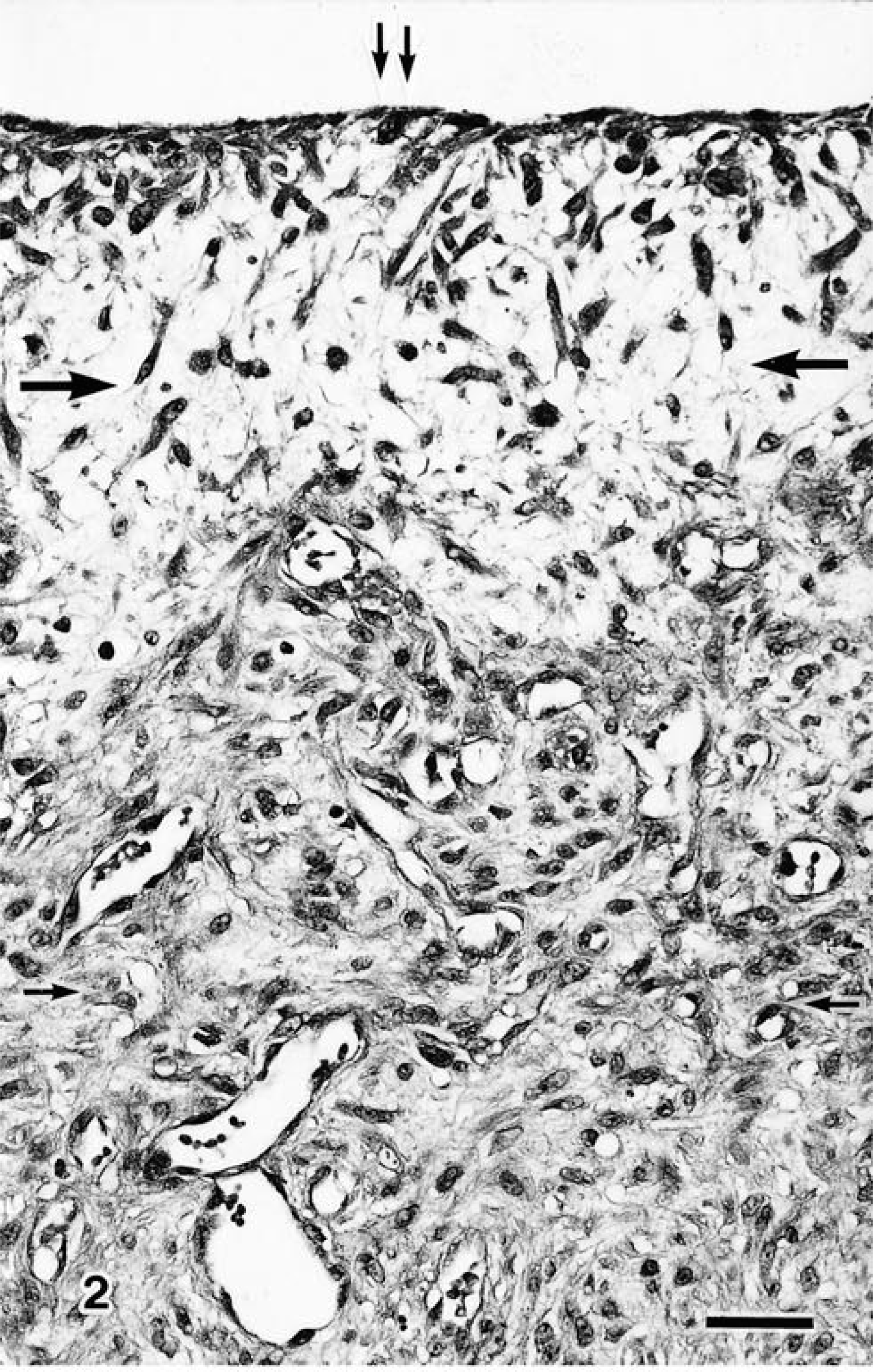
Ganglion cyst; dog. Cyst consists of inner myxomatous (large arrows) and outer fibrous (small arrows) connective tissue areas. There are no true lining cells (double small arrows). Note well-developed tortuous capillary channel. HE. Bar = 40 µm.
The various stages of myxoid metaplasia leading to cyst formation were observed between the outer cellular areas of cysts and the subcutaneous connective tissues (Fig. 3). In the initial phase, mild myxoid metaplasia was observed in collagen tissue. In the initial lesions, there was a central collagen core, which stained blue with Masson's trichrome and was surrounded by swollen fibroblastic cells (Fig. 3). In the next phase, the size of the myxoid area increased and a smaller cystic cavity appeared within the myxoid lesion (Fig. 3). The cavities gradually increased in size and then became completely cystic (Fig. 3). Both the myxoid lesions and the content of the cavities stained blue (acid mucin) with AB-PAS stain.
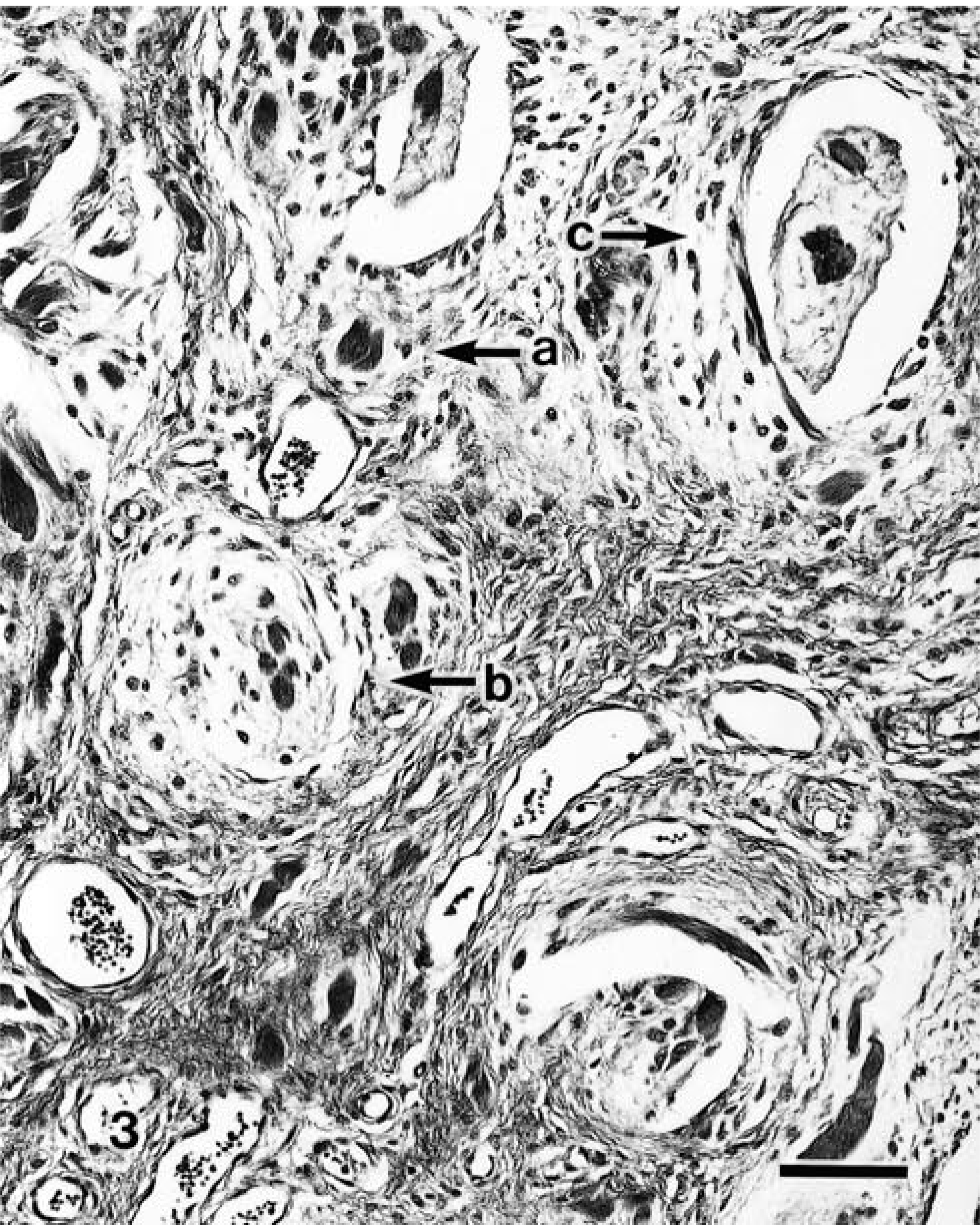
Ganglion cyst; dog. The various stages of myxoid metaplasia leading to cyst formation: mild myxoid metaplasia foci (arrow a) around collagen core, moderate myxoid metaplasia with small cyst cavity (arrow b), and complete cyst cavity (arrow c). HE. Bar = 80 µm.
Electron microscopy revealed abundant rough endoplasmic reticulum (rER) and Golgi apparatus and a few mitochondria in the cells in the inner myxomatous lesions and foci in various stages of myxoid metaplasia (Fig. 4). Degenerative ganglion cells often were observed in the inner myxomatous lesions and were characterized by marked dilatation of the rER and Golgi apparatus, which contained fine granular materials (Fig. 5). There were variable numbers of small to medium-size spherical smooth-walled vacuoles containing a dense granular material in the cytoplasm. Some filopodia were observed on the cell surface. A few cytoplasmic filaments, usually in longitudinal orientation, were occasionally observed. The shape of the nuclei in these cells was moderately irregular. The nuclear chromatin was marginated along the nuclear membrane. The lining of the cyst wall consisted of fibroblastic cells as above mentioned. The intercellular matrix revealed characteristic changes. Bundles of collagen fibrils were visible adjacent to the fibroblasts in the initial phase of the mucinous lesions. As the lesion progressed, collagen fibrils were broken and shortened and arranged haphazardly. Amorphous fine granular materials were observed in the intercellular matrix.
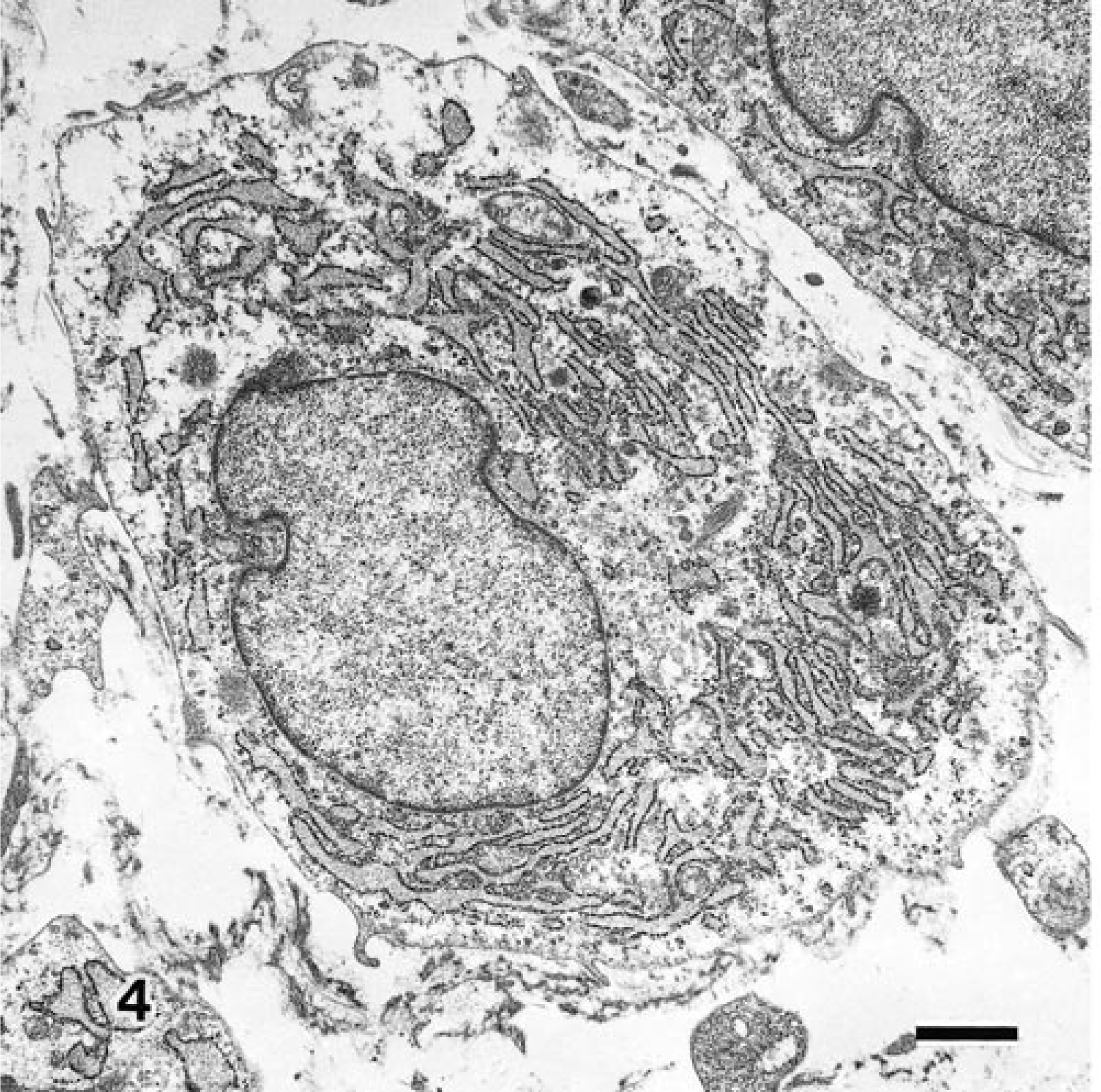
Transmission electron micrograph. Ganglion cyst; dog. Ganglion cell with well-developed rough endoplasmic reticulum. Uranyl acetate and lead citrate. Bar = 1.6 µm.
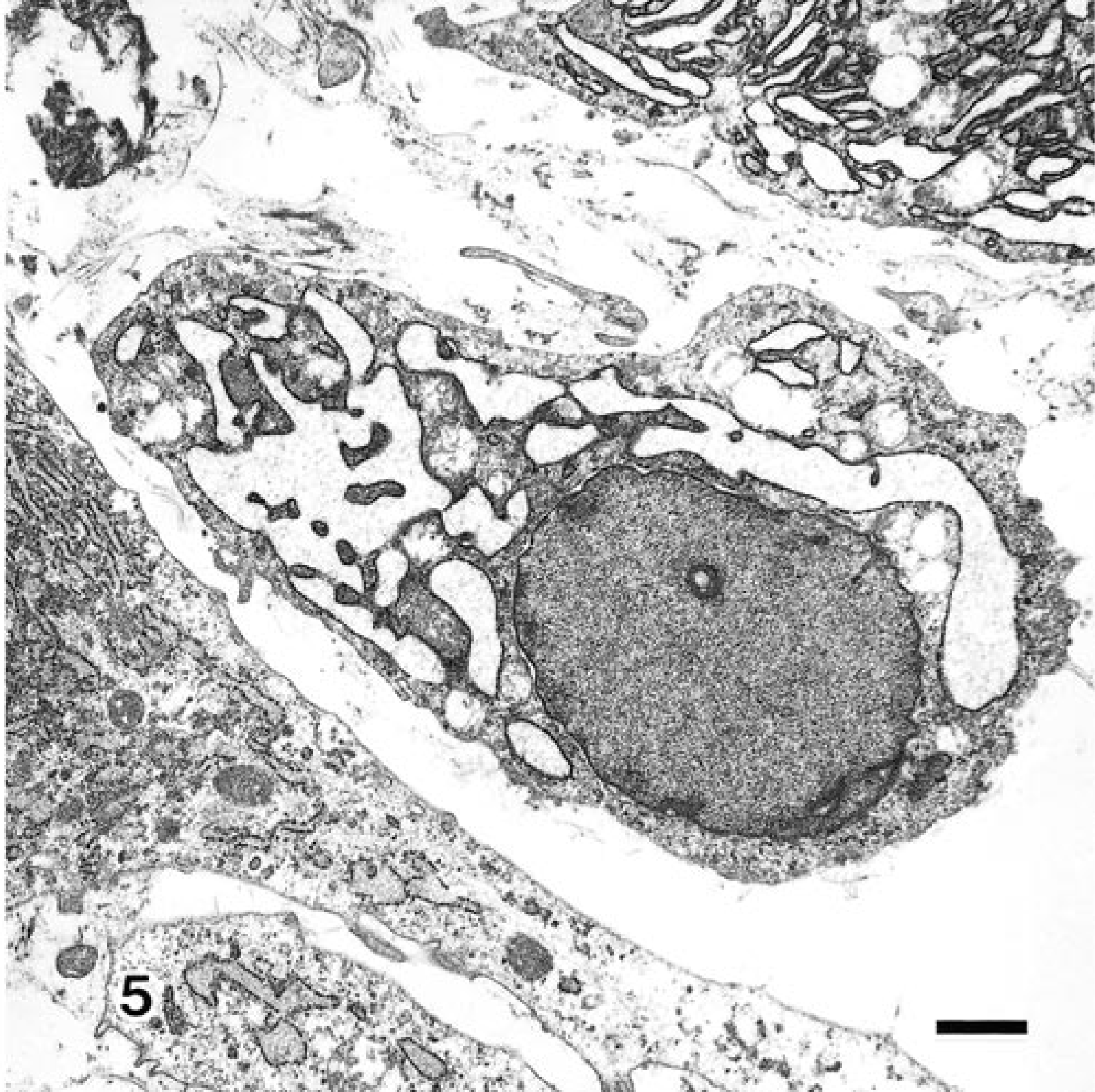
Transmission electron micrograph. Ganglion cyst; dog. Degenerative ganglion cell with marked dilatation of Golgi apparatus, which has fine, dense granular material. Uranyl acetate and lead citrate. Bar = 1.6 µm.
From the histologic and ultrastructural features observed here, the present cysts were diagnosed as ganglion cysts. The cysts revealed neither apparent synovial lining cells in the multilocular cyst walls nor communication with the joint cavity. The present ganglion cysts, therefore, can be differentiated from synovial cysts and adventitious bursae because they lack synovial lining cells and have no communication with the joint cavity. 6 In addition, these ganglion cysts differ from tumors of myxoid or synovial cells because those tumors rarely form cysts. 6
The pathogenesis of the ganglion cyst is obscure. This cyst is thought to arise from mucinous degeneration or metaplasia of fibroblasts to secreting cells. These changes take place in the connective tissue adjacent to a tendon sheath or a joint capsule. 1 , 3–5, 7 The formation of cysts of various sizes observed in the wall of the lesions seen here is of interest. Initially the mucinous lesion was observed among the fibroblastic cells that surrounded a central collagen core. As the lesion progressed, the cysts occurred in the mucinous lesions. The cells surrounding the central collagen core in the initial mucinous lesions seem to be fibroblasts, which are active collagen-secreting cells. Ultrastructural findings in our study revealed also that the cells in the cyst wall were similar to fibroblasts and synovial cells. Ultrastructurally, synovial membrane consists of two cell types: type A cells are phagocytic and contain numerous large vacuoles, branched aperiodic fibrils, filopodia, vesicles, and mitochondria, and type B cells appear to be adapted for protein production and contain abundant rER, a few mitochondria, and occasional vacuoles and vesicles. 7 The cells in the ganglion cyst wall were very similar to type B synovial cells and fibroblasts. It is difficult to distinguish synovial cells from fibroblasts by electron microscopy only. Other researchers have shown that the metaplastic fibroblasts in the ganglion cysts share morphologic features with synovial cells. 2 This finding suggests that histologically myxomatous lesions in collagen tissues around the cysts and cyst formation may result from the secretion of metaplastic fibroblasts. This finding supports conclusions by previous workers, 1 , 4 who described how the fibroblasts underwent metaplasia to secreting cells in ganglion cysts.
In the case presented here, recurrence of ganglion cysts was seen in the subcutaneous tissue around the caudal elbow joint. The recurrence may be due to incomplete surgical excision as previously described. 9
Although the etiology of ganglion cyst is still obscure, trauma has been suggested as one of the inciting factors. 3 In this dog, ganglion cysts appeared at sites that easily contact the ground. Repeated contact may have caused trauma, which led to the formation of ganglion cysts in this dog.